-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Obstetrics and Gynecology
p-ISSN: 2326-120X e-ISSN: 2326-1218
2016; 4(1): 7-10
doi:10.5923/j.rog.20160401.02

Angiotensin Converting Enzyme Insertion/Deletion (I/D) Polymorphism and Risk of Recurrent Pregnancy Loss among Sudanese Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAisha Mahmood Fageer Hussian, Nasr Eldeen Ali Mohammed, Mohanad Altayeb Mohamed Ahmed, Elshazali Widaa Ali
Department of Hematology, Faculty of Medical Laboratory Sciences, Al Neelain University, Khartoum, Sudan
Correspondence to: Elshazali Widaa Ali, Department of Hematology, Faculty of Medical Laboratory Sciences, Al Neelain University, Khartoum, Sudan.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

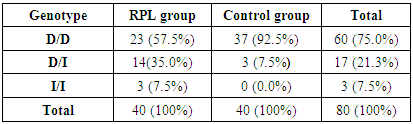
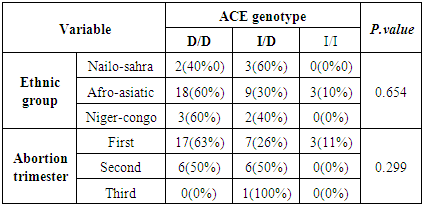
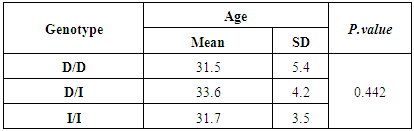
Recurrent pregnancy loss (RPL) is a common clinical problem, and for most women the cause is never discovered. Angiotensin-converting enzyme (ACE) affects vascular structure and placental function, and its role in blood pressure regulation and electrolyte balance is well documented. Furthermore, ACE influences the fibrinolytic balance at a central point by converting angiotensin I to angiotensin II, which increases plasminogen activator inhibitor-1 (PAI-1) activity. This study aimed to investigate the association between ACE insertion/deletion (I/D) polymorphism and RPL among Sudanese women. A total of 80 women were enrolled in this study, 40 with RPL and 40 healthy fertile women-with at least one successful pregnancy and had no history of abortion or any abnormal pregnancy outcome-as a control group. Salting out method was used for DNA isolation from peripheral blood leukocytes, and ACE polymorphic genotypes were determined using polymerase chain reaction (PCR). The frequency of ACE genotypes was found to be 57.5% for D/D, 35.0% for I/D, and 7.5% for I/I in the RPL group, and 92.5% for D/D, 7.5% for I/D, and 0.0% for I/I in the control group. There was statistically significant association between RPL and the genotype (OR: 6.641, 95% CI: 1.732-25.465, P.value: 0.003). There was no statistically significant correlation between ACE I/D polymorphism and each of ethnic origin (P.value: 0.654) and abortion trimester (P.value: 0.299). Comparison of mean age among different genotypes showed no statistically significant difference (P.value:0.442). In conclusions, the ACE I/D Polymorphism exhibits a statistically significant association with RPL among Sudanese women.
Keywords: Angiotensin- converting enzyme, Polymorphism, Recurrent pregnancy loss
Cite this paper: Aisha Mahmood Fageer Hussian, Nasr Eldeen Ali Mohammed, Mohanad Altayeb Mohamed Ahmed, Elshazali Widaa Ali, Angiotensin Converting Enzyme Insertion/Deletion (I/D) Polymorphism and Risk of Recurrent Pregnancy Loss among Sudanese Women, Research in Obstetrics and Gynecology, Vol. 4 No. 1, 2016, pp. 7-10. doi: 10.5923/j.rog.20160401.02.
Article Outline
1. Introduction
- Recurrent pregnancy loss (RPL) refers to the consecutive loss of three or more clinically recognized pregnancies prior to the 20th week of gestation [1]. RPL is a major health problem that affects up to 5% of women of reproductive age [2]. Different etiological factors can lead to spontaneous RPL including anatomical, endocrinologic, hematologic, immunologic and genetic abnormalities of the parents. Nevertheless, half of the RPL cases remain unexplained [3].Successful pregnancies require an even balance of coagulation and fibrinolysis, inorder to secure stabilization of the basal plate as well as adequate placental perfusion [4]. Angiotensin-converting enzyme (ACE) probably influences the fibrinolytic balance at a central point by converting angiotensin I to angiotensin II, which increases PAI-1 activity. In addition, ACE degrades bradykinin, an important mediator of the tissue type plasminogen activator (t-PA), which also contributes to decrease fibrinolysis, hence increasing the thrombotic risk [5]. The ACE gene polymorphism was first reported by Rigatetal, consisting of the presence (insertion-I) or absence (deletion-D) of a 287 pb fragment, at the angiotensin Iconverting enzyme gene (intron 16). Accordingly, three genotypes canresult: II, DD and ID [6]. The ACE I/D polymorphism has been reported to be associated with RPL, especially the number of D allele, and it is a main risk factor for RPL in Asia and Asian populations, as well as in Caucasians [7].The aim of this study was to investigate the association of ACE I/D polymorphism with RPL among Sudanese women.
2. Materials and Methods
- This case-control study was conducted at Khartoum state hospitals during April 2014. A total of 40 women with RPL were enrolled in this study. All the selected women were in the child-bearing age, experienced three or more consequent abortions with no apparent cause; women with a significant medical history such as presence of uterine structural anomalies, endocrinal disorder, diabetes, chronic hypertension, and cardiac disorders were excluded from the study. Furthermore, a total of 40 women with at least one or more successful pregnancy, and had no history of abortion or any abnormal pregnancy outcome were also enrolled in this study as a control group.
2.1. Sample Collection and DNA Extraction
- Blood samples (each 5mL) were collected from each participant in ethylene diamine tetra acetic acid (EDTA) blood tubes and DNA was extracted from peripheral blood leukocytes using salting out method.
2.2. Polymerase Chain Reaction (PCR)
- The insertion/deletion genotyping was performed by PCR (TECHNE, TC412, UK). The reaction mixture (20μL) contained 1μL of each of the forward primer (5’CTGGAGACCACTCCCATCCTTTCT-3’), reverse primer (5’GATGTGGCCAT-CACATTCGTCAGAT-3’), and internal primer (5’TGGGATTACAGGCGT- GATACAG-3’), 2μL of genomic DNA, 10μL sterile distilled water and5μL master mix (Maxime PCR pre mix Kit (I-TAQ), INTRON, KOREA).The amplification program included initial denaturation at 94ºC/3 min; then 30 cycles, each consist of [94ºC/1 min, 52ºC/1 min, and 72ºC/1 min]; then final extension at 72ºC/5 min. PCR products were electrophoresed on 2% agarose gel containing ethedium bromide and the fragments sizes were determined using 50 bp DNA ladder (SOLIS BIODYEN, ESTONIA) and analyzed under UV transilluminator (SYNGENE, JAPAN). A PCR product of 190 bp fragment was consistent with D allele, while a product of 490 bp fragment was consistent with I allele.
2.3. Statistical Analysis
- Data was analyzed by statistical package for social sciences (SPSS), version 18. Correlation between categorical variables was tested by Chi-Square test. Regression analysis was used to investigate the association between the disease and genotypes. The Hardy–Weinberg equilibrium was tested by a goodness-of-fit X2 test to compare the observed genotypic frequencies in normal individuals to the expected genotypic frequencies calculated from the observed allelic frequencies.
2.4. Ethical Considerations
- This study was approved by the scientific research committee of the faculty of medical laboratory sciences, Al Neelain University, and informed consent was obtained from each participant before sample collection.
3. Results
- A total of 40 Sudanese women with RPL and 40 healthy women (control group) were enrolled in this study to verify whether there is an association between ACE I/D polymorphism and RPL among Sudanese women or not. Mean age of women with RPL was 32.3 years and of the control group was 30.9 years.The frequencies of ACE genotypes were found to be 57.5% for DD, 35.0% for ID, and 7.5% for II in the RPL group, and 92.5% for DD, 7.5% for ID, and 0.0% for II in the control group (Table 1).
|
|
|
4. Discussion
- The present study was conducted in Khartoum state, Sudan, to explore the association of ACE I/D polymorphism with RPL among Sudanese women.The results showed that, the D/D genotype was the most frequent among both patients and control groups, followed by I/D and I/I genotypes consequently.The studies concerning with ACE I/D polymorphism in recurrent abortion in different populations showed conflict results. Al Sallout et al., studied ACE polymorphism in 100 women with RPL and 100 healthy women and found that DD>ID>II in both patients and control groups [8]. On the other hand, Buchholz et al., and Goodman et al., found that ID>DD>II, and Vettriselvi et al., reported that II>ID>DD [9-11]. The result of the present study revealed statistically significant association between ACE I/D genotype and RPL in Sudanese women, and the risk of RPL increased about 6 folds in those with the genotype I/D.This finding is agrees with that of Bukreeva et al., who concluded that, the ACE I/D genotype exhibits a statistically significant association with a history of foetal loss [12]. This finding was more supported by studies available in meta-analysis by Yang et al., who demonstrated that, the ACE I/D polymorphisms is associated with RPL susceptibility, especially the number of D allele, which is the main risk factor for RPL in Asia and Asian populations, as well as in Caucasians [7]. Goodman et al., and Shakarami et al., reported no significant association between ACE D allele or DD genotype and RPL [10, 13]. A possible reason for inconsistency among these the mentioned studies may be genetic basis that causes different susceptibilities among different populations or differences in patients’ selection criteria.There was no statistically significant correlation between ACE genotypes and each of ethnic group, and abortion trimester. Furthermore, no statistically significant difference was found in mean age among different ACE genotypes. Similar results were reported by Mello et al., who found no differences in maternal age, parity, gravidity, and body mass index among the groups classified according to ACE I/D genotypes [14].The frequency of the D allele was 0.60 in women with RPL and 0.77 in the control group, while the frequency of the I allele was 0.40 in the in women with RPL and 0.23 in the control group. Yang et al., reported that, the frequency of the D allele in women with RPL in Asian and Caucasian populations was 71.0%, 59.55, and 51.6% [7]. However, in this study, no significant deviation from Hardy-Weinberg equilibrium was found in both RPL group and the control group.
5. Conclusions
- This study showed a significant association between the ACE I/D Polymorphic genotype and RPL among Sudanese women.