-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Obstetrics and Gynecology
p-ISSN: 2326-120X e-ISSN: 2326-1218
2015; 3(2): 17-21
doi:10.5923/j.rog.20150302.02
Comparison of the Effect of Acupressure at Yong Quan (KI-1) and Hegu (LI-4) Acupoints on Pain Intensity of Labor Pain in Primiparous Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaasumeh Kaviani1, Nasim Partash2, Sara Azima1, Mohammad Javad Hadyanfard3, Mehrab Sayadi4
1Department(s) and Institution(s) Department of Midwifery, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran
2Department(s) and Institution(s) Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran
3Departement(s) and Institution(s) Assistant Professor, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
4Department(s) and Institution(s) Msc, Department of Biostatistics, School of Public Health, Behbahan University of Medical Sciences, Behbahan, Iran
Correspondence to: Maasumeh Kaviani, Department(s) and Institution(s) Department of Midwifery, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Labor is a very important experience in women’s life whose quality has both short- and long-term effects. Fear and anxiety due to delivery increase women’s pain and discomfort in the delivery room. The present study aimed to assess the effects of acupressure at KI-1 and LI-4 acupoints on the intensity of labor pain. This interventional clinical trial was conducted on 78 primiparous women (52 in the intervention groups and 26 in the control group) referring to Hafez and Zeinabiyeh hospitals, Shiraz, Iran. The participants were in the 37th week of gestation and their cervical dilation was 3-4 cm. Based on the medical records, the participants suffered from no diseases and were physically healthy. Also, they had received no drugs during labor. The intervention groups’ participants received acupressure at KI-1 and LI-4 acupoints at 3-4 and 7-8 cm dilations and the second stage of labor for 10 minutes. However, the control group subjects underwent no interventions. The participants’ intensity of pain was measured using Visual Analogue Scale (VAS) before and after the intervention. The results showed no significant difference among the three groups regarding the intensity of pain. However, a significant difference was observed among the three groups in this regard immediately, 30 minutes, and 60 minutes after application of acupressure (P<0.001); such a way that pain intensity was higher in the intervention groups compared to the control group. Also, a significant difference was observed among the three groups with respect to the intensity of pain in the second stage of labor. The study results showed that acupressure at KI-1 and LI-4 acupoints was effective in the intensity of labor pain. Thus, this is simple, non-invasive, safe, and inexpensive method can be effective in reduction of labor pain.
Keywords: Pain intensity, Labor pain, Yong Quan acupoint, Hegu acupoint, Primiparous women
Cite this paper: Maasumeh Kaviani, Nasim Partash, Sara Azima, Mohammad Javad Hadyanfard, Mehrab Sayadi, Comparison of the Effect of Acupressure at Yong Quan (KI-1) and Hegu (LI-4) Acupoints on Pain Intensity of Labor Pain in Primiparous Women, Research in Obstetrics and Gynecology, Vol. 3 No. 2, 2015, pp. 17-21. doi: 10.5923/j.rog.20150302.02.
Article Outline
1. Introduction
- Labor is a very important experience in women’s life whose quality has both short- and long-term effects. Negative labor experiences lead to psychological and sexual disorders and affect the emotional relationships between mother and her child after delivery. On the other hand, fear and anxiety resulting from labor pain increase the rate of surgical interventions. Thus, in order to decrease the rate of these interventions, fear and anxiety due to labor pain should be changed into a desirable experience [1-3]. Labor is most probably painful and labor pain is a convincing alarm that the pregnant mother should be in a healthy and safe place [1]. Evidence has indicated that fear and anxiety resulting from labor increased the women’s pain and discomfort in the delivery room [4]. Although delivery is a natural physiological process, most pregnant women are highly concerned and anxious about labor pain during their pregnancy period [5]. Labor pain leads to an increase in oxygen consumption followed by hypoventilation, hypocarbia, increase in respiratory alkalosis, involuntary stimulation, and catecolamins secretion, leading to increase of gastric acid, increased peripheral vascular resistance, reduction of placenta perfusion, fetal hypoxia, abnormal fetal heart rate, reduction of Apgar score, metabolic acidosis, uncoordinated uterine response, delay in gastric emptying, inefficiency of uterine contractions, and long delivery process, eventually resulting in obstetrics interventions and their resultant complications [6, 7]. U.S. College of Nursing and Midwifery in 2003 announced that 1 out of every 4 deliveries was carried out through cesarean section, the most important reason of which being fear from pain resulting from natural vaginal delivery. This has been mentioned by World Health Organization (WHO) as an alarm for the obstetrics society [7]. According to the statistics provided by the College of Nursing and Midwifery of Shiraz University of Medical Sciences, the rate of cesarean delivery was 49% in Shiraz, 48% in Fars province, and 45% in Iran in 2008. Yet, WHO has announced that nearly 15% of all deliveries in each region can be carried out through cesarean section by correct indications. However, the rate of cesarean delivery is various and ever increasing in different parts of the world; such a way that it has increased from 5% to 25% in the recent 20 years [8]. On the other hand, tolerating labor pain, particularly in primiparous women, creates an undesirable experience for them, affects their decision for their further deliveries, and increases their tendency toward cesarean delivery. In comparison to natural vaginal delivery, cesarean section can increase the risk of wound infection, bleeding, urinary tract infection, and thromboembolism in the mother. Studies have also indicated that cesarean delivery could have impacts on future deliveries, breastfeeding, the relationship between the mother and her child, and postpartum depression [9-12].In general, three main bases in relieving pain in obstetrics issues are simplicity, safety, and maintenance of fetal homeostasis, which are also the features of the best anesthetic drugs in gynecology and obstetrics. These drugs should, in fact, be efficient against pain, should not intervene in the natural process of delivery, and should not have negative effects on fetus’ respiratory and blood circulation systems [13]. Overall, labor pain relief methods are divided into two categories, namely pharmacological and non-pharmacological methods. Pharmacological methods include epidural anesthesia, opioids, and respiratory gasses such as N2O. In spite of these methods’ desirable effects on labor pain, they have potential side effects on both mother and fetus. On the other hand, non-pharmacological methods include acupuncture, acupressure, Lamaze breathing techniques, hypnotism, music therapy, hydrotherapy, thermotherapy, and Cryotherapy. These methods are usually simple and inexpensive and can be used either as replacement therapy or in combination with drugs. Acupuncture and acupressure are among the non-pharmacological methods which have attracted a lot of attention these days. WHO has approved application of acupuncture and acupressure in 100 Cases.Acupressure is a kind of skill in traditional medicine in which fingers are employed to apply pressure on the key points on the skin for stimulation and induction of body’s self-treatment abilities. Chinese traditional medicine indicates that human body consists of 14 meridians or canals in which life energy known as “qi” is flowing [14]. This energy, including positive (Yang) and negative (Yin) forms, is normally balanced in the body, and any disorder or imbalance in these two energies would lead to the incidence of diseases. With regards to practical and clinical perspective, acupressure is non-invasive, does not require specific instruments, is inexpensive and accessible, and can be taught to the patients simply. Nowadays, acupressure is considered as one of the branches of community-based health sciences. It is also considered as one of the complimentary medicines in which application of gentle and stable pressure on one or some of the 365 energy points on the 12 paths leads to release of energy in that path [15].
2. Materials and Methods
- This interventional clinical trial was conducted on 78 primiparous women who were in the 37th week of gestation at 3-4 and 7-8 cm cervical dilation and the second stage of delivery. According to the medical records, the study participants had no special diseases during pregnancy, were physically healthy, and had used no anesthesia or analgesic methods during labor. Using the table of random numbers, the study participants were divided into two intervention groups (N=52) and a control group (N=26). Then, the participants were equally explained about the interventions and written informed consents were obtained from them.The participants’ intensity of pain was measured using Visual Analogue Scale (VAS). This instrument is like a ruler numerated from 0 to 10, representing no pain and the most intolerable pain, respectively.At the beginning of contractions at 3-4 cm dilation, the intensity of pain was measured using VAS before and immediately, 30 min, and 60 min after the intervention. At this stage, pressure was applied at the beginning of each uterine contraction for 10 min. The intervention was also continued at 7-8 cm dilation and the second stage of labor. In doing so, the researcher applied pressure by the right hand on Yong Quan acupoint (KI-1, on sole, at the junction of the anterior 1/3 and posterior 2/3 of the line connecting bases of the second and third toes with the heel) on the mother’s right foot; such a way that the area around the pressed point turned into white.In the other intervention group also, the researcher applied pressure by the right hand on Hegu acupoint (LI-4, on the dorsum of the hand between the first and second metacarpal bones, in the middle of the second metacarpal bone on the radial side) on the mother’s left hand. The applied pressure was equal to 3-3.5 kg which was learned by the researcher using a bathroom scale before beginning of the study. In the control group, however, no intervention was performed.After all, the data were analyzed using the SPSS statistical software (v. 16) and P<0.05 and P<0.16 were considered as statistically significant. Kruskal-Wallis test was used to compare the intensity of pain among the three groups before and after the intervention. Besides, Mann-Whitney test was used to compare the pain intensity in each of the three groups.
3. Results
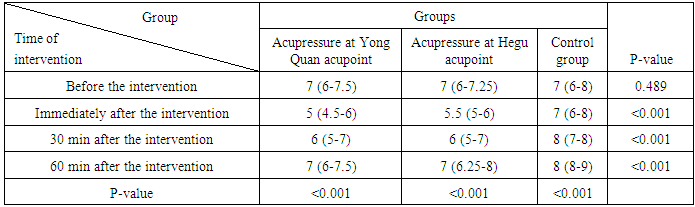
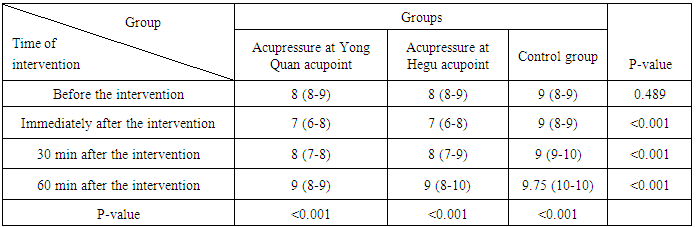
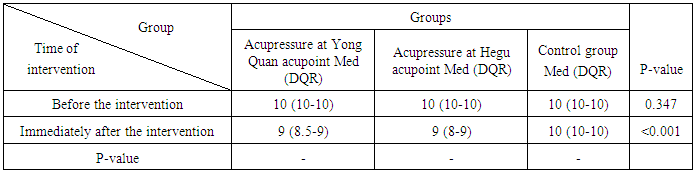
- This study was conducted on 78 primiparous women, 52 in the intervention groups and 26 in the control group. The results revealed no significant difference among the three groups regarding the intensity of pain before the intervention. At the beginning of uterine contractions, the intervention groups’ participants underwent acupressure for 10 min and the intensity of pain was measured immediately, 30 min, and 60 min after the intervention. Based on the results presented in Table 1, the intensity of pain significantly decreased in the intervention groups compared to the control group after application of acupressure at 3-4 cm dilation (P<0.001). Also, as Tables 2 and 3 depict, a significant difference was found among the three groups regarding the intensity of pain at 7-8 cm dilation (P<0.001) and the second stage of labor (P<0.001). However, the results showed no significant difference between the two intervention groups with respect to the pain intensity at 3-4 and 7-8 cm dilation and the second stage of labor immediately, 30 min, and 60 min after the intervention.
4. Discussion
- Difficulty of tolerating labor pain is undeniable. Labor pain is one of the most intense pains; thus, women in developing countries resort to cesarean section for reducing this pain. Recently, due to progress in complementary medicine, acupressure has attracted a lot of attention in obstetrics and has led to development of novel skills in pregnancy cares [16] which can reduce the use of analgesic drugs during labor.In the present study, acupressure as a non-pharmacological method was assumed to decrease labor pain. Hence, the effect of acupressure on the intensity of labor pain was investigated.The study results revealed that the intensity of pain decreased in the intervention groups after application of acupressure, but increased in the control group which received no interventions (Tables 1, 2, and 3).
|
|
|
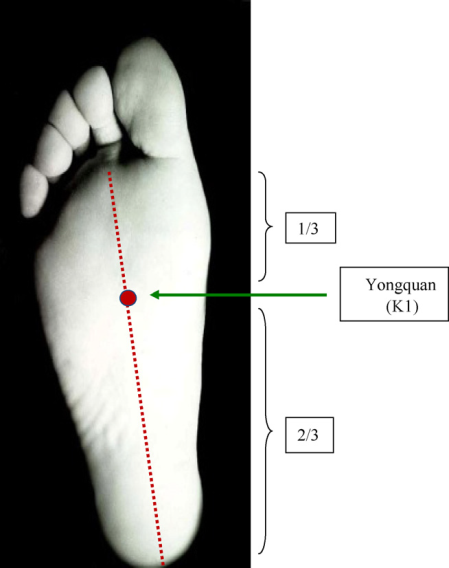 | Figure 1. Yong Quan acupoint (KI-1) |
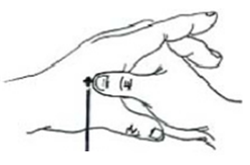 | Figure 2. Hegu acupoint (LI-4) |
5. Conclusions
- The findings of the present study showed that acupressure at both KI-1 and LI-4 acupoints was effective in reduction of labor pain during the first and second stages of labor. However, the intensity of pain increased in the control group which had received no interventions. Considering the simplicity, safety, and inexpensiveness of acupressure, this method is recommended to be used for reduction of intensity of labor pain.
ACKNOWLEDGEMENTS
- This article was extracted from Nasim Partash's M.Sc. thesis approved by Shiraz University of Medical Sciences (proposal No 92-6612).Hereby, the authors would like to thank the Research Vice-chancellor of Shiraz University of Medical Sciences, personnel of labor departments in Hafez and Zeinabiyeh hospitals, and all the individuals who cooperated in the study. The authors are also grateful for Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for improving the use of English in the manuscript.