-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Obstetrics and Gynecology
p-ISSN: 2326-120X e-ISSN: 2326-1218
2013; 2(3): 31-35
doi:10.5923/j.rog.20130203.03
Sexual Function in Woman with Urinary Incontinence: A Cross- Sectional Study from Iran
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMomenimovahed Zohre1, Pakgohar Minoo2, Montazeri Ali3, Bahiraee Azam4
1Msc of Midwifery Education, Department of Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
2PHD of Gerontology, Department of Gerontological nursing, Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3Professor of Public Health, Mental Health Research Group, Health Metrics Research Centre, Iranian Institute for Health Sciences Research, ACECR, Tehran, Iran
4PHD of Health Promotion, Department of Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
Correspondence to: Pakgohar Minoo, PHD of Gerontology, Department of Gerontological nursing, Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Objective: Urinary incontinence is a common problem throughout the world that affects women from all cultures, ages and ethnic groups. This study aimed to assess the impact of different type of urinary incontinence on sexual function. Methods: This cross-sectional study was performed from April 2012 to October 2012 among women complaining of urinary incontinence who were referred to a large teaching hospital, in Tehran, Iran. Sexual function was measured with Pelvic organ prolapse/ urinary incontinence sexual questionnaire (PISQ). Urinary incontinence was determined with Questionnaire for Urinary Incontinence Diagnose (QUID). Participants were divided into three groups of stress urinary incontinence (SUI), urge urinary incontinence (UUI) and mixed urinary incontinence (MUI) and then sexual function was compared among these groups. Results: In all, 400 women were entered into the study. Among the whole participants, 223 patients (55.8%) complained of SUI, 97 patients (24.2%) of UUI and 80 patients (20%) of MUI. There was significant association between sexual function and type of urinary incontinence (P<0.001). Mixed urinary incontinence had a greater disruptive effect on sexual function compared to other groups. Among other groups, scores in UUI group were lower than SUI. Higher age groups had lower sexual function scores and there were significant differences among age groups (P<0.001). The results obtained from multiple logistic regression analysis showed that the most significant contributing factor to total PISQ scores was age. Conclusions: The findings from this study suggestthat UI affect sexual function and that MUI has a greater effect on sexual function than the other two types of incontinence.
Keywords: Female Sexual Function, Urinary Incontinence, Cross Sectional Study
Cite this paper: Momenimovahed Zohre, Pakgohar Minoo, Montazeri Ali, Bahiraee Azam, Sexual Function in Woman with Urinary Incontinence: A Cross- Sectional Study from Iran, Research in Obstetrics and Gynecology, Vol. 2 No. 3, 2013, pp. 31-35. doi: 10.5923/j.rog.20130203.03.
1. Introduction
- Urinary incontinence (UI) refers to the complaint of involuntary leakage of urine[1]. UI is a common problem throughout the world that affects women from all cultures, ages, and ethnic groups[2]. Overall, 25-45 percent of women complain of some degrees of UI[3]. In general, one out of every five women reports that UI has affected her daily life[4]. Urinary incontinence greatly affects the health - related quality of life[5, 6]. The sexual function, as one aspect of health related quality of life, is impaired in people with urinary incontinence[7,8]. This problem is associated with low libido, vaginal dryness, and dyspareunia[9]. The findings of one study showed that 34 percent of women with UI suffered from low libido, 23% had exciting phase disorder, 11% had orgasmic disorder, and 44% suffered from pain during intercourse[10]. Women, for many different reasons including psychological distress, wetting at night, urine leakage during intercourse, shame, and depression, refuse intercourse[11]. Yip et al reported that the marital relationship and sexual function were negatively affected in woman with UI[12]. The assessment of the sexual function in women with urinary incontinence has been carried out in different studies, but different measurements and designs of the studies have led to conflicting results[13, 14, and 15]. However, many of these studies have used general questionnaires for the assessment of the sexual function and few have investigated the effect of different types of UI and compared them[8, 15]. Therefore, this study aimed to assess the impact of different types of urinary incontinence on the sexual function using the validated and self- administered Pelvic Organ Prolapse and Urinary Incontinence Questionnaire (PISQ) in women complaining of UI.
2. Methods
- Participants and data collectionThis cross-sectional study was performed from April 2012 to October 2012 in a sample of 400 women complaining of urinary incontinence who were referred to Imam Khomeini Hospital, a large teaching hospital affiliated to Tehran University of Medical Sciences. Inclusion criteria for this study were complains of any type of stress (SUI), urge (UUI), or mixed urinary incontinence (MUI) for at least six months, age above the 20 years, being married and sexually active (having intercourse according to the subject`s statement), being able to read and write, and not being pregnant (according to the patient`s statement). People with reversible causes of urinary incontinence, functional disability, mental disorder, and associated diseases (according to the patient`s statement) were excluded.Measures1. Demographic data: Demographic information was collected using a questionnaire that was designed by the researcher. The questionnaire contained items on age, educational level, employment status, height, weight, menopausal status, duration of marriage, number of pregnancies and children, type of delivery, and history of multiple pregnancies. BMI was calculated by the researcher using height and weight.2. Sexual function: Sexual function was measured using the Pelvic Organ Prolapse Urinary IncontinenceQuestionnaire (PISQ). The PISQ is a validated, self-administered and condition-specific questionnaire developed for the measurement of the sexual function in women with urinary incontinence and pelvic organ prolapse. The short form of the questionnaire includes 12 questions and has three main domains: behavioral, emotive, physical and partner related. Each question is rated from 0 (a worse condition) to 4 (a better condition) yielding a total score ranging from 0 to 48[16]. Psychometric properties of the Iranian version of the questionnaire have been well documented[17]. 3. Urinary incontinence: Urinary incontinence was determined using the Questionnaire for Urinary Incontinence Diagnose (QUID); according to this questionnaire, the participants are divided into three groups of stress urinary incontinence, urge urinary incontinence, and mixed urinary incontinence[18].Statistical analysisData were analyzed using SPSS version 16. Descriptive statistics were used to explore the data. The main outcome was a total PISQ score. Comparison among groups was made using the one-way analysis of variance. Also, we performed ANCOVA to compare mean scores among the three groups while adjusting the outcome for age, live child, BMI, and number of pregnancies. In addition, univariate and multivariate regression analyses were performed to assess the association of the independent variables with the sexual function. Multivariate regression logistic analysis was performed to obtain the best model to predict the total PISQ score. P-Values less than 0.05 were considered statistically significant.EthicsTehran University of Medical Sciences ethics committee approved the study and all participants completed an informed consent form prior to inclusion in the study. A private environment was provided for participants to complete the questionnaire and participants were assured of the confidentiality of their information.
3. Results
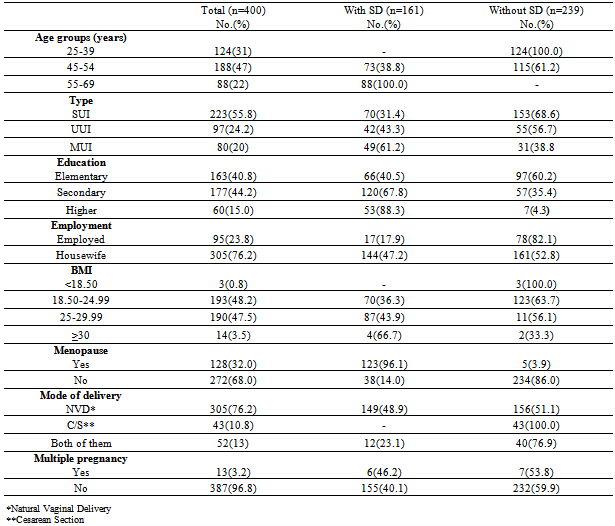
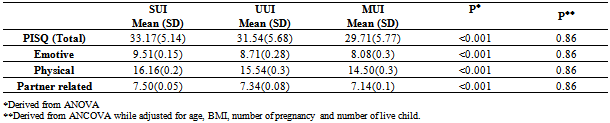
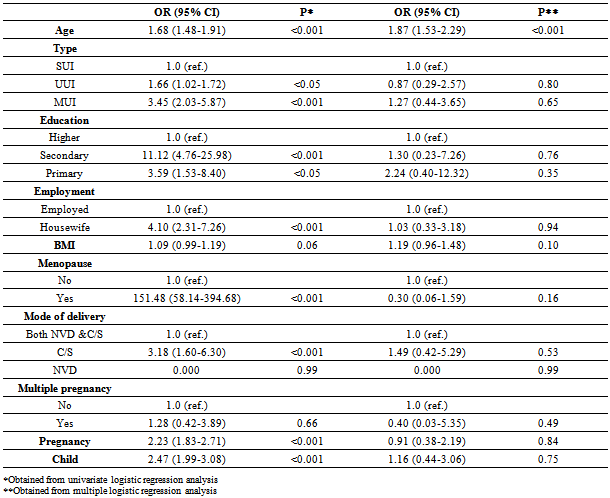
- Demographic characteristics of the study sampleIn all, 400 women complaining of urinary incontinence were included in the study. The mean age of the participants was 46 years (SD=10.13). Of all the participants, 223 (55.8%) complained of SUI, 97 patients (24.2%) of UUI and 80 patients (20%) of MUI. Most women (76.2 8%) were housewives and had primary school education (40.8%). A few participants were underweight or obese. Delivery mode of most women was natural vaginal delivery (76.2%). The majority of the participants were pre-menopausal women (68.0%). The characteristics of the participants are shown in Table 1.Impact of urinary incontinence on the sexual functionTable 2 presents the comparison of PISQ by type of incontinence. There were significant differences in the sexual function among the sub-groups of patients with different types of urinary incontinence (P < 0.001). Mixed urinary incontinence had a greater disruptive effect on the sexual function when compared to the two other groups. Among other groups, mean scores in the UUI group were lower than the SUI group. However, the results obtained from ANCOVA adjusted for age, BMI, and the number of pregnancies and live children showed that there were no significant differences in the sexual function among the study sub-groups (P>0.05).Table 3 shows the relationship between the sexual function and the demographic characteristics of the study samples. The results showed a significant association between the sexual function and age, type of urinary incontinence, educational level, employment, menopausal status, mode of delivery, and the number of pregnancies and live children (P<0.05).
|
|
|
4. Discussion
- This study examined the sexual function in women with urinary incontinence using a standard and condition specific questionnaire. In this study, three groups of SUI, UUI, and MUI were evaluated. Most women complained of stress urinary incontinence (55.8%). The findings of our study revealed that the majority of the women with the complaint of urinary incontinence had a low sexual function. Other studies have also reported that urinary incontinence is associated with sexual dysfunction, but some of them have used condition specific questionnaires[13, 14]. The PISQ has been designed to assess the sexual function in women with urinary incontinence and pelvic organ prolapse in order to better reflect the changes associated with the disease as compared to general questionnaires[16]. Husband sexual dysfunctions can leave a significant effect on the sexual function. Unlike general questionnaires, the partner related domain of this questionnaire gives information about the sexual function of the husband.Although our results showed that MUI affected the sexual function more than other types of urinary incontinence, Lane and Ozel reportd a different conclusion. They found no differences between the impact of the different types of incontinence on the sexual function. The only statistically significant difference in their study was the fact that women with MUI were significantly more likely to be satisfied with the variety of sexual activities[14]. Similarly, Aslan et al found that the sexual function assessed by the female sexual function index (FSFI) did not differ by the type of urinary incontinence, which could be due to the small sample size of the study. They measured the sexual function in 21 premenopausal incontinent women and compared it with the control group[15]. Although FSFI is a valid questionnaire, it may not be sensitive enough to assess the sexual function in incontinent women. Our findings were very similar to a study carried out by Coksuer and colleagues in which they reported that MUI was associated with a lower sexual function than UUI and SUI[13].Yip only studied two groups of UI (SUI and MUI), and reported the negative effect of UI on the sexual function. The sample size of this study was very small. Yip assessed the sexual function in 65 incontinent women in comparison with 26 continent women[12]. Handa et al. did not examine the effects of different types of urinary incontinence on the sexual function but showed that sexual complaints among women 30-60 years had the lowest rate[9]. Sen et al found that MUI had a greater impact on the sexual function as compared to other groups. The sample size was also very small in this study[8].Urinary incontinence is a distressing disorder that can have negative impacts on the sexual function in women[7]. Using a specific questionnaire, the present study showed that sexual dysfunction was common in women with urinary incontinence. Our findings also revealed that MUI had greater negative effects on the sexual function among the different types of urinary incontinence. Various types of urinary incontinence due to different pathologies may leave different effects on sexual function. Because MUI is a combination of SUI and UUI, it may have greater effects on the sexual function. Religious and cultural factors play an important role in the sexual function. Therefore, further studies are required in different societies.There were some strong points to this study. First, we assessed the sexual function with a condition specific and valid questionnaire and second, we compared three groups of UI. Of course, our study had some limitations which need to be addressed. First of all, in this study, we did not include illiterate women and therefore, a number of women who had urinary incontinence but were illiterate were excluded. Second, there was no control group. Including a control group would provide more accurate results. Another limitation of this study was the fact that we carried out the study in a referral center and the results of this study may not be generalized to the general population. Further studies are required to assess the sexual function in different centers. Various treatment methods have different effects on the outcomes and studying the effect of these treatments on the sexual function as a consequence of therapy is also recommended.In conclusion, by using the Iranian version of PISQ, we evaluated the sexual function in women with UI and found that although all types of UI affected the sexual function, MUI had the greatest effect. Therefore, we believe that sexual dysfunction should be considered in women with urinary incontinence and assessed in urogynecology clinics.