-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Obstetrics and Gynecology
p-ISSN: 2326-120X e-ISSN: 2326-1218
2013; 2(3): 28-30
doi:10.5923/j.rog.20130203.02
Utility of Investigative Modalities in Diagnosis of Congenital Anomaly-A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKanica Kaushal1, Sunil Kumar Raina2, Sandeep Moudgil3
1Zonal Hospital, Mandi (Himachal Pradesh), India
2Department of Community Medicine, Dr. RP Government Medical College, Tanda, Kangra (HP), India
3Department of Radio-diagnosis, PGIMER, Chandigarh, India
Correspondence to: Sunil Kumar Raina, Department of Community Medicine, Dr. RP Government Medical College, Tanda, Kangra (HP), India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Introduction: Studies point to presence of single umbilical artery (SUA) as the most common vascular anomaly in humans. Antenatal ultrasound is the imaging investigation of choice and a SUA is often detected incidentally on ultrasound. However is USG, a foolproof modality of diagnosis SUA? Case report: A 25 year old patient G2P1001 reported to the gynecology OPD (GOPD) at the zonal hospital in north western India, on 20th of March 2013 as Post dated pregnancy at 40 weeks and 3 days with no evidence of labour pains. However, a cross section of umbilical cord, revealed 2 umbilical arteries and single umbilical vein. Discussion: The sensitivity, specificity, positive and negative predictive value has been reported at 36%, 99%, 32% and 99% respectively in a study. These results may seem disappointing but do reflect practice in a routine clinical setting where the time allocated to a routine anomaly scan is 15 minutes.
Keywords: Utility, Investigative Modalities, Congenital Anomaly
Cite this paper: Kanica Kaushal, Sunil Kumar Raina, Sandeep Moudgil, Utility of Investigative Modalities in Diagnosis of Congenital Anomaly-A Case Report, Research in Obstetrics and Gynecology, Vol. 2 No. 3, 2013, pp. 28-30. doi: 10.5923/j.rog.20130203.02.
1. Introduction
- Studies point to presence of single umbilical artery (SUA) as the most common vascular anomaly in humans. The reports point to an incidence varying from 0.72% to 0.85%.[1, 2] Further as the single vessel cord is found to be associated with congenital and chromosomal abnormalities, it is of great concern to the parents regarding well being of the baby and to the obstetrician with the management and how to counsel. Single umbilical artery is detected more commonly now in the antenatal period, due to routine anomaly scan advised in the second trimester. About 30 % of all infants with only one umbilical artery had associated congenital anomalies.[3] Antenatal ultrasound is the imaging investigation of choice and a SUA is often detected incidentally on ultrasound. Study in past has claimed that high resolution ultrasound has a sensitivity and specificity approaching 100%.[4] This essentially explains the utility of ultrasound as part of anomaly plan in the antenatal period. But are these anomaly plans and more so the antenatal ultrasound, a foolproof investigative modality for picking up congenital anomalies like SUA?This case report from a zonal hospital in north-western state of India, points to the contrary.
2. Case Report
- A 25 year old patient G2P1001 reported to the gynecology OPD (GOPD) at the zonal hospital in north western India, on 20th of March 2013 as Post dated pregnancy at 40 weeks and 3 days with no evidence of labour pains. The patients had no history of receiving antenatal check up in antenatal period. The details of the patient were, last menstrual period (LMP) on 10th of June 2012 and therefore the expected date of delivery (EDD) as 17th march 2013. The patient was admitted. On clinical examination the patient blood pressure was BP=120/70 mm hg, with a pulse rate of 88/minute. On abdominal examination, height of uterus approximated to full term, Cephalic down, Uterus relaxed, Liquor adequate. Fetal heart sounds were present, regular at 144 beats per minute (bpm).On speculum examination no leakage was found. Per vaginal examination revealed cervix soft central, os closed, uneffaced. On routine investigations, the patient was found to be anemic with Hb at 10g%. Urine routine & microscopy was found to be within normal limits. The patient’s VDRL, HIV and HBSAG were non-reactive.The patient was investigated with USG Doppler and the biophysical profile which revealed a single live intrauterine fetus in longitudinal lie and vertex presentation at the time of examination averaging to 36 weeks 05 days. The estimated fetal weight was around 3.0 Kg+/-460 grams. The fetal cardiac activity was regular at 153bpm (Non reactive, recorded at 163bpm after stimulation). The Amniotic fluid was normal in amount amniotic fluid Index (AFI-70mm). Largest amniotic fluid pocket in left lower quadrant measured approx 3.4 cm in vertical depth. The Placenta was postero-fundic in position & grade 3 in maturity and cervical length approximately 2.1 cm. The Biophysical profile revealed score of 8/10. The fetal Doppler study revealed two vessels pattern with Single Umbilical Artery (SUA) and single umbilical vein. Umbilical artery showed normal flow in diastole with Systolic-Diastolic ratio of 1.6, resistive index (RI) of 0.4 and Pulsatility Index (PI) of 0.5. The Patient was counseled for the associated congenital abnormalities usually associated with Single Umbilical Artery (SUA).Fetal heart sound (FHS) was monitored every four hours. Induction of labor was performed with cerviprim gel on 28th of March 2013 at period of gestation (POG) 41weeks 4 days which failed. Elective Lower segment caesarean section was conducted on 29th of March 2013 and it delivered an alive female child with birth weight 3.5 Kg at 7:50 pm. A cross section of umbilical cord was examined. It revealed 2 umbilical arteries and single umbilical vein. Patient was discharged from hospital on 2nd April 2013 with a healthy baby.
3. Discussion
- The umbilical cord serves as an essential conduit for oxygen and nutrients between mother and foetus. The cord normally inserts near the centre of the placenta. Both foetal and placental cord insertions are generally well visualized by USG. The umbilical cord normally has two arteries and one vein. Occasionally, there is only one single umbilical artery (SUA) present in the umbilical cord.[5] Approximately this affects between 1 in 100 and 1 in 500 pregnancies, making it the most common umbilical abnormality.[5] It is more common in multiple births. Presence of an SUA is a risk factor for additional complications; however most fetuses with the condition will not experience other problems, either in utero or after birth. Prior to ultrasound technology, the only method for determining the presence of a SUA was at birth, following an examination of the placenta. However studies in past reflected on the variable predictive accuracy of USG Doppler in correctly identifying SUA as an entity. The sensitivity, specificity, positive and negative predictive value has been reported at 36%, 99%, 32% and 99% respectively in a previous study.[6] These results seem disappointing. This case report points to the same disappointment. What exactly leads to such a variation in the predictive accuracy of USG Doppler remains a question of debate. Further these variations should be examined across populations and in different settings. However one thing that this report does point to is the practice in a routine clinical setting where the time allocated to a routine anomaly scan is around15 minutes.
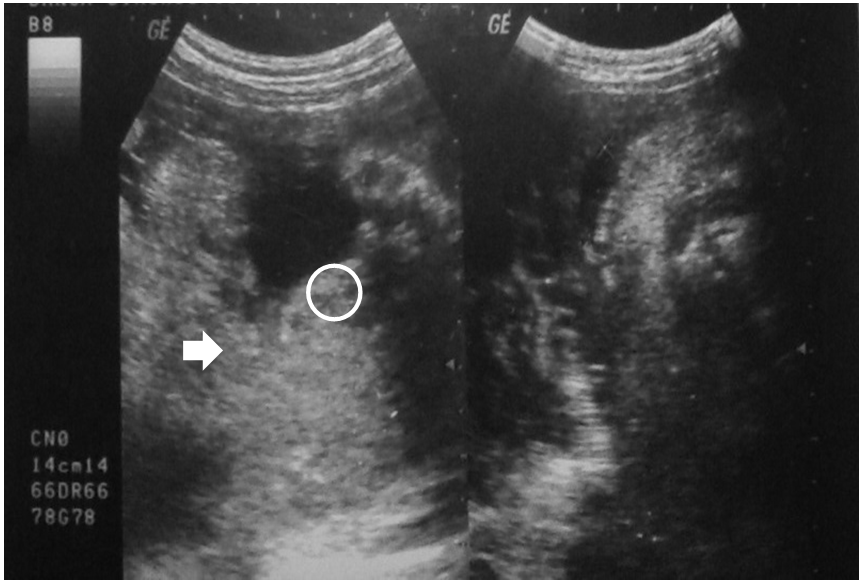 | Image 1. Gray scale image showing an amniotic fluid pocket (white arrow). Circle depicts the reported ‘single umbilical artery’ |