-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research In Cancer and Tumor
2013; 2(2): 27-30
doi:10.5923/j.rct.20130202.01
Smoking Behavior Patterns among Patients Being Managed for Malignancy in a Medical College in North-West India
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSunil Kumar Raina1, Vishav Chander1, Muninder Kumar Negi2, Ashok Bhardwaj1
1Department of Community Medicine, Dr. RP Government Medical College, Tana, Kangra (HP) India
2Department of Radiotherapy, Dr. RP Government Medical College, Tanda (HP), India
Correspondence to: Sunil Kumar Raina, Department of Community Medicine, Dr. RP Government Medical College, Tana, Kangra (HP) India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Introduction: Smoking has been known as a known risk factor for many types of cancer. Besides this, studies have shown that continued smoking during treatment for many types of cancer has several adverse effects on treatment, such as increasing the chances of a second malignancy. Material and Methods: The study was conducted among patients being managed in the department of radiotherapy. Participants were eligible if they had been receiving treatment for any type of cancer in the department of radiotherapy. Results: The mean age for patients was 57.24±16.62 and the mean age for both sexes was almost same (57.82±18.39 for males and 56.52±13.31for females). The most common malignancy among men was carcinoma of lung with 21/84 (25%) reporting with it while the most common malignancy among females was carcinoma of breast (30/69; 43%). The mean age at the start of smoking in case of carcinoma lung was 19±6.84 years. Discussion: It is to the benefit of cancer patients that a well-structured smoking cessation programs, either through individual counselling by health care providers or through lifestyle change group therapy is in place. But the key question remains as to what is impact and utility of these programmes among patients being managed for malignancy.
Keywords: Smoking, Behaviour, Pattern, Cancer, Radiotherapy
Cite this paper: Sunil Kumar Raina, Vishav Chander, Muninder Kumar Negi, Ashok Bhardwaj, Smoking Behavior Patterns among Patients Being Managed for Malignancy in a Medical College in North-West India, Research In Cancer and Tumor, Vol. 2 No. 2, 2013, pp. 27-30. doi: 10.5923/j.rct.20130202.01.
1. Introduction
- Smoking has been known as a known risk factor for many types of cancer, including cancers of the lung, bladder, oesophagus, stomach, kidney, cervix, pancreas, and head and neck.[1] Besides this, studies have shown that continued smoking during treatment for many types of cancer has several adverse effects on treatment, such as increasing the chances of a second malignancy[2-5]. It has also been suggested that smoking interferes with the three most common cancer treatments: surgery, chemotherapy, and radiation therapy.[6] In particular smoking is known to increase the risk for infection during surgery and slows wound healing afterward[7]; increases the risk of adverse effects from and decreases the response to radiation therapy [8,9]; and may decrease the effectiveness of chemotherapy drugs.[10] Studies have also shown that continuing with smoking after cancer diagnosis increases mortality rates. [8,11,12] Studies have also proposed that smoking cessation attempts begun immediately after cancer diagnosis may have a higher than normal success rate.[6,13]A number of studies in past have worked on the factors that influence smoking habits among cancer patients.[7-12] A few interventional studies have showed cessation rates of 22% to 59%,[6, 13, 14] But studies in this regard have mostly involved patients with head and neck and lung cancers. The purpose of this study was to examine the smoking habits among patients with various types of cancers as a preliminary step to creating a successful smoking cessation intervention. The department of radiotherapy in our institution became functional two years back. This study will go a long way in establishing basis for a smoking cessation programme.
2. Methods
- The study was conducted among patients being managed in the department of radiotherapy in a medical college in a rural area of north-west India. Participants were eligible if they had been receiving treatment for any type of cancer in the department of radiotherapy. All patients receiving treatment during the study period of one month were included in the study.The patients were interviewed using a pre-structured questionnaire to elicit information on patient’s history of disease. Fagerstrom Nicotine Tolerance Questionnaire (FNTQ) was used to elicit information on tobacco use and frequency.Data obtained from the questionnaire consisted ofsocio-demographic information, clinical and smoking history. Socio-demographic information collected included age, sex, income, occupation, highest level of education attained, and whether respondents were currently married or not.Clinical information included type of cancer and time since diagnosis. Smoking history parameters included current smoking status (whether participants were current, former, or never smokers); smoking frequency and timing.Data were analyzed using SPSS version 11.5 (SPSS Inc, Cary, North Carolina).
3. Results
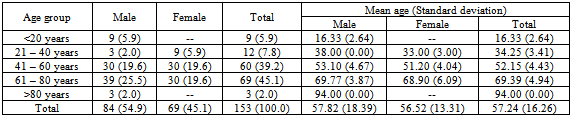
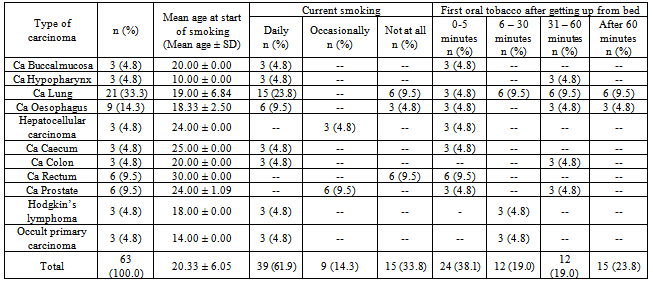
- A total of 153 patients undergoing treatment, were included in the study. 84/153 (54.9%) were male patients and 69/153 (45.1%) were female patients. (Table 1) The mean age for patients was 57.24±16.62 and the mean age for both sexes was almost same (57.82±18.39 for males and 56.52±13.31for females). Majority of females 66/69 (95.6%) were home makers while a substantial number (30/84 i.e., 35%) of males had retired from service. 12/84 (14%) males were unable to work because of malignancy. There was not much difference in the mean years of education for men and women (6.54 ± 5.27 for males and 5.35 ± 5.21for females). 12/84 (14%) of males were unmarried while 6/84 (7%) were widower while 9/69 (13%) females were widowed. The most common malignancy among men was carcinoma of lung with 21/84 (25%) reporting with it while the most common malignancy among females was carcinoma of breast (30/69; 43%). (Figure 1)This was followed by carcinoma rectum in males (12/84; 14%) and carcinoma stomach in females (15/69; 21.7%). (Figure 1) 63/84 (75%) of men had a history of previous or current smoking. Out of these 63 patients, 48 (76%) patients were current smokers. No female had a history of previous or current smoking. Interestingly no female among the patients studied was suffering from carcinoma of hypo pharynx, buccal mucosa, oesophagus or lung. The mean age at the start of smoking in case of carcinoma lung was 19±6.84 years. Patients with carcinoma of hypo pharynx started smoking at the earliest with mean age of starting smoking being 10 years.
|
|
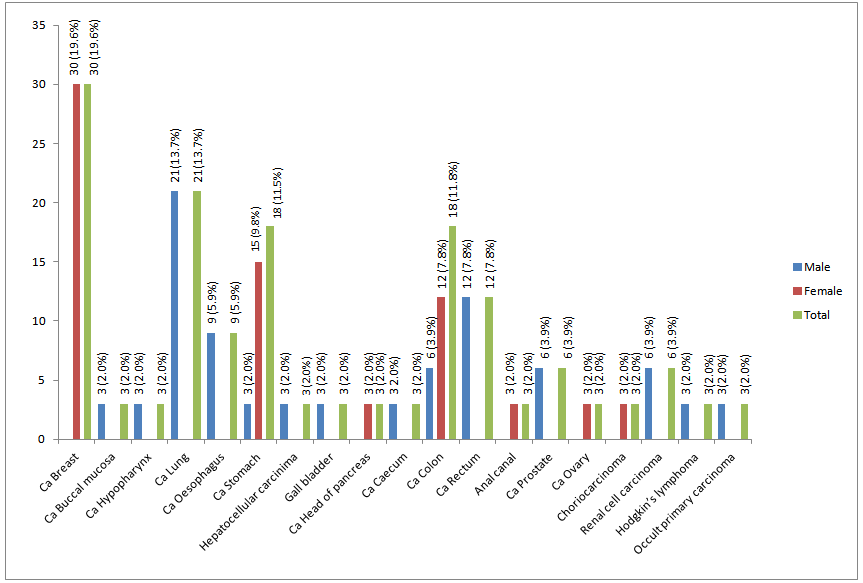 | Figure 1. Showing the type of malignancy present in the study population |
4. Discussion
- The study highlights the fact that smoking is associated with majority of the patients reporting in our study. Interestingly, abstinence from smoking among patients of malignancy is not a common practice. Even patients with malignancy of hypo pharynx, buccal mucosa, oesophagus or lung have not abstained from smoking. In an earlier study conducted at, only 44% of cancer patients who were smokers at diagnosis maintained abstinence after they were diagnosed with cancer.[15] Therefore the findings in our study are comparable to those reported in previous studies.[13-14, 16- 20] The fact that the dangers of smoking for cancer patients are not explained to them by a health care provider maybe a contributing factor. In an earlier study only 62% of patients who were smokers at diagnosis reported having been told to quit by their doctors.[15] Also the fact that these patients have a variable survival after diagnosis also impedes strict advice on smoking cessation. The good thing to observe in this study is the prevalence of smoking in females, which is nil. This is reflective of the trends in smoking among females across India.It is to the benefit of cancer patients that a well-structured smoking cessation programs, either through individual counselling by health care providers or through lifestyle change group therapy is in place. The programme needs to reflect global consideration but has to be rooted in local needs and resources. Budget allocation in this field is a cause for concern as also the unwillingness on part of stakeholders to get involved. Besides this the key question remains as to what is impact and utility of these programmes among patients being managed for malignancy.Limitations: The study per se does not reflect on the trends in malignancy in our setup as the sample used for the purpose of this study is based on convenience. As such a few types of malignancies may not be found in the study sample. Inspite of this and the small sample, the study does open up areas of research in tobacco use and malignancies.