-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research In Cancer and Tumor
2013; 2(1): 22-26
doi:10.5923/j.rct.20130201.03
Synchronous Adenocarcinoma of Caecum and Sigmoid Colon: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTakalkar Unmesh V.1, Asegaonkar Balaji N.1, Asegaonkar Shilpa B.2, Kodlikeri Pushpa1, D. N. Reddy3
1Kodlikeri memorial’s CIIGMA Hospital Jalna road Aurangabad, 431001, Maharashtra India
2Goverment Medical College Aurangabad Maharashtra India
3Asian Institute of Gastroenterology Hyderabad India
Correspondence to: Takalkar Unmesh V., Kodlikeri memorial’s CIIGMA Hospital Jalna road Aurangabad, 431001, Maharashtra India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Patients with carcinoma of the colon are known to have synchronous multiple malignant lesions with reported incidence 2.3-12.4%. We report a case of synchronous adenocarcinoma of caecum and sigmoid colon managed successfully at our center. 58 year old man underwent colonoscopy and growth observed in sigmoid colon. On explorative laparotomy synchronous coexisting, two tumors were detected in the caecum and sigmoid colon. Tumors were excised by right hemicolectomy and sigmoidectomy. Histopathologically both tumors were moderately differentiated adenocarcinoma with normal mucosa in between them without metastasis. In post operative phase, patient developed pneumonitis, diarrhea and Pancytopenia. These sequels were managed aggressively with mechanical respiratory support, blood transfusion and antibiotics. Then patient received adjuvant chemotherapy. Synchronous multiple primary malignancies are significant clinical entity from diagnostic and management point of view. Careful evaluation for detection of multiple tumors plays a crucial role for a better outcome of the disease.
Keywords: Synchronous Multiple Malignancy, Adenocarcinoma, Caecum, Sigmoid Colon
Cite this paper: Takalkar Unmesh V., Asegaonkar Balaji N., Asegaonkar Shilpa B., Kodlikeri Pushpa, D. N. Reddy, Synchronous Adenocarcinoma of Caecum and Sigmoid Colon: A Case Report, Research In Cancer and Tumor, Vol. 2 No. 1, 2013, pp. 22-26. doi: 10.5923/j.rct.20130201.03.
1. Introduction
- Worldwide, colorectal carcinoma represents 10-15% of all cancer and second leading cause of cancer related death. In India also, its prevalence is rising in proportion of male: female as 6.7:5.5 per 100000 populations.[1] In 2007 World Cancer Research Fund reported epidemic of colorectal cancer as a major public health problem due to adaptation of modern lifestyle. Changed dietary pattern, sedentary lifestyle, smoking, increased lifespan and genetic susceptibility are predisposing factors for development of colorectal cancer.[2] In context of location, 75% of carcinoma of colon occurs in the left colon, 22% in right and only 3% in the caecum.[3] Patients with carcinoma of the colon have chances of synchronous multiple malignant lesions with a reported incidence ranged between 2.3-12.4%.[4] Double malignancies of the gastrointestinal tract are very rare. In a review of more than 2000 patients, Minni et al. found the incidence of a second primary tumor in the gastrointestinal tract to be 4.3%. This association most often occurs in patients with familial cancer syndromes.[5] It is a significant clinical entity and if detected early results in a better outcome. Otherwise second malignant lesion with metachronous presentation poses significant problems in management. We report a case of synchronous adenocarcinoma of caecum and sigmoid colon managed successfully at our center.
2. Case Presentation
- A 58 year old man presented with complaints of pain in the abdomen and black colored stools over the last six months. Clinical examination revealed the existence of a palpable mass in right iliac fossa as well as in left iliac fossa. On acquisition of detailed history, personal and family history of malignancy of the gastrointestinal tract was not significant. Patient was pale with hemoglobin 7.2g/dL and all other biochemical and hematological parameters were within normal limit. Ultrasound sonography (Figure 1 and 2) and computed tomography revealed irregular circumferential thickening in caecum and sigmoid colon suggestive of malignancy without evidence of distant metastasis. On colonoscopy growth in the region of sigmoid colon was observed and biopsy was taken. (Figure 3) Further colon could not be visualized because of the presence of mass. Biopsy of colonic growth revealed presence of malignant cells suggestive of moderately differentiated adenocarcinoma.
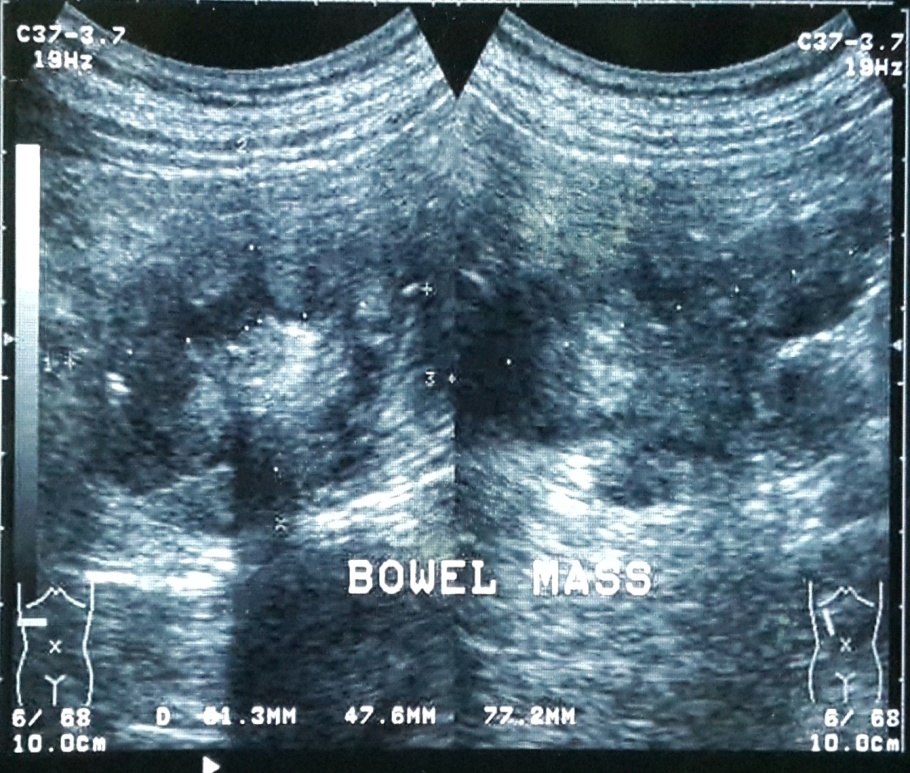 | Figure 1. Ultrasound examination showing mass in right iliac region |
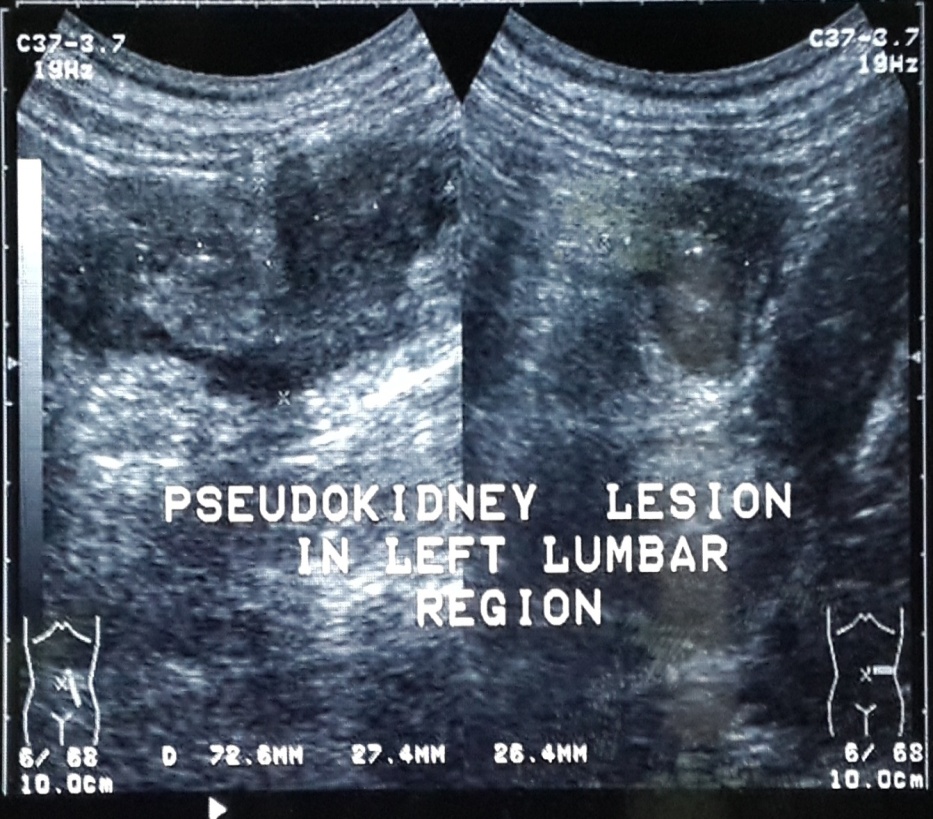 | Figure 2. Ultrasound examination showing mass in left iliac region |
 | Figure 3. Growth observed in the sigmoid colon during colonoscopy |
 | Figure 4. Specimen of resected growth with segments of the large bowel |
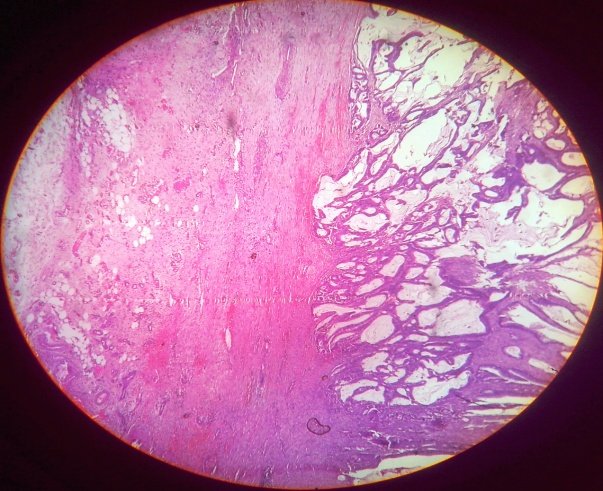 | Figure 5. Histological examination of moderately differentiated adenocarcinoma from caecum |
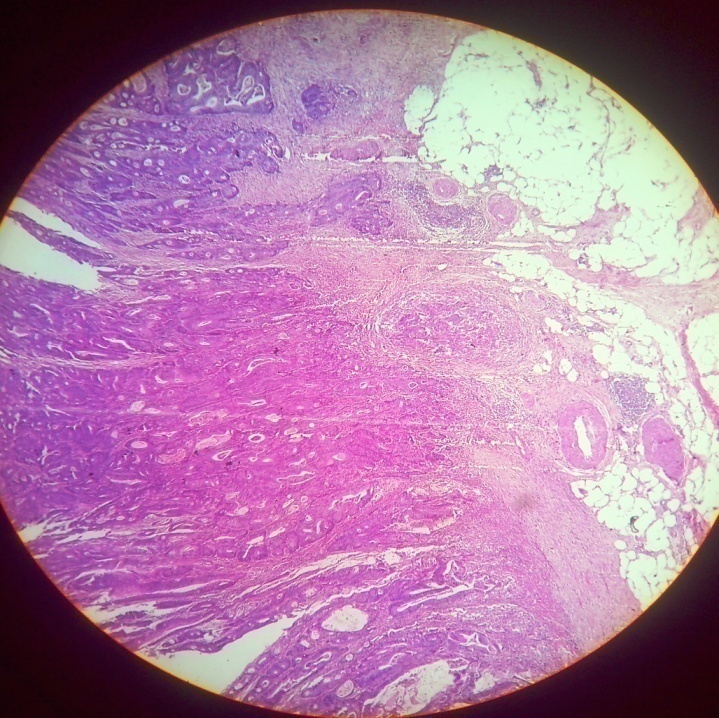 | Figure 6. Histological features of moderately differentiated adenocarcinoma from sigmoid colon |
3. Discussion
- Multiple primary cancer is defined as occurrence of two or more different primary malignancy in same or different organs synchronously or metachronously. Phenomenon of multiple primary tumors was first described by Billroth and further by Warren and Gates.[6] Colon is the most commonly affected organ by multiple tumors. 32% of cases of multiple tumors localize in the large intestine.[7] In our case risk factors recognized for carcinoma of colon were smoking, consumption of nonvegetarian food and Diabetes Mellitus. Personal and family history did not contribute any further information. Yuhara et al concluded in their meta-analysis Diabetes Mellitus as an independent risk factor for colorectal cancer.[8] Multiple primary colorectal cancers are predominantly observed in males. Common sites of multiple primary colorectal cancers are the sigmoid colon and rectum. The aetiopathology of coexisting multiple tumors remains unclear, but it has been hypothesized that they can arise from tissues with similar embryological origin when they get simultaneously exposed to carcinogens or hormones.[9] Our case fulfills the criterion reported by Cunliffe et al who described synchronous adenocarcinoma as two or more in number detected either pre or intraoperatively, or postoperatively within 6 month. They should be distinctly separated by at least 4 cm distance, and they should not consist of submucosal spread or a satellite lesion of each other.[10] In the present report 58 year old man with synchronous adenocarcinoma in the caecum and sigmoid colon with the existence of normal colonic mucosa between two neoplasms is desribed. On colonoscopy visualization of bowel beyond sigmoid colon was not possible due to the presence of tumor. During laparotomy coexistence of both tumors was observed and they were excised with two segment resection. Joo Won Yoon and colleagues identified 26 cases with multiple primary colorectal tumors among 1669 patients. Six of them with synchronous lesions were treated with two segment resection of colon as we managed our case.[11]Masatoshi Oya et al reported 4.8% cases of synchronous colorectal carcinoma predominantly in males associated with a short post operative survival compared to cases with single lesion.[4] Prognosis depends on deeper wall penetration, lymph node metastasis, distant metastasis and advanced pathological stage. Some studies reported lesions predominantly in the left colon in contrast to some studies with a predominance in the right colon.[12, 13] Preoperative careful evaluation for the presence of multiple malignant lesions can be achieved with the help of optical colonoscopy, intraoperative palpation and colonoscopy, barium enema and colonoscopy. Intraoperative thorough examination of total colon is a crucial step to avoid missing of coexisting tumors and subsequent operative procedures. Chen et al reported 66% cases of synchronous cancers were missed in preoperative examination.[12] Po-Li Tsai and associates reported significantly higher mortality in synchronous cases than single cancer.[14] Synchronous adenocarcinoma in the colon has been described only in one case report by Gruia et al. They observed flat type of adenocarcinoma in the caecum and mucinous adenocarcinoma in the sigmoid colon.[15] Various reports described coexisting multiple tumors in colorectal region with other organs. To our best knowledge ours is the second case report of synchronous adenocarcinoma of sigmoid colon and caecum. Thorough clinical and radiological evaluation is necessary in patients with colorectal cancer. If multiple lesions are missed, they present as early metachronous carcinoma in advanced stage. Present case report emphasizes the necessity of careful evaluation for detection of additional cancers.Conclusion: Complete perioperative evaluation of the colon is necessary to identify multiple malignant lesions. Surgeon should be alert and always be aware of possibility of multiple tumors in the colon to avoitd he second surgery for missed lesion to secure best prognosis.
ACKNOWLEDGMENTS
- The author reports no conflicts of interest in this work.