-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2026; 16(1): 10-13
doi:10.5923/j.phr.20261601.02
Received: Apr. 5, 2026; Accepted: May 2, 2026; Published: May 29, 2026

Resource Provision and Logistics of Medical Care During an Epidemiological Crisis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhusanov Anvar Mirzakbarovich, Alimova Hilola Pulatovna
“Republican Specialized Hospital Zangiota No. 1”, Tashkent, Uzbekistan
Correspondence to: Khusanov Anvar Mirzakbarovich, “Republican Specialized Hospital Zangiota No. 1”, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

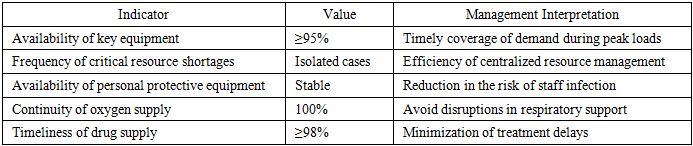
Objective. To evaluate the effectiveness of an adaptive resource supply and logistics model in a specialized hospital during an epidemiological crisis. Materials and Methods. A retrospective-prospective organizational and managerial study of the activities of the Republican Specialized Hospital “Zangiota No. 1” was conducted for the period 2020–2025. Data on bed capacity, equipment availability, oxygen infrastructure, pharmaceutical stock levels, personal protective equipment (PPE), and internal logistics flows were analyzed. Results. During the COVID-19 pandemic, resource management was transformed into a centralized and controlled process, including real-time monitoring, forecasting, and redistribution of material and technical resources. A prioritization system for critically important components—bed capacity, respiratory support equipment, pharmaceuticals, and PPE - was implemented. The introduction of daily consumption monitoring and safety stock formation ensured ≥98% timeliness of pharmaceutical supply and stable PPE availability. The availability of key equipment reached ≥95%, oxygen supply continuity was maintained at 100%, and cases of critical shortages were isolated. Optimization of internal logistics flows reduced delivery time and decreased the workload on medical staff. Collectively, these measures ensured the hospital’s operational resilience during peak epidemiological periods. Conclusion. The adaptive logistics model enhanced resilience, manageability, and resource efficiency of the specialized hospital, confirming the importance of centralized management and predictive planning during epidemiological crises.
Keywords: Resource supply, Logistics, COVID-19, Resource management, Hospital
Cite this paper: Khusanov Anvar Mirzakbarovich, Alimova Hilola Pulatovna, Resource Provision and Logistics of Medical Care During an Epidemiological Crisis, Public Health Research, Vol. 16 No. 1, 2026, pp. 10-13. doi: 10.5923/j.phr.20261601.02.
1. Introduction
- Epidemiological crises, such as the COVID-19 pandemic, have demonstrated the critical importance of effective resource and logistics management in healthcare delivery. The sharp increase in patient numbers, shortages of equipment and medications, and disruptions in global supply chains necessitated a transition from traditional supply models to strategically oriented, adaptive resource management systems. Healthcare logistics is understood as the integrated management of material and information flows aimed at the timely and efficient meeting of patient needs, particularly under crisis conditions [1]. The implementation of lean healthcare principles within logistical processes enables the optimization of operational procedures, reduction of losses, and improvement of care delivery efficiency [1].Modern dynamic resource allocation models are based on epidemiological forecasting and allow for the advance estimation of needs in hospital beds, equipment, and personnel [2,3]. The application of mixed-integer programming methods facilitates cost minimization while ensuring adequate coverage of the growing demand for healthcare services [4]. The reorganization of healthcare networks, including bed capacity management and workforce redistribution, is also of critical importance, as it helps prevent hospital overload and improves the quality of patient care [5]. The use of fuzzy forecasting models under conditions of uncertainty further enhances the adaptability of healthcare systems [5]. At the same time, challenges remain related to the need for rapid data acquisition and the high rate of change in the epidemiological situation, underscoring the importance of further improving logistical and resource management strategies in healthcare.
2. Materials and Methods
- This study was conducted as a retrospective–prospective organizational and managerial analysis of resource provision and healthcare logistics under conditions of an epidemiological crisis. The observation period covered 2020–2025 and included the active phase of the COVID-19 pandemic, peak workload periods, and the post-COVID transformation of the hospital. The study was based at the Republican Specialized Hospital “Zangiota No. 1” (Tashkent, Uzbekistan), which functioned as a tertiary infectious disease referral center during the pandemic.The object of the study was the hospital’s material and technical resource management system, including bed capacity, medical equipment and oxygen infrastructure, pharmaceuticals, personal protective equipment (PPE), consumables, and internal logistical processes. The analysis incorporated data from organizational and statistical reports, internal hospital registries, information on bed capacity dynamics, equipment availability, the structure of safety stock for pharmaceuticals, centralized distribution of PPE, and indicators of continuity of oxygen supply.The effectiveness of the logistics model was assessed using the following indicators: availability of key equipment (%), frequency of critical resource shortages, stability of PPE supply, timeliness of pharmaceutical provision (%), continuity of oxygen support (%), and the hospital’s operational resilience during peak workload periods. Organizational-analytical, comparative, and systems-based research methods were applied.
3. Results
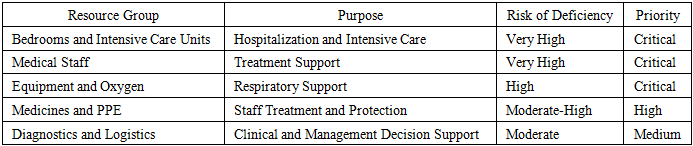
- The COVID-19 pandemic demonstrated that the resilience of a specialized infectious disease hospital is determined not only by workforce capacity and patient flow organization, but also by the effectiveness of resource management systems. Under conditions of a sharp increase in demand for medical services, disruptions in global supply chains, and high levels of uncertainty, traditional approaches to resource planning proved insufficient, necessitating the implementation of adaptive logistics models.At the Republican Specialized Hospital “Zangiota No. 1,” resource provision was considered an integrated managerial process, encompassing planning, allocation, monitoring, and real-time adjustment of material and technical resource utilization.During the pandemic, the resource base of “Zangiota No. 1” included several key components: bed capacity and infrastructure, medical equipment, pharmaceuticals, personal protective equipment (PPE), and consumables (Table 1). Each of these components exhibited varying levels of vulnerability to shortages and required differentiated management strategies.
|
|
|
4. Discussion
- The results of the study confirm that under conditions of an epidemiological crisis, the resilience of a specialized hospital is determined not only by the volume of resources, but primarily by the quality of their allocation and the level of logistical manageability. International evidence indicates that dynamic resource allocation systems, incorporating regional demand, epidemiological forecasts, and disease structure, enable the rapid adjustment of supply volumes and redistribution of capacities across institutions [6]. This approach is particularly important during exponential growth in patient numbers, when static supply models become ineffective. Resource allocation should therefore be based on evidence and analytical tools that minimize the vulnerabilities of traditional planning methods [7].The integration of personnel, equipment, and material resources within hierarchical emergency healthcare delivery systems (EHDTS) is also of critical importance, as it ensures coordinated action and rational utilization of ambulance and hospital resources [8]. The establishment of centralized stockpiles of essential medical supplies increases availability and reduces the risk of local shortages during peak demand periods [8]. Similar principles underpin models of collaborative drug supply rebalancing aimed at equitable distribution and minimization of total losses under conditions of limited supply [6,9]. The application of linear and mixed-integer optimization methods enables evidence-based decisions on the redistribution of resources across regions and institutions [10].An important direction is the development of internal and external dispatching systems integrating local and interregional supply chains, which reduces logistical delays and improves the level of demand satisfaction in affected areas [11,12]. Integrated healthcare resource allocation models, involving coordination between institutions at different levels, contribute to more equitable access to care and help prevent overloading of individual hospitals [13].However, despite the effectiveness of optimization models, the pandemic has revealed persistent systemic vulnerabilities, including disruptions in global supply chains, shortages of personal protective equipment, and workforce limitations, particularly in resource-constrained regions [14]. The rapid evolution of crisis situations often outpaces existing management mechanisms, necessitating the implementation of real-time systems and digital tools for monitoring and forecasting. Thus, effective resource provision in epidemic conditions requires not only the use of mathematical models, but also continuous adaptation, interdisciplinary collaboration, and strategic planning aimed at enhancing healthcare system resilience.
5. Conclusions
- The implementation of an adaptive model of resource provision and logistics at the Republican Specialized Hospital “Zangiota No. 1” enabled the transformation of material and technical resource management into a centralized, analytically driven process oriented toward rapid response under conditions of epidemiological instability. The centralization of equipment and PPE distribution, daily monitoring of pharmaceutical inventories, establishment of safety stock reserves, and optimization of internal logistical flows ensured a high level of availability of key resources (≥95%), uninterrupted oxygen supply (100%), and minimization of critical shortages.