-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2026; 16(1): 1-9
doi:10.5923/j.phr.20261601.01
Received: Feb. 10, 2026; Accepted: Mar. 6, 2026; Published: May 29, 2026

Evaluation of C-reactive Protein-Related to Oxidative Stress in Patients Suffering from Hyperthyroidism Babylon, Iraq (2024)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMitra Noori1, Hanadi T. Muslem2, 3
1Department of Biology, Faculty of Science, Arak University, Arak-Iran
2MSc Student of Biochemistry, Department of Biology, Faculty of Science, Arak University, Arak-Iran
3Department of Biochemistry, College of Sciences, Al-Mustaqbal University, Babylon, Iraq
Correspondence to: Mitra Noori, Department of Biology, Faculty of Science, Arak University, Arak-Iran.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The thyroid gland is considered one of the most important endocrine glands, due to its great role and impact on the body and its multiple functions. This study highlights the role of CRP in patients with hyperthyroidism. The production of C-reactive protein is part of the non-specific acute phase response to most forms of inflammation, infection, and tissue damage, so the study aimed to determine whether there is an effect of C-reactive protein on hyperthyroidism. This study was designed to evaluate the acute phase of hyperthyroidism and its association with oxidative stress markers and CRP levels in Babylon. The study was performed in 2024. 120 subjects were enrolled in this study, 60 controls 27 males, and 33 females, and 60 patients with hyperthyroid 31 males, and 29 females in our study, the mean age of the population ranged from (25-75) years. Completion of consent and question forms were done by the control and patient groups. Blood samples were collected from both control and patient groups. All laboratory test analysis were performed in Iraq at Murjan Teaching Hospital, Alpha Lab/ Babylon, and the Clinical Biochemistry laboratory in the College of Science (University of Al-Mustaqbal). 16 quantitative and qualitative parameters were studied in them. All data were analyzed using SPSS ver. 28, T-Test &Mann-Whitney U test (P≤ 0.05). Results showed decreasing TSH and increasing T4 and T3 in the hyperthyroidism group. TC, TG, LDL and HDL serum had a significant decrease in hyperthyroidism in comparison with the healthy group, while increasing CRP was observed in hyperthyroidism people. Results clearly showed increasing MDA in patient group compared to the control. AOPP level was significantly higher in the patient comparing to control group. CAT activities increased in the patient group compared to the control (𝑃≤ 0.05). These results may go some way toward explaining that diseases result from thyroid disorders such as hyperthyroidism, which in turn play an important role in the induction of oxidative stress-mediated inflammation. The comparison with hypothyroidism cases or post-treatment effects is an important suggestion. Therefore, regarding this point is needed in future work.
Keywords: Hyperthyroidism, C-reactive protein, Oxidative stress, Antioxidant, Inflammation, Iraq
Cite this paper: Mitra Noori, Hanadi T. Muslem, Evaluation of C-reactive Protein-Related to Oxidative Stress in Patients Suffering from Hyperthyroidism Babylon, Iraq (2024), Public Health Research, Vol. 16 No. 1, 2026, pp. 1-9. doi: 10.5923/j.phr.20261601.01.
Article Outline
1. Introduction
- Hyperthyroidism is a endocrine disease in which the thyroid gland produces excessive amounts of thyroid hormones. Thyrotoxicosis is a condition that occurs due to elevated levels of thyroid hormones of any cause and therefore includes hyperthyroidism [1]. There are several causes of hyperthyroidism. Most often, the entire gland is overproducing thyroid hormone. Less commonly, a single nodule is responsible for the excess hormone secretion, called a "hot" nodule. Thyroiditis (inflammation of the thyroid) can also cause hyperthyroidism. Functional thyroid tissue producing an excess of thyroid hormone occurs in a number of clinical conditions. The major causes in humans are: graves' disease, toxic thyroid adenoma, toxic multinodular goiter, inflammation, Hashimoto, sthyroditis, amiodarone, postpartum thyroiditis, struma ovarii, excess iodine consumption (kelps), exogenous thyrotoxicosis, TSH hypersecretion and etc. [2-5]. Signs and symptoms vary between people and may include irritability, muscle weakness, sleeping problems, a fast heartbeat, heat intolerance, diarrhea, enlargement of the thyroid, hand tremor, and weight loss. Symptoms are typically less severe in the elderly and during pregnancy. An uncommon but life-threatening complication is thyroid storm in which an event such as an infection results in worsening symptoms such as confusion and a high temperature; this often results in death [6].Hyperthyroidism due to certain types of thyroiditis can eventually lead to hypothyroidism (a lack of thyroid hormone), as the thyroid gland is damaged. Also, radioiodine treatment of Graves' disease often eventually leads to hypothyroidism. Such hypothyroidism may be diagnosed with thyroid hormone testing and treated by oral thyroid hormone supplementation [7].Measuring the level of thyroid-stimulating hormone (TSH), produced by the pituitary gland (which in turn is also regulated by the hypothalamus's TSH-Releasing Hormone) in the blood, is typically the initial test for suspected hyperthyroidism. A low TSH level typically indicates that the pituitary gland is being inhibited or "instructed" by the brain to cut back on stimulating the thyroid gland, having sensed increased levels of T4 and/or T3 in the blood. In rare circumstances, a low TSH indicates primary failure of the pituitary, or temporary inhibition of the pituitary due to another illness (euthyroid sick syndrome) and so checking the T4 and T3 is still clinically useful [8].In hyperthyroidism, C-reactive protein (CRP) levels can be elevated, and this is linked to increased oxidative stress. Oxidative stress, caused by an imbalance between reactive oxygen species (ROS) production and the body's antioxidant defenses, damages cellular components and is a key factor in the pathogenesis of hyperthyroidism. Czarnywojtek et al. studies showed rapid metabolic activity brought on by hyperthyroidism can stimulate the immune system, cause the adrenergic nerve system to become hyperactive, and cause a significant increase in peripheral blood flow. All of these effects can raise the levels of CRP [9]. It has also been suggested that the level of CRP may be used as a measure of arterial hardening and as an indicator to gauge its amelioration in hypothyroid patients [10].Some studies showed associations between lipids metabolism and thyroid diseases. Thyroid hormones play a crucial role in regulating lipid metabolism. Both hypothyroidism and hyperthyroidism can lead to significant alterations in lipid profiles, increasing the risk of cardiovascular disease and other metabolic complications. Al-Odat et al (2024) studies showed the prevalence of thyroid dysfunction is high among Jordanians. It also demonstrated that the lipid profile is abnormal in thyroid dysfunction conditions. Dyslipidemia is a major risk factor for cardiovascular disease. Their results recommended screening high-risk groups for thyroids dysfunction, such as females. Furthermore, educating the public about thyroid dysfunction can help detect thyroid conditions at an early stage for proper intervention. Also they emphasized the importance of monitoring lipid levels in patients with thyroid dysfunction to prevent or, at the very least, minimize cardiovascular diseases [11].This study was conducted to evaluate the level of the human antioxidant system by measuring some antioxidant enzymes such as catalase (CAT), to evaluate the effect of oxidative stress by measuring some oxidative markers such as MDA and AOPP, evaluation of inflammation by measuring some inflammatory markers such as CRP, evaluating the effect of thyroid hormones on lipid levels (TG, TC, HDL and LDL), and also examining the correlation between thyroid parameters (T3, T4 and TSH) with lipid parameters (TG, TC, HDL and LDL) and other studied parameters in hyperthyroidism and the control groups.
2. Materials and Methods
2.1. Study Design & Completion of Consent Forms and Questionnaires by the Control and Patient Groups
- This study is conducted at Murjan Teaching Hospital, Alpha Lab/ Babylon, and Clinical Biochemistry laboratoryin the College of Science (University of Al-Mustaqbal) during the period between (March 2024) to (May 2024). The study included 120 subjects, 60 controls (27 males & 33 females), and 60 Patients (31 males & 29 females) with hyperthyroidism, the mean age of the population ranged from (25-75) years. This research consisted of patients at the time of diagnosis and clinical presentation of hyperthyroidism to obtain accurate biochemical measurements of the inflammatory response and to minimize variability related to disease progression. All patients were diagnosed by specialized doctors, and the diagnosis was verified by clinical features and biochemical investigations. The diagnosis of hyperthyroidism in this study was confirmed based on clinical manifestations and thyroid function tests including T3, T4, and TSH levels. The prepared consent forms and questionnaires were delivered to the people of both patient and control groups who referred to Murjan Teaching Hospital in Iraq. Blood samples were collected from both control and patient groups.
2.2. Collection of Blood Samples & Biochemical Analysis
- All laboratory test analysis were performed in Iraq at Murjan Teaching Hospital, Alpha Lab/ Babylon, and the Clinical Biochemistry laboratory in the College of Science (University of Al-Mustaqbal). The studied blood biochemical factors, including TSH, T3, T4, AOPP, MDA, CAT, CRP, TG, TC, HDL and LDL, were calculated and recorded using standard and up-to-date measurement methods. Sixteen quantitative and qualitative parameters were studied (Table 1) and also studied factors reference range has been shown in Table 2. The statistical analysis was done using SPSS Ver. 28. The results were expressed as mean ± standard deviation (mean ± SD). Group statistics (T-Test) of two healthy and patient for studied factors was done. All of studied factors in both healthy and patients peoples compared with reference range (Table 2). Group statistics (T-Test) of two healthy and patient for studied factors (P≤0.05) were utilized (Table 3). Then correlations of studied parameters in patients obtained (Pearson-2-tailed method) (Table 4). The significant relationship between studied factors (TSH, T3, T4, AOPP, MDA, CAT, CRP, TG, TC and weight) obtained (Figures 1 a-l).
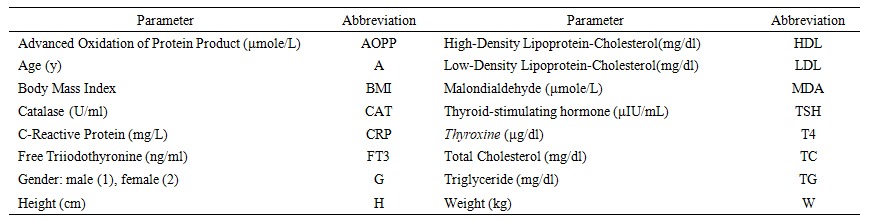 | Table 1. Studied quantitative and qualitative parameters in control and patient people |
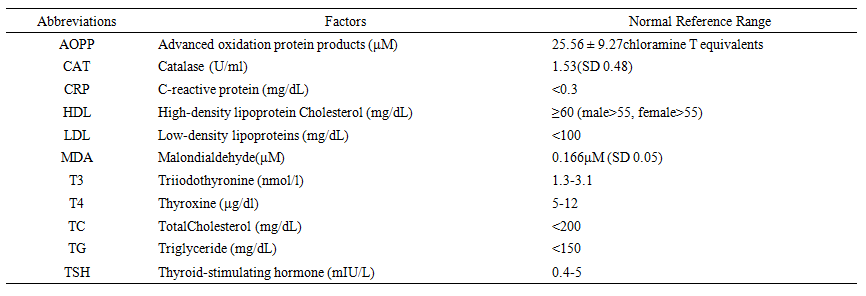 | Table 2. Studied factors reference range |
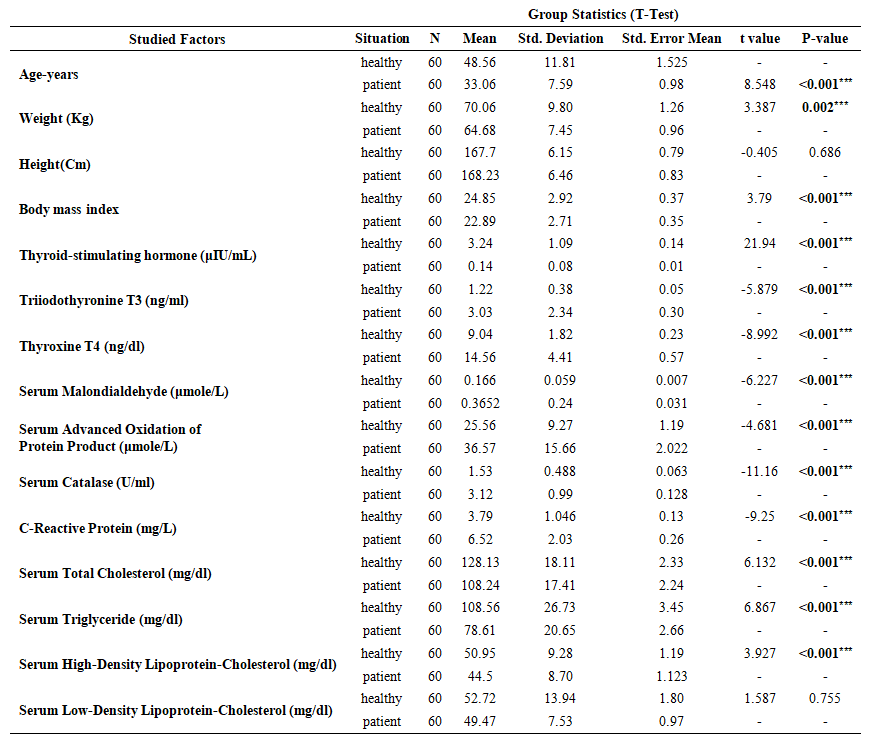 | Table 3. Group statistics (T-Test) of both healthy and patient for studied factors (P≤0.05) |
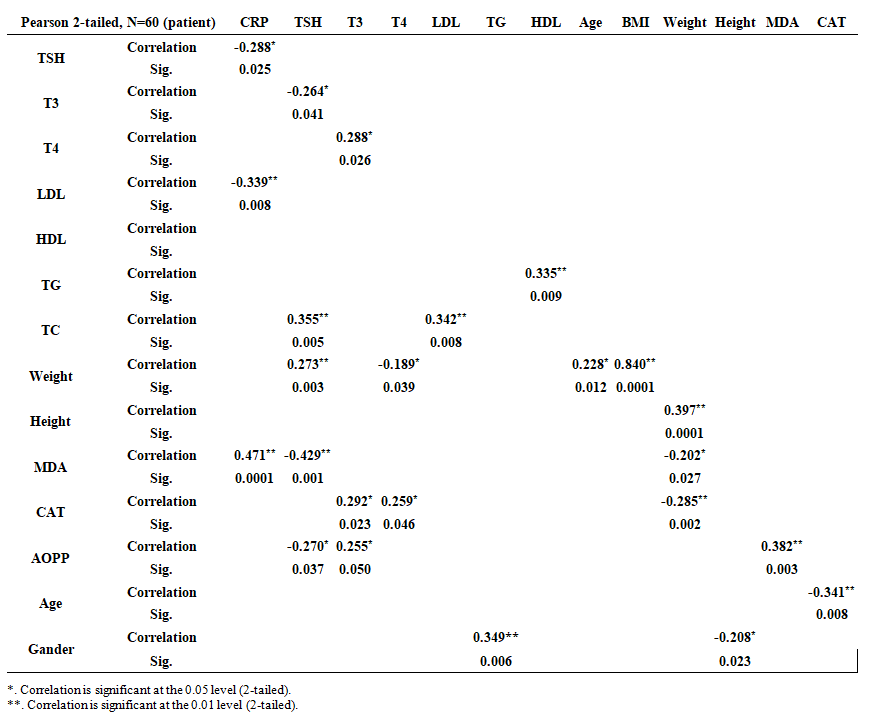 | Table 4. Correlations of studied parameters in 60 patients (Pearson -2-tailed method) |
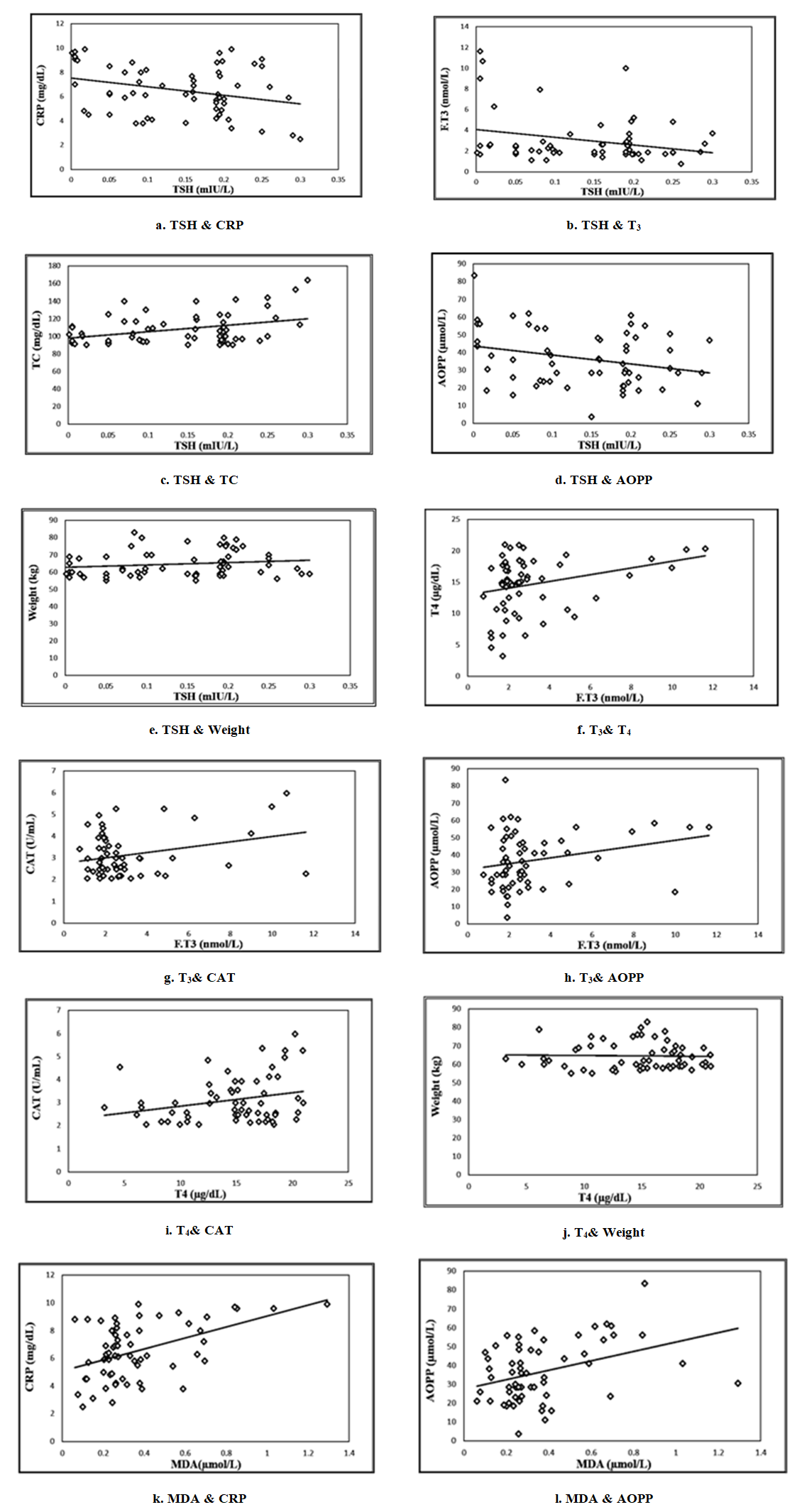 | Figure 1. (a-l). The significant relationship between studied factors (TSH, T3, T4, AOPP, MDA, CAT, CRP, TG, TC and weight) |
3. Results
- In this study 120 individuals, 60 of them were patients with Hyperthyroid 31 (51.66%) males, and 29 (48.33 %) females, and 60 healthy individuals: 27 (45 %) males, and 33 (55%) females. The age group of 25to 35 years had the most patients 39 (65%), whereas the age group of 36 to 45 years had the fewest patients 21(35%). The highest proportion of patients, 48 (80%), belonged to the normal weight group, while the lowest, 1 (1.66%), belonged to the obese group. Body mass index (BMI) as another biomarker for hyperthyroid is divided into three categories: normal weight (18.50–24 kg/m2), overweight (25–30 kg/m2), and obesity (>30 kg/m2). All of recorded data results of studied qualitative and qualitative factors in referral people to Murjan Teaching Hospital, Iraq between March 2024 to May 2024 were analyzed. Table 3 shows Group statistics (T-Test) of both healthy and patient for studied factors. Correlations of studied parameters in 60 patients (Pearson -2-tailed method) have been showed in Table 4 (P≤0.05). Figure 1: a-l showed the significant relationship between studied factors (TSH, T3, T4, AOPP, MDA, CAT, CRP, TG, TC and weight) in this research.
4. Discussion and Conclusions
- This study, which was conducted on 120 people, including 60 healthy individuals and 60 patients with hyperthyroidism, both men and women aged 25 to 65, showed that the percentage of men participating in this study was 48.33% and women were 51.66%. The higher incidence of hyperthyroidism in women than in men could be due to their increased sensitivity to hormonal changes. In this study, 18.33% of patients were overweight and 1.66% of obese patients had a BMI above 30. Weight changes can indicate abnormal thyroid function. Unexpected weight loss can be a sign of overproduction of thyroid hormones (hyperthyroidism). The present study showed a significant decrease in hyperthyroidism compared to the healthy group in mean serum TC, TG and LDL-C. The mean HDL-C level showed a significant decrease in hyperthyroidism compared to the control group (Table 3). Thyroid disorders are known to be factors affecting lipid metabolism. Serum cholesterol levels are generally inversely related to thyroid activity [12]. Studies show that in hyperthyroid patients, TG, TC, and LDL-C levels are reduced compared to euthyroid and hypothyroid individuals [13]. LDL oxidation is influenced by thyroxine levels, and increased thyroid hormone levels can affect HDL-C metabolism by stimulating the activity of cholesterol ester transferase, which converts cholesterol esters and TG in HDL-C to VLDL-C in a reversible manner [14]. This result is consistent with other studies, such as those conducted by [15].Table 3 shows elevated T3 and T4 levels and decreased TSH levels. Hyperthyroidism (overactive thyroid) occurs when thyroid gland produces too much of the hormone thyroxine. Hyperthyroidism can speed up the body’s metabolism, causing unwanted weight loss and a fast or irregular heartbeat [16]. Thyroid disease is more common than heart disease or diabetes. Hormones produced by the thyroid gland maintain the muscles, heart, brain, and other organs of the body. Improper functioning of the thyroid gland leads to hyperthyroidism (overactive thyroid), which produces too much T4. This can occur for a variety of reasons, including Graves' disease, hyperactive thyroid nodules, and thyroiditis. This type of hyperthyroidism occurs when one or more thyroid adenomas produce too much T4. Thyroid dysfunction is nonspecific and often variable. Therefore, the diagnosis of thyroid dysfunction is primarily based on biochemical abnormalities. The pituitary hormone thyrotropin (TSH) has a complex inverse relationship with the thyroid hormones thyroxine (T4) and triiodothyronine (T3) [17]. In this study we focused on diagnosis of hyperthyroidism based on clinical manifestations and thyroid function tests including T3, T4, and TSH levels. But we know studying thyroid-specific autoantibodies would provide deeper insight into the disease mechanism, and this will be considered in our future research work.Epidemiological studies conducted in areas with long-term iodine deficiency have shown that iodine deficiency increases the frequency of thyroid nodularity, thyroid autonomy, and ultimately hyperthyroidism in the elderly [18]. Malondialdehyde is a highly reactive organic chemical that occurs naturally as an enol. It is a marker of oxidative stress and is produced when polyunsaturated fatty acids are broken down by reactive oxygen species. MDA is a highly stable, low molecular weight end product of membrane lipid peroxidation that is produced along with other byproducts and is the most commonly used biomarker as an indication of lipid peroxidation [19]. The results of this study showed that malondialdehyde (MDA) levels were increased in patients with hyperthyroidism compared to controls. Under normal circumstances, epithelial cells of the thyroid have a moderate production of reactive oxygen species (ROS) that are physiologically required for the formation of thyroid hormones. These are not necessarily toxic because they are continuously detoxicized by the synthesis of the hormone or the endogenous antioxidant system [20,21]. It is deduced that oxidative stress occurs when reactive free radicals cause oxidative damage to the macromolecular structures of the cell. The thyroid gland plays an important role in producing general oxidative stress in conditions of the disease [22]. Thyroid hormones play a role in regulating the status of basic metabolism and in oxidative metabolism. These hormones can lead to high changes in the number and activity of mitochondrial respiratory chain compounds, which may result in increased production of reactive oxygen species (ROS). Thyroid hormones are associated with the oxidant and antioxidant status of the human organism [23]. The findings obtained from in vitro and in vivo studies show that thyroid hormones have a strong impact on oxidative stress. Untreated hyperthyroidism is associated with an increase in parameters of oxidative stress in serum/plasma compared with euthyroid subjects including lipid peroxides, hydrogen peroxide, and MDA [24]. The finding of elevated lipid peroxidation is consistent with Erem, Suleyman et al. (2015) [25]. AOPP is recognized as a new marker of oxidant-mediated protein damage, the severity of oxidative stress, and inflammation, and is produced during oxidative stress by ROS and chlorinated oxidants, such as hypochlorous acid and chloramines, which are formed by myeloperoxidase in activated neutrophils [26]. They are described as dityrosine-containing cross-linked protein products that may be used to determine the degree of oxidative protein modification [27]. The results of this study show increased levels of AOPP in patients with Hyperthyroidism compared to control. An elevated metabolic status in hyperthyroidism, accompanied by oxygen consumption, leads to increased construction of ROS [28]. It can oxidize diverse cellular constituents comprising DNA, lipids, and proteins, resulting in changes in tissue functions. Increased protein oxidation has been proved in diverse tissues in experimental hyperthyroidism. An increase in protein oxidation indicator was demonstrated in the plasma of hyperthyroid patients [29]. The results are consistent with Khinteel Jabbar et al (2022). The results of this study show increased levels of CAT in patients with Hyperthyroidism compared to control. The increase of some antioxidant enzyme activities such as CAT, which are the main antioxidants in the body may be indicative of the failure of compensating the induced oxidative stress. These enzymes may scavenge excess. O-2 and H2O2, and peroxides ROOH produced by free radicals. For example, SOD catalyzes the conversion of superoxide anion radical to H2O2. The resulting hydrogen peroxide in turn is decomposed by the enzymes GPx and CAT. Our findings showed an increased activity of CAT in patients with hyperthyroid which is a reflex mechanism against increased oxidative stress induced by hyperthyroidism, the results agree with [30]. CRP is composed of 187 amino acids and is an acute phase protein synthesized by the stimulation of leukocyte endogenous mediator [31]. Researchers have recently focused on the role of inflammatory reactions as a pathogenetic mechanism for atherosclerosis. Some studies have reported that CRP is increased in patients with atherosclerosis and this is related to prognosis. Furthermore, CRP is related to the development of cardiovascular disease and is an important factor for prognosis along with fibrinogen [32]. Anderson et al (1998) reported that the level of serum CRP is increased by more than two-fold in patients with coronary artery disease [33]. Despite the fact, no clear mechanism has been established in relationship between CRP and atherosclerosis [34]. CRP is an important risk factor for atherosclerosis and coronary artery disease [35]. Pasceri et al. (2000) proposed that CRP directly stimulates the inflammatory reaction of arteriosclerosis by inducing the expression of adhesion molecule in vascular endothelial cells and further hypothesized that CRP could be a treatment target for arteriosclerosis [36]. Hyperthyroidism causes rapid metabolic activity, which may result in adrenergic nervous system hyperactivity, immune system stimulation, and significantly increased peripheral blood flow. Thus conditions might result in an increase in CRP concentration [9].According to Table 4, CRP has a positive significant correlation with T3, T4, MDA, CAT, and AOPP, while a negative significant correlation with Age, BMI, TSH, TC, and TG. TSH has a positive significant link with Age, weight, BMI, HDL, TC, and TG, while a negative significant correlation with T3, T4, MDA, CAT, and AOPP. Serum T3 has a positive significant correlation with T4, MDA, CAT, and AOPP, while a negative significant correlation with Age, BMI, TC, and TG. Serum T4 has a positive significant correlation with CAT, and AOPP, while a negative significant correlation with Age, BMI, Weight, TC, and TG. Serum LDL has a positive significant correlation with TG, while a negative significant correlation with AOPP. Serum HDL has a negative significant correlation with MDA, CAT, and AOPP. Serum TC has a positive significant correlation with TG, and Age, while a negative significant correlation with CAT, and AOPP. Serum TG has a positive significant correlation with Age, while a negative significant correlation with MDA, CAT, and AOPP. Agehas a positive significant correlation with BMI, and Weight, while a negative significant correlation with MDA, CAT, and AOPP. BMI has a positive significant correlation with Weight, and Gander, while a negative significant correlation with CAT. Height has a negative significant correlation with Gander. Weight has a positive significant correlation with Height, while a negative significant correlation with MDA and CAT. Serum MDA has a positive significant correlation with CAT. Serum CAT has a positive significant correlation with AOPP.
4.1. Conclusions
- The results demonstrated a clear association between hyperthyroidism and elevated oxidative stress and inflammatory markers, that hyperthyroidism can lead to inflammation through high levels of C-reactive protein. Also it found a positive relationship between malondialdehyde and C-reactive protein. These changes indicate the metabolic and oxidative impact of thyroid hormones. Monitoring these biomarkers in hyperthyroid patients is essential. Future research is recommended to explore additional biochemical and immunological variables related to hyperthyroidism such as the therapeutic role of antioxidants.
ACKNOWLEDGEMENTS
- The authors would like to thank of Dr. Sabreen Farhan Jawad in Iraq. Thanks to all the laboratory staff of Murjan Teaching Hospital, Alpha Lab/ Babylon, and Clinical Biochemistry Laboratoryin the College of Science (University of Al-Mustaqbal) which for their cooperation and assistance, and I thank all patients for their cooperation and patience.