-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2023; 13(1): 32-37
doi:10.5923/j.phr.20231301.03
Received: May 11, 2023; Accepted: May 26, 2023; Published: Jun. 12, 2023

Review of the National AIDS and Sexually Transmitted Infections Case-Based Surveillance System for Viral Suppression among HIV Positive Women of Reproductive Age, Western Kenya, 2021
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSarafina S. Sikwata1, 2, Maurice Owiny1, Fredrick Odhiambo1, Jonah Onentiah2, Violet Oramisi2, Rose Wafula2, Maryan Daud1, Esau Langat1, Dickens Onyango3, A. Abade1
1Field Epidemiology and Laboratory Training Program, Kenya (FELTP)
2National AIDS & STI Control Program, Kenya (NASCOP)
3Ministry of Health, County Government of Kisumu, Kenya
Correspondence to: Sarafina S. Sikwata, Field Epidemiology and Laboratory Training Program, Kenya (FELTP).
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

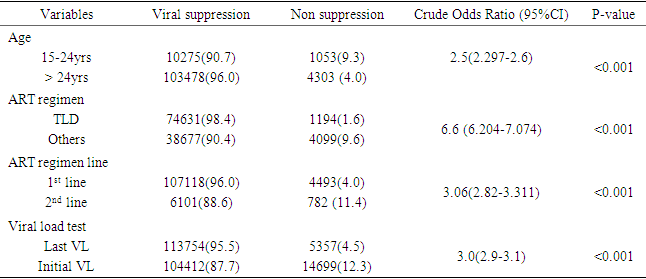
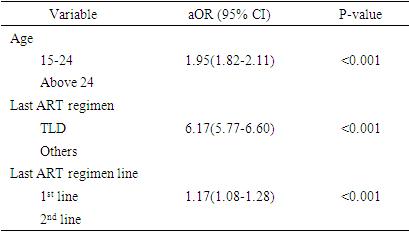
Globally, the 2020 UN targets of 90:90:90 projected that 90% of patients started on Antiretroviral therapy achieve HIV viral suppression (<400 copies) monitored routinely using Viral load test. We evaluated the Case-based surveillance system (CBS) for the viral suppression among HIV positive women of reproductive age (15–49years old) on ART since Kenya is among priority countries for validation of elimination of Mother-to-Child Transmission of HIV & Syphilis. We retrospectively reviewed records from the CBS system in three HIV high burden sub-national levels in April 2021. Revised CDC guidelines were used to evaluate the following attributes; Representativeness, simplicity, completeness and timeliness. Descriptive, bivariate and multivariate analysis of age, drug regimen and regimen line were conducted with odds ratios determined for association with viral suppression. The CBS system is real time obtaining data from Electronic Medical Record systems used in 41% of the facilities (1493/3650) with completeness, reporting rate and timeliness at 87.6% and 84% respectively. We reviewed 119,109 records: mean age was 35 years (± 7.9) with viral suppression of 95.5%. Age group 15–24 years had the lowest viral suppression at 90.7%. Women on TDF/3TC/DTG and AZT/3TC/DTG had highest and lowest viral suppression rates of 98.4% and 66.8% respectively. Suppression on 1st line was 95.8% while 2nd line was 88.6%. The odds of Viral suppression were 6 times higher among women on TLD compared to other ART regimens (aOR: 6.17, 95% CI: 5.77–6.60). Other independent variables included those above 25 years of age and being on 1st line regimen with (aOR: 1.95, 95% CI: 1.82-2.11) and (aOR: 1.17, 95% CI: 1.08-1.28) respectively. Representativeness, simplicity, completeness and timeliness were good. Viral suppression surpassed UN targets though lower for those aged 15–24 years and those on 2nd line. We recommend TLD optimization amongst adolescents and young women.
Keywords: HIV, Surveillance, Transmission, Adolescent
Cite this paper: Sarafina S. Sikwata, Maurice Owiny, Fredrick Odhiambo, Jonah Onentiah, Violet Oramisi, Rose Wafula, Maryan Daud, Esau Langat, Dickens Onyango, A. Abade, Review of the National AIDS and Sexually Transmitted Infections Case-Based Surveillance System for Viral Suppression among HIV Positive Women of Reproductive Age, Western Kenya, 2021, Public Health Research, Vol. 13 No. 1, 2023, pp. 32-37. doi: 10.5923/j.phr.20231301.03.
Article Outline
1. Introduction
- HIV continues to be a major public health issue, with an estimated 38 million people living with HIV AIDS globally as of 2020. (UNAIDS_FactSheet_en_2.Pdf, n.d.) By 2019, there were 1.7 million new HIV infections (the lowest annual number of new infections since 1989), a 23% decline from 2010 attributable to increase in uptake of antiretroviral drugs. (Global HIV & AIDS Statistics — Fact Sheet, n.d.; HIV/AIDS, n.d.; UNAIDS_FactSheet_en_2.Pdf, n.d.) Therefore, WHO recommends that all PLHIV be started on ART as soon as they are diagnosed though only 25.4 million were on ART by end of 2020. (Gibert, 2016; Update of Recommendations on First- and Second-Line Antiretroviral Regimens, n.d.; What to Start, n.d.) The UN Global targets 2020 expected countries to achieve 90- 90- 90 targets; 90% of people living with HIV were to be identified, 90% of those identified initiated on HIV treatment, and 90% of those on treatment expected to achieve viral load suppression. (Fast -Track-Ending the AIDS Epidemic by 2020.Pdf, n.d.) This was further revised to 95-95-95 by 2025. Sub-Saharan Africa accounts for 59% of the global HIV burden of whom young women and adolescent girls accounted for one in four new infections in 2019, despite making up about 10% of the total population. Three in five new infections in 2019 were among women, and the incidence of HIV infections among adolescent girls and young women (aged 15 to 24 years) were 2.5 times more likely than their male peers. (Analysis of HIV/AIDS Epidemic and Socioeconomic Factors in Sub-Saharan Africa - PMC, n.d.; Girum et al., 2018) In Kenya the HIV prevalence among adults (15-49 years) declined from about 10% in the mid-1990s to 4.5% in 2020. (KASFII_Web.Pdf, n.d.) It was estimated that there were 1,401,598 PLHIV aged 15 years and above of whom 1,055,809 were between 15-49 years with 84% (889,547) being women. (KENPHIA-2018-PREL-REP-2020-HR3- Final.Pdf, n.d.) Siaya, Kisumu and Homabay counties had the highest HIV prevalence according to Kenya 2020 estimates at 22.4%, 21.4% and 20.6% respectively. These counties are among 10 counties that had more than 1,000 new HIV infections, accounting for 72% of all new infections in the country. (Kenya’s National HIV Survey Shows Progress Towards Control of the Epidemic. Nairobi, 20th February 2020 – MINISTRY OF HEALTH, n.d.)It is estimated that majority of new HIV infections are transmitted from undiagnosed people or diagnosed people not initiated on ART or those on ART but not yet virally suppressed. (Attia et al., 2009; Undetectable = Untransmittable, n.d.) Early diagnosis, initiation of antiretroviral therapy (ART), behavioral change and viral suppression after initiation on ART among people living with HIV & AIDS (PLWHIV) has shown marked improvement in their health and reduced risk of transmission of HIV to their sexual partners and children. (Changing AIDS Risk Behavior, n.d.; Update of Recommendations on First- and Second-Line Antiretroviral Regimens, n.d.; Cock et al., 2009; Gibert, 2016) HIV being a preventable disease, effective HIV prevention interventions have proven to reduce HIV transmission, morbidity and mortality over the years. HIV Case Based Surveillance (CBS) system involves the individual-level capture of persons diagnosed with HIV infection and routine longitudinal follow-up of cases beyond diagnosis. CBS monitors the transition of the HIV cases through sentinel events that are related to HIV disease progression. Each country determines these sentinel events based on data needs or priorities, data availability and logistics and resources required to collect such data. In Kenya, the following are the sentinel events captured for each individual reported in the CBS database: Diagnosis, Enrollment into care, Initiation on treatment, First and all CD4 counts, First and all VL tests, Changes in ART regimen line and Death. The system pulls data from different sources that capture information on HIV infected persons. The current system is designed to pull sentinel events data from electronic medical records in health facilities, laboratory databases, pharmacy databases, vital statistics registries and other databases that may have information on HIV positive individuals. However, this is being implemented in Kenya in a phased manner; prioritizing data from health facilities. The main objectives for which the system was developed was to monitor individual-level HIV indicators in the HIV care cascade, monitor progress towards the attainment of the 90-90-90 UNAIDS targets, monitor trends in the continuum of care for HIV patients and detect HIV epidemics.Kenya is among 22 priority countries for validation of elimination of Mother-to-Child Transmission (MTCT) of HIV & Syphilis. (EMTCT Framework 2016 2021.Pdf, n.d.; World Health Organization, 2017) This could be achieved if more than 90% of the women of child bearing potential on ART are virally suppressed. We also sought to promote use of available data for public actions and interventions for public health diseases and events therefore the review was to help generate inputs that could eventually improve the efficiency and attainment of the objectives the CBS system was set for and achieve HIV epidemic control. The data analysis could help determine the performance as a country against the UNAIDS 90-90-90 targets and examine the progress towards validation for elimination of HIV infection from mother to child.The study therefore aimed at assessing the Kenya HIV Case Based System against the CDC surveillance system evaluation attributes, describing the HIV positive women of reproductive age receiving Antiretroviral therapy in the three HIV high burden counties in Kenya and determining viral suppression among HIV positive women of reproductive age receiving Antiretroviral therapy in the three HIV high burden counties in Kenya as at April 2021.
2. Methods
2.1. Evaluation Setting
- We reviewed records for the three HIV high burden counties in Kenya; Siaya, Kisumu and Homabay, as at April, 2021. The three counties under review are geographical neighbors located in the Lake region part of Western Kenya along Lake Victoria with the highest HIV prevalence according to Kenya 2020 estimates at 22.4%, 21.4% and 20.6% respectively. (County HIV Estimates 2020_Vs 17 (1). Xlsx, n.d.) These counties are among 10 counties that had more than 1,000 new HIV infections, accounting for 72% of all new infections in the country. They are rated poor by the World Bank in spite of great climate and physical resources. More than 50% of the residents earn less than one dollar per day. The main economic activities include fisheries, agriculture in sugarcane and cotton, livestock production, manufacturing, artisanal mining and the energy sector. (HOMABAY-COUNTY-Strat-Plan_MAY1513_odipo1.Pdf, n.d.) The main factors that promote the rapid spread of the HIV/AIDS in these counties are widow inheritance, negative cultural believes, loose lifestyles among the fishermen, pre-marital sex and night disco dances. (KENPHIA-2018-PREL-REP-2020-HR3-Final.Pdf, n.d.)
2.2. Evaluation Design
- We assessed the Kenya HIV Case based System against the revised CDC surveillance system evaluation attributes of Simplicity, Flexibilty, Acceptability, Sensitivity, Predictive-value positive, representativeness, timeliness, Stability and completeness. Simplicity was measured using the levels of reporting and skills required to collect and interpret data through the flow chart of the surveillance system, uptake by different stakeholders, method of collecting the data, including number and types of reporting sources and the number of variables collected per case. Flexibility was assessed by looking at the ease by which the system accommodated other additional variables and indicators over the last few years and how it survived funding changes if there was any such. Acceptability was measured by the willingness of persons and organizations to participate in the surveillance through the number of facilities using the system, completeness of reports, facility reporting rate trends; default in reporting and timeliness of data entry into the system. Representativeness was evaluated based on the geographical distribution and ownership of the facilities using it. Timeliness was established by considering the average time taken to transmit data from the health facilities up to national level, time taken in analysis and time taken for national level to give feedback to the facilities through dash boards. The time taken to do routine system maintenance was also evaluated. Completeness was calculated using the proportion of missing data in all the variables including the "unknowns" and "blanks". The numerator was those records with the variable available while the denominator was the total number of records captured under that variable (119109).
2.3. Review Design
- We conducted a retrospective data review of records from the Kenya HIV case-based System on women of reproductive age (15-49yrs). We characterized them for sociodemographic characteristics, clinical characteristics and viral suppression status. Such variables included age, residence and marital status, ART start regimen and regimen line, current ART regimen and regimen line, First Viral load, and Last viral load taken. The last viral load done beyond six months on antiretroviral therapy was used to determine viral suppression status.
2.4. Operational Definitions
- Viral suppression was defined as having a viral load of < 400 copies of HIV virus also referred to as LDL while low level viremia (LLV) was when one had viral load of between 400 and 999 copies. One was deemed as not suppressed if they had a viral load of more than 1000 copies.
2.5. Data Analysis
- We conducted descriptive data analysis using MS Excel by calculating measures of central tendency and dispersion for continuous variables and calculated counts, frequencies and proportions for categorical data. For bivariate analysis we analyzed potential factors associated with viral suppression using two by two table. The columns represented the outcome variables while the rows represented the exposure and non-exposure. All factors with a P value less than 0.2 were considered for multivariate analysis. We reported independent factors associated with viral suppression as those with P value less than 0.05; their adjusted odds ratios and their 95% confidence interval was also reported.
2.6. Ethical Consideration
- Permission was sought from National AIDS & STI Control Program (NASCOP) and Palladium the Implementing partner supporting the system. The system de- identifies all records only known by unique identifiers and one can only access the system with authorized password credentials.
3. Results
3.1. Evaluation of the System
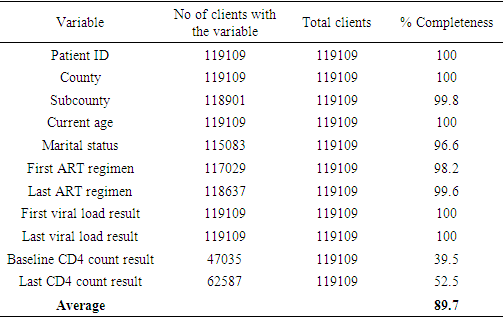
- The CBS system is simple to use as it is real time transmitting data from Electronic Medical Record systems at a click of a button. The system can be modified to include new variables that need to be recorded as advised by the program. The system was being used in 41% of the facilities (1493/3650). The completeness of data in the system was at 89.7% as shown in table 1, reporting rate and timeliness at 87.6% and 84% respectively.
|
3.2. Characterization of the Women of Reproductive Age
- We reviewed 119,109 records: Most of the women whose records were reviewed were aged between 35-44 years with a mean age of 35 years with a standard deviation of 7.9. Majority of the women (43,568) were receiving ART from Siaya with Kisumu and Homabay having 38162 and 37,379 respectively. Awendo Subcounty had the lowest proportion of women receiving ART (0.3%) while Kisumu central had the highest proportion at 12.3%. More than half of the women whose records we reviewed were married (67%).
3.3. Viral Suppression Rates
- The average viral suppression rate among the three counties was 95.5% with Homabay at 95.6%, Siaya at 95.5% and Kisumu at 95.4%. Awendo Sub county in Homabay County had the highest viral suppression rate at 98% while Kisumu west in Kisumu County had the lowest at 93.7%. The viral load suppression was 96% amongst married women compared with 94% amongst the single and divorced. Age group 15–24 years had the lowest viral suppression at 90.7% % compared to other age groups that were above 95% as shown in Figure 1.
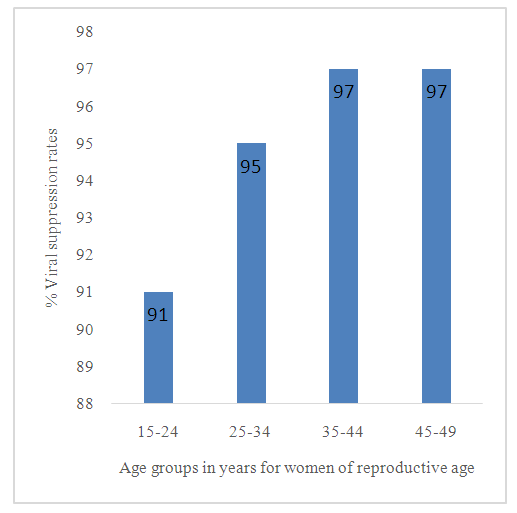 | Figure 1. Viral load suppression rates across different age groups |
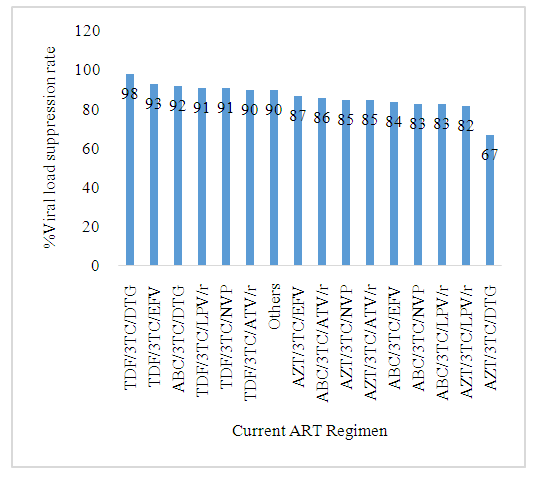 | Figure 2. Viral load suppression rate as per current ART regimen |
|
|
4. Discussion
- The system had data quality issues in terms of completeness especially recording of the CD4 results that was below average. The CBS system was not representative as it only pulled data from facilities that used electronic tools which were less than half of the facilities offering HIV care and treatment services. The mean age of the women was 35 which is the prime age for childbearing. More than half of the women whose records were reviewed were married. Marital status did not have significant impact on Viral suppression. (Rangarajan et al., n.d.) Viral Suppression among women of reproductive age was in line with the WHO recommendation of 90%. (Marinda et al., 2020) The suppression rate was low among 15-24year olds as seen in other studies with low suppression rates among adolescents and young women comparable to a study by Naswa et al on Adolescent HIV/AIDS: Issues and challenges. Indian Journal of Sexually Transmitted Diseases and AIDS. (Naswa & Marfatia, 2010; Rangarajan et al., n.d.) This could be attributed to the adolescent transition effects; as older adolescents tend to be non-adherent to medication. The odds of Viral suppression were 6 times higher among women on TLD compared to other ART regimens as observed several studies quoted by WHO and the Kenya ART guidelines. (Gibert, 2016; Kenya ARV Guidelines 2018 Printable_20thAug2018 Final. Pdf, n.d.) Viral suppression was better among those on 1st line than those on second line similar to WHO information on second line. (Information et al., 2010) This could be associated with poor adherence and drug resistance due to longer periods on ART and retention of the same NRTI. (Idindili et al., 2012)
5. Conclusions
- Representativeness, simplicity, completeness and timeliness were good. Viral suppression surpassed UNAIDS 90-90-90 targets though lower for those aged 15–24 years and those on 2nd line. TLD was an optimal regimen for women of reproductive age with excellent viral suppression rates. The counties were on the right trajectory towards being validated for the elimination of mother to child transmission of HIV as more than 90% of the women on ART were virally suppressed and therefore very minimal chances of infecting their children.
6. Recommendations
- The Ministry of Health with the help of implementing partners through NASCOP to roll out use of electronic system in all counties and health facilities offering HIV and AIDS care and treatment services by the ministry with the help of implementing partners to ensure that the Case-based Surveillance system captures all PLHIV. There should be active and routine update of the information in the system by health care workers to ensure latest information on the client is captured and updated. The program in liaison with implementing partners should plan for routine refresher trainings on use of the system to ensure Health care workers understand all the indicators that are captured and the importance of complete data.NASCOP should facilitate active transition and uptake of TLD amongst women of reproductive age with specific focus on those aged 15-24years.
7. Review Limitations
- The review was based on secondary data that had already been captured and therefore if there were any variables that had been erroneously entered at primary level in the facilities we analyzed it as it were.
ACKNOWLEDGEMENTS
- I would like to appreciate Kenya FELTP faculty and residents for the technical support and guidance through the evaluation and analysis. NASCOP and Palladium were of invaluable support in ensuring availability of data and time to ensure the study was completed.