-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2022; 12(4): 90-94
doi:10.5923/j.phr.20221204.02
Received: Sep. 8, 2022; Accepted: Sep. 21, 2022; Published: Oct. 12, 2022

Caregivers Care Seeking Behaviour for Home Injuries Among Children Between 0- 12 Years in Kaptembwa, Nakuru County, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPhylis Jerotich Kibet
Kabarak University, Kabarak, Kenya
Correspondence to: Phylis Jerotich Kibet, Kabarak University, Kabarak, Kenya.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Unintentional home injuries are a leading cause of mortality and morbidity among children. Approximately 1 million children worldwide die due to injuries yearly and 90% of these deaths are as a result of home injuries. The study aimed at determining the factors influencing the actions undertaken by caregivers towards unintentional home injuries sustained by their children. A cross-sectional study design was used to give a snapshot of events regarding home injuries among children. A total of 305 caregivers were interviewed. Purposive sampling was used to sample Kaptembwa which is an informal settlement with high prevalence of home injuries among children. The sampling frame was households with children between 0-12 years. Systematic sampling with a five skip interval was used to pick the households. Majority 85.12% of the caregivers had inappropriate care seeking behaviour (self-medication, taking no action, seeking help of traditional medicine and resorting to prayers). Only 14.88% of caregivers sought appropriate care when their children sustained injuries. Several factors were found to influence care seeking behaviour of the caregivers. The factors included level of income (P-0.041), perceived severity of the injury (P-0.0045), type of injury (P-0.0039), marital status (P-0.028) and age of caregiver (P-0.047). In conclusion, most caregivers in Kaptembwa had inappropriate health seeking behaviour.
Keywords: Care-seeking behaviour, Caregivers, Home injuries
Cite this paper: Phylis Jerotich Kibet, Caregivers Care Seeking Behaviour for Home Injuries Among Children Between 0- 12 Years in Kaptembwa, Nakuru County, Kenya, Public Health Research, Vol. 12 No. 4, 2022, pp. 90-94. doi: 10.5923/j.phr.20221204.02.
Article Outline
1. Introduction
- Home injuries among children are one of the leading causes of child mortality and morbidity globally [1]. A home injury among children is a global public health concern that accounts for approximately 1 million deaths globally [1]. Several factors contribute to home injuries; however, home environment plays a pivotal role. The nature of childhood development is highly risky in itself. Children of different age categories engage in various activities that may endanger or predispose them to injuries especially in a home environment where they spend most of their time. Appropriate care seeking behaviour involves timely action (within 24 hours) to a satisfied health practitioner [2]. Therefore, appropriate care seeking behaviour if practised by caregivers, would positively impact the lives of the children. Caregivers from slums and informal settlements usually have poor health seeking behaviour caused by many factors such as: low socio-economic status, personal and cultural practices, high illiteracy levels, beliefs and negative attitude towards healthcare providers [3]. Children are usually highly dependent on their caregivers be it biological parents or guardians for their well-being which health seeking when injured is part of it. Hence, proper health-seeking behaviour by caregivers can go a long way in reducing morbidity and mortalities associated with injuries. Therefore, the aim of the study was to determine the actions taken by caregivers when their children sustain injuries at home.
2. Materials and Methods
- Study design and Study population: Cross sectional study design was utilized as it provided a snapshot of the events regarding injuries among children aged 0-12 years and the care seeking behavior undertaken by the caregiver in the community. Only injuries sustained within six months before the period of data collection were termed eligible to avoid recall bias. The study population was caregivers of children between 0-12 years of age. The caregivers must have resided in Kaptembwa for one year prior to the time of data collection. Sample size determination and Sampling techniques: Fisher et al formula was used in calculating the sample size to arrive at a sample size of 305. The Standard Normal Deviate (1.96) which corresponds to 95% confidence level was used. Additionally, an actual prevalence (P) of 50% for home injuries was considered due to lack of documented prevalence [4].Nakuru County was purposively selected among other 47 counties high cases of injuries among children. A total of 2000 injury cases are reported yearly in the County [4]. Kaptembwa informal settlement was purposely selected due to its high incidence of injuries among children according to the Health reports that ranked injuries as number eight cause of mortality among children in the area, and the reported cases are just a drop in the ocean. It was reported that most cases do not reach health facilities. Additionally, Kaptembwa informal settlement is characterized by high population density, poor housing infrastructure, high illiteracy levels and low socio-economic status, which are predisposing factors for home injuries to the children. From a total of 1500 households in Kaptembwa, systematic sampling of every fifth household arrived at by dividing the total number of households in the area by the calculated sample size was be employed.Data collection technique: A structured self-administered interviewer schedule was used to collect data from eligible caregivers in Kaptembwa The questions in the research instruments were arranged systematically to answer the research question and divided into various sections in accordance with the study specific objectives. The questions were written in English and translated into Kiswahili. Five research assistants were well trained on how to administer the data collection tool prior to data collection day. Moreover, the data tool was pre-tested through a pilot study that was done in Rhonda, an area similar to the area of study. The data was collected for a period of two weeks between tenth June 2020 to first day of August 2020. Data analysis and presentation: The data collected was first checked for completeness, cleaned, coding done, then entered into Microsoft Excel and SPSS data analysis software for analysis. Both descriptive and measure of association analysis were done. The descriptive statistics for the study got presented as numerical summaries, tables and charts. On the other hand, Chi square analysis was done to associate the dependent and independent variables. P values of less or equal to 0.05 were considered statistically significant.Ethical considerations: Ethical clearance was given by Kenyatta University Ethical Review Committee. While NACOSTI gave the research permit. Community entry permission was sought from the local leaders, specifically the area chief and community elders. Verbal consent sought from the study participants. The study participants were assured of upholding of confidentiality of information obtained from them. Confidentiality of data obtained ensured through the following strategies: coding of the data tool, not indicating the names of the study participants, and limiting access to identifiable study data. Anonymity of the respondents was also ensured. Additionally, risks and benefits of the study were well explained to the participants. Lastly, the study participants were told that they were free to withdraw from the study if they really wanted after enrolment.
3. Results
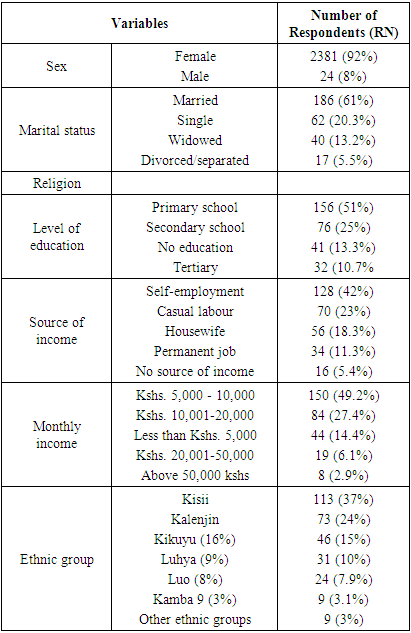
3.1. Demographic Characteristics of the Respondents
- The demographic characteristics of the respondents greatly directly or indirectly influence the actions they take once their children get injuries at home.
|
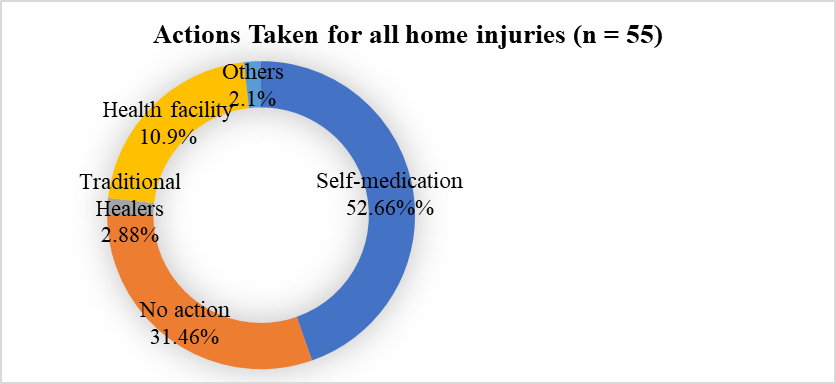
3.2. Actions Taken within 24 Hours by Caregivers after Their Child Sustaining an Injury
- Majority of the respondents 160 (52.66%) chose self-medication, 96 (31.46%) took no action, 33(10.9%) took their children to health facilities, 9(2.88%) took their children to traditional healers while those who opted for Other options such as prayers constituted 6(2.1%) (Figure 1).
 | Figure 1 |
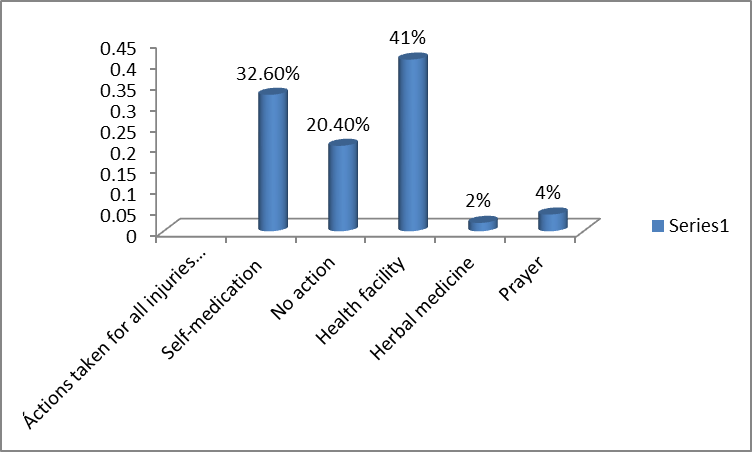
3.3. Actions Taken for Burns
- It was noted that caregivers took different actions depending on the type of injury. For instance, most burn injuries were taken to the health facility (41%), self-medication (32.6%), no action (20.4%), prayer (4%) and herbal medicine (2%).
 | Figure 2 |
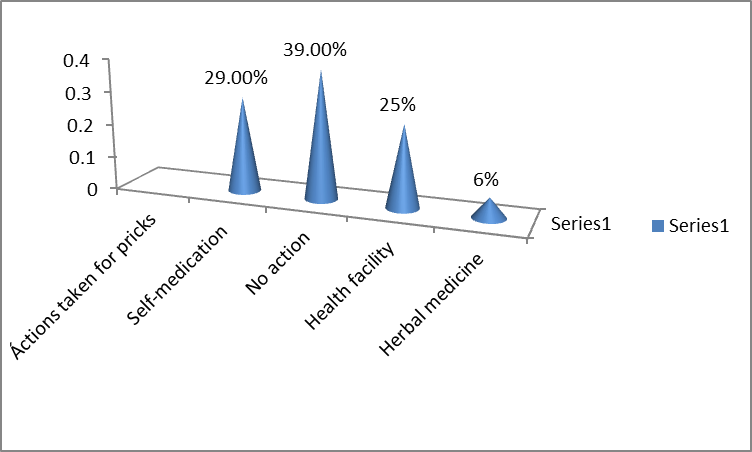
3.4. Actions Taken for Pricks
- Most caregivers (39%) did not do anything when pricks occurred, (29%) opted for self-medication, (25%) opted for health facility and (6%) sorted remedy from traditional healers.
 | Figure 3 |
3.5. Actions Taken for Falls
- Falls seems to have been considered a serious injury with serious consequences if not well attended to. Therefore, most of fall cases were taken to a health facility (46%), no action (26.7%), self-medication (23%) and a visit to herbalist (4%).
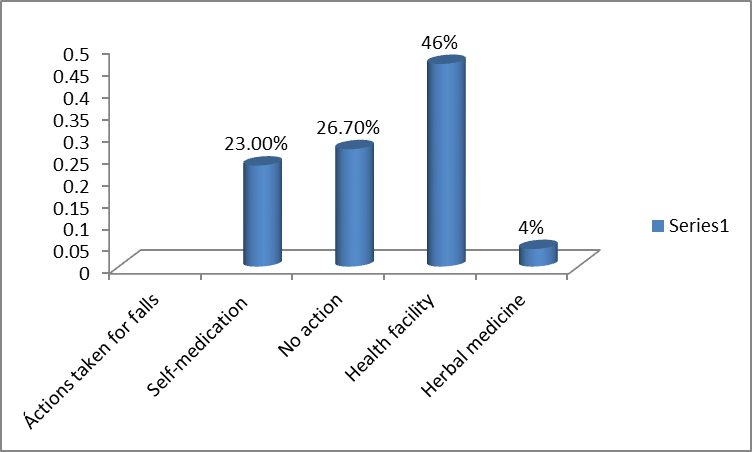 | Figure 4 |
3.6. Actions Taken for Cuts
- With regard to the 55 cases of cuts, (45%) were self-medicated, (30%) taken to health facility, (21%) received no action, (2%) cases received remedy from traditional healers at 1(2%), while (2%) sought other options like prayer.
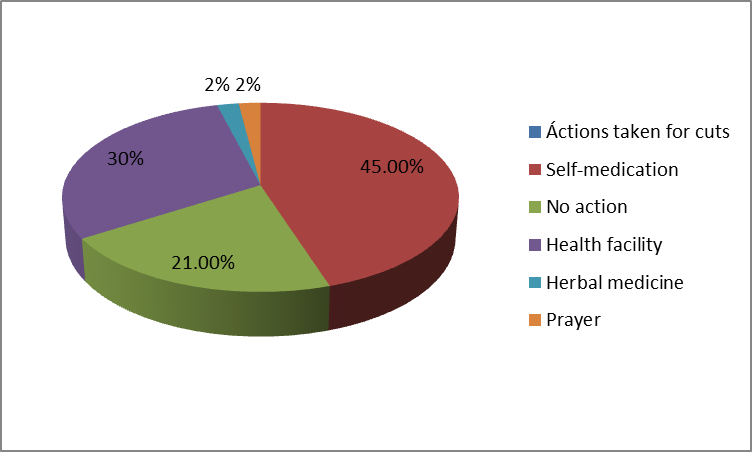 | Figure 5 |
4. Discussion
- All caregivers (n=305) reported that their children had ever been injured at home, once or more than once. Therefore, some of the injuries were overlapping. Health seeking behavior of caregivers directly and indirectly affects the quality of life of their children. Most caregivers in Africa, Kenya included have inappropriate health seeking behavior that include: self-medication, taking no action, choosing herbal medicine or just praying over the injury other than taking the injury case to a medical personnel. The study revealed that majority of the caregivers did not take home injuries sustained by their children as serious as they would do to other illnesses. Generally, majority of the caregivers (89.01%) had inappropriate care seeking behavior while only (10.09%) of caregivers took their children to a health facility for treatment. These results are consistent with those by [6] that found out that most parents in Bangladesh, about two-thirds opted for unqualified service providers for treatment of home injuries of their children. Although the general health seeking behavior was inappropriate, each injury received different attention from the caregivers. For instance, majority of burn injuries were taken to health facilities therefore being an injury that caregivers exuded appropriate care seeking behavior. The study found out that (41%) of caregivers sought medical attention for injuries, a trend that was different from the other injuries. The same findings were found in a study by [6] that found health facility was a choice opted by my parents to remedy burn injuries. The same findings were also found by [7] whose findings revealed that 48% of childhood burns in Ghana were taken to a health facility. Burns is considered a more serious injury and most caregivers comprehend the consequences of untreated burns hence the serious attention given towards its treatment. On the other hand, (45%) of cut injuries were remedied through self-medication, (30%) were taken to health facility, (21%) received no attention while (4%) were remedied through prayers and herbal medicine. Most cut injuries were of either minor or moderate severity and hence most caregivers did not see the need for medical attention. Prick injuries is another type of injury that received the same attention as cuts. The consequences of untreated pricks were deemed not serious or fatal by caregivers hence did not receive medical attention. These results are consistent with those of [8] that found certain injuries like pricks, falls and cuts not being taken to a health facility.Interestingly, education level was found not to be statistically significant with the health seeking behavior (P=0.052). The results were consistent with the findings by [9] who found that educated caregivers tend to self-medicate more than taking their injured children to a health facility. The educated caregivers do so because they are well knowledgeable in matters medicine and can self-prescribe the medication. Additionally, most educated caregivers are busy with white colour jobs and hence have limited time to take their injured children for treatment in a health facility.The findings are concurrent with those by [9] who found no relationship between the level of education and whatever the action the parent took to remedy a home injury sustained by their child. Most socio-demographic factors were found to be statistically significant to health seeking behaviour and hence played a role in influencing the health seeking behavior. The age of the child was found to be statistically significant with health seeking behavior (p-0.021). Most young injured children were taken to health facility or bought over the counter medicine unlike the older children. The results agreed with that of [10] that found that children below the age of five years received medical attention unlike their counterparts. Most caregivers understand that younger children have low immunity and any negligence could be fatal [10]. Additionally, severity determined the remedy action taken by the caregiver. More severe injury cases were taken to a health facility while moderate and minor severe cases were either treated at home or received no attention. Severity was statistically significant at (p-0.045). The level of income of the caregivers was also a statistically significant (p-0.031). The cost sharing policy in Kenya makes health services unaffordable to the socioeconomically deprived caregivers. Hence, most caregivers opt for remedies that are affordable and within their financial reach. A study by [11,12] got the same results, most poor families take treatment more so injury treatment as secondary because they have other pressing issues that need finances. The age of the caregiver was found not to be statistically significant to health seeking behavior (p=0.054). These results differed to the results by [11] that found that older caregivers had inappropriate health-seeking behavior unlike the younger caregivers. Mass media also has a significant role in preventing health hazards for all age groups of mankind. [12]
5. Conclusions
- Caregivers in Kaptembwa informal settlement have inappropriate health seeking behavior. Among all the home injuries sustained by children, only burns received utmost appropriate health seeking behavior in most of the cases. Several factors influenced the care seeking behavior of the caregivers. One of the factors was education level of the caregivers. Ironically, more educated caregivers practiced inappropriate health seeking behavior. The trend by the educated caregivers can be explained by the fact that educated caregivers are knowledgeable in matters drugs and diseases and hence prefer over the counter treatment method. Additionally, educated caregivers are mostly busy in workplaces and lack time to take their children to a health facility. Income status also largely influenced the care seeking behaviour since there are some financial implications of choosing the medical care. The financial implications include transport cost and medical fee. The other factor that also influenced the care seeking behavior includes severity of the injury. Perceived severe cases were taken to the health facility while moderate and minor cases were treated at home or never treated at all. The age of the child also dictated the option of remedy by the caregiver. Most injury cases involving younger children especially below five years were taken to the health facility. The other factor is the marital status of the caregiver; married caregivers tend to exercise appropriate health seeking behavior unlike the single caregivers. The reason could be combined financial efforts and also collective decision making by married couple.
ACKNOWLEDGEMENTS
- I would to sincerely thank the Almighty God for His grace throughout the study. I would also like to appreciate the assistance and professional input by my colleagues at Kabarak University Department of Public Health. Lastly, I would like to appreciate my two supervisors Professor Wesley Too and Justus Osano from Kenyatta University for their role in supervising my work.
Disclosure
- Competing interestsThe author declares that there is no competing interest.