-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2022; 12(2): 51-59
doi:10.5923/j.phr.20221202.03
Received: Mar. 9, 2022; Accepted: May 10, 2022; Published: May 12, 2022

Environmental Sanitation and Hygienic Conditions in Senior High Schools
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLGodfred Safo-Adu 1, Ninette Owusu-Adzorah 2, Charles Essiam 3
1Department of Environmental Science, Faculty of Science Education, University of Education, Winneba, Winneba, Ghana
2Department of Environmental Health and Sanitation Education, Faculty of Science Education, University of Education, Winneba, Winneba, Ghana
3Department of Integrated Science Education, Faculty of Science Education, University of Education, Winneba, Winneba, Ghana
Correspondence to: Godfred Safo-Adu , Department of Environmental Science, Faculty of Science Education, University of Education, Winneba, Winneba, Ghana.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study examined the environmental sanitation and hygienic conditions in Senior High Schools in the Western North Region of Ghana. A cross-sectional survey research design was adopted for the study. A simple random sampling technique was used to select 360 students from three senior high schools. A structured questionnaire was used for data collection. Multiple logistic regression and t-test statistics were used to analyse the data. The study revealed that tap water was the main source of drinking water students (54.4%) used followed by groundwater (22.2%). Also, most students (53.1%) used flush latrine followed by pit latrine (20.0%). Toilets were never covered after use and some too had no lids, as a result, produced offensive odour. Moreover, urinary bays in the schools were untidy and produced offensive odour as well. Stagnant water was found in most schools. A significant proportion of students (83.6%) washed their hands after using toilets with water and soap. However, 1 out of every 16 persons washed their hands with water only. Unwholesome environmental practices such as open dumping and burning were ways schools disposed of their solid waste. The result of the multiple logistic regression showed that there was no statistically significant association between gender and their participation in school sanitation exercise (B= 0.100, Wald test = 0.100, p = 0.752, p > 0.05). The level of environmental sanitation and hygienic conditions in senior high schools in the Western North Region of Ghana was inadequate and needs to be improved. It is recommended that teachers and heads of senior high schools in the Western North Region of Ghana should ensure proper maintenance of toilet facilities and equip students to drain all stagnant water in their schools to improve upon the environmental sanitation and hygienic conditions in the schools.
Keywords: Drinking water, Healthcare planning, Infectious diseases, Sanitary conditions, Waste disposal
Cite this paper: Godfred Safo-Adu , Ninette Owusu-Adzorah , Charles Essiam , Environmental Sanitation and Hygienic Conditions in Senior High Schools, Public Health Research, Vol. 12 No. 2, 2022, pp. 51-59. doi: 10.5923/j.phr.20221202.03.
Article Outline
1. Introduction
- Environmental sanitation encompasses the provision of facilities and services for the safe management of human excreta and solid waste. Improved environmental sanitation contributes highly to healthy living, economic development, social dignity, and general environmental protection [1]. Schools with inadequate sources of drinking water, sanitation, hygienic conditions, and intense levels of person-to-person contact are high-risk environments for students and teachers and exacerbate students’ susceptibility to environmental health hazards [2]. Infectious diseases spread very fast in schools with poor sanitation and hygienic conditions, where many students are together in classrooms for many hours a day. This consequently affects students’ ability to learn [3]. It is estimated that 88% of diarrhoea morbidity is caused by unsafe water supply, and inadequate sanitation and hygiene [4]. In the year 2015, approximately 1400 children lost their lives as a result of diarrhoea [5]. Many schools serve communities that have a high prevalence of diseases related to inadequate water supply, sanitation, and hygiene, where child malnutrition and other underlying health problems are common. Under these conditions, schools become unsafe places where diseases are transmitted [6]. The provision of adequate water, sanitation, and hygiene (WASH) facilities in schools are therefore necessary for ensuring the adoption and maintenance of safe environmental sanitation and hygienic conditions in schools [7] to avert the spread of infectious agents, and enhance students’ wellbeing [8,9,10].Schools often lack drinking water, sanitation, and handwashing facilities. Alternatively, where such facilities do exist, they are often inadequate in both quality and quantity [2]. A study carried out in schools in Zambia revealed that although hygiene educational programmes were present in most of the 132 schools sampled, only 45% of the schools had soap for handwashing, and the impact of hygiene behaviour in the school catchment areas appeared to be limited [11]. Moreover, 5% of the schools had no toilet at all, and the average recorded number of students per toilet was 43.8%. Also, a study carried out on sanitation and hygiene practices of students in urban governmental inter college at Allahabad District, India revealed that only 61.5% of students wash their hands before meals and that sanitation and hygienic practices among students were not satisfactory, hence there was the need for improvement [12]. Furthermore, research work conducted in South-Western Nigeria revealed that out of 12 public schools visited; only 25% had drinking water points and 40% of toilets in the schools were not gender friendly. In addition, only 10% of the schools had handwashing points but without soap and there was no plan in the schools for advancing WASH programmes [13]. Globally, 12% of schools have limited drinking water sources and over 620 million children lacked basic sanitation services at their schools whilst one-third of schools in Sub-Sahara Africa and South-Eastern Asia had no sanitation services [14]. Similarly, it has been reported that about 8% of schools in Jos North Local Government Area of Plateau State in Nigeria never had toilet facilities [15] whilst 8% of schools in Obio-Akpor Local Government area in Nigeria had no water supply while 21.7% occasionally had water supply [16]. In addition, students walked more than five minutes before getting access to water. The situation in schools in Ghana is not different and calls for appraisal. The environmental sanitation and hygienic conditions in most senior high schools in Ghana are not encouraging. This makes the school environment no longer a safe place for students [17]. A significant proportion of rural and urban senior high schools still lack access to adequate sanitation facilities such as toilets and handwashing facilities. The poor environmental sanitation and hygienic conditions coupled with inadequate access to clean water in schools lead to the outbreak of communicable diseases [13] such as typhoid fever, contributing significantly to increase morbidity and mortality [18]. It has been reported that hardly will you come across a dustbin, let alone a handwashing facility in schools in Sefwi-Wiawso, the capital city of the Western North Region in Ghana [8]. Moreover, the schools have few toilet facilities and cannot maintain them, leaving them in a deplorable state. Baseline data on current environmental sanitation and hygienic conditions in senior high schools in the Western North Region of Ghana is scarce. The limited source of information on environmental sanitation and hygienic conditions in senior high schools in the Western North Region impedes identifying priority needs during healthcare planning. This study was designed to fill this gap. This study evaluated the level of environmental sanitation and hygienic conditions in senior high schools in the Western North Region of Ghana. Specifically, the study sought to assess the level of environmental sanitation and hygienic conditions in senior high schools in the Western North Region of Ghana. It also sought to identify methods senior high schools in the Western North of Ghana employ to dispose of their solid waste.The research findings apart from providing baseline information on environmental sanitation and hygienic conditions in senior high schools in Western North Region and adding to existing knowledge would also be useful to municipal and district assemblies in the region when formulating and reviewing policies on sanitation interventions. The following questions were posed to guide the study:1. What is the level of environmental sanitation and conditions in senior high schools in the Western North Region?2. How do senior high schools in Western North Region dispose of their solid waste? The following null hypotheses were tested: Ho 1: There is no statistically significant difference between the mean response of male and female students about their participation in school sanitation exercises.Ho 2: There is no statistically significant association between gender and their participation in school sanitation exercise.
2. Methods
2.1. Setting and Design
- The study was conducted in three senior high schools in the Western North Region of Ghana. The schools were Sefwi Bekwai Senior High School, Oto Memorial Senior High School, and Bibiani Senior High School. The Western North Region is one of the six new regions created in 2019. It spreads from the Ivory Coast border on the west to the Central Region in the southeast and Ashanti and Bono Regions in the north. The population of students in the senior high schools where the study was conducted was 5,490. A cross-sectional survey research design was adopted in the study. A cross-sectional survey is relatively quick, easy, and cheap to perform. Also, it is particularly suitable for estimating the prevalence of behaviour in a population [19]. Again, a cross-sectional survey is good for descriptive analysis and data generation. Data on all variables are collected once and multiple outcomes can be studied.
2.2. Study Participants
- A sample of 360 was estimated for the study using StatCalc in Epi Info Version 7 developed by the American Centre for Disease Control and Prevention, Atlantic Georgia (2010). A simple random sampling technique was employed to obtain 120 final year students from each of the three senior high schools. The final year students were targeted because they had almost spent three years in the school and therefore would have known the environmental sanitation and conditions better.
2.3. Data Collection
- A structured questionnaire was used to collect the data. The questionnaire contained 24 items divided into four sections (Sections A to D). Section A solicited the demographic characteristics of the respondents. Section B collected data on the sources of drinking water and storage options. Section C assessed the type of toilet facility used and hygienic conditions whilst section D sourced information on methods used to dispose of solid waste in the selected second cycle institutions. The instrument was reviewed by experts in the Department of Environmental Science of the University of Education, Winneba to ensure its face and content validity after which it was pre-tested in Senior High Schools in Central Region with similar characteristics like schools in the study area to estimate its reliabilities. The items were subjected to item analysis to identify those whose removal or modification would enhance the internal consistency of the instrument [20]. The Statistical Package for Social Sciences (SPSS) was used to determine the Cronbach alpha coefficient value for the instrument, which was found to be 0.89. Cronbach alpha coefficient value of 0.70 and above indicates a reasonable internal consistency and that alpha value between 0.60 and 0.69 indicate minimal adequate reliability [21]. Moreover, where results are used to make decisions about a group, reliability coefficients of 0.50 to 0.60 are accepted [22]. The questionnaire items were therefore reliable as the Cronbach alpha coefficient value was above 0.70. The responses of participants indicated that they understood the questions and that the wordings of the items were appropriate. An official letter of introduction was obtained from the Western North Director of Education to visit the selected senior high schools in the Region. The consent of the headmasters was sought before collecting the data. Well-trained research scientists from the Department of Environmental Science administered the questionnaires directly to the respondents. The research scientists explained the purpose of the study and any part of the questionnaire that posed a problem to the respondents. All the respondents were assured that the information they will provide would be confidential. Each respondent was given adequate time to complete the questionnaire. The respondents completed the questionnaire on the same day the questionnaires were administered, and a 100% return rate was achieved.
2.4. Data Analysis
- The Statistical Package for Social Sciences software (version 20) was used to organise the data into frequency, counts, and percentages. Also, mean scores and standard deviation of the sample responses were determined. The t-test statistic was used to test for any statistically significant difference between the mean responses of gender groups in the sample while multiple logistic regression was used to examine a possible association between gender and their participation in school sanitation. ‘No response’ was regarded as missing values and so were treated using the imputation technique. Thus, the missing values on a variable were substituted with the mean of observed values for the same variable. This was done to achieve a complete data set on which standard statistics can be applied (Bell et al 2014; Carpenter et al, 2020) [23,24]. According to Leyrat et al. (2020) imputation retains data in incomplete cases that would have been discarded if the analysis were restricted to complete cases, and for imputing values of correlated variables [25]. It also increases the external and internal validity of the research findings [26,27].
3. Results
3.1. Demographic Distribution of Respondents
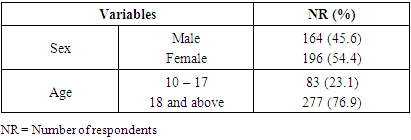
- The demographic characteristics of respondents such as sex and age affect respondents’ participation in environmental sanitation exercise. Table 1 presents the demographic characteristics of respondents in the study area.
|
3.2. Sources of Drinking Water and Treatment Options
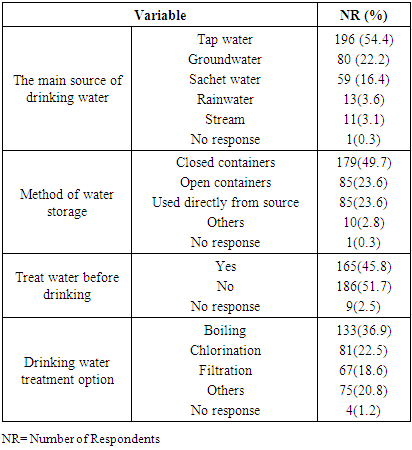
- Safe and readily available water is important to public health. The sources of drinking water and methods employed by respondents to treat their water before drinking are shown in Table 2.
|
3.3. Toilet Facilities and Their Sanitary Conditions
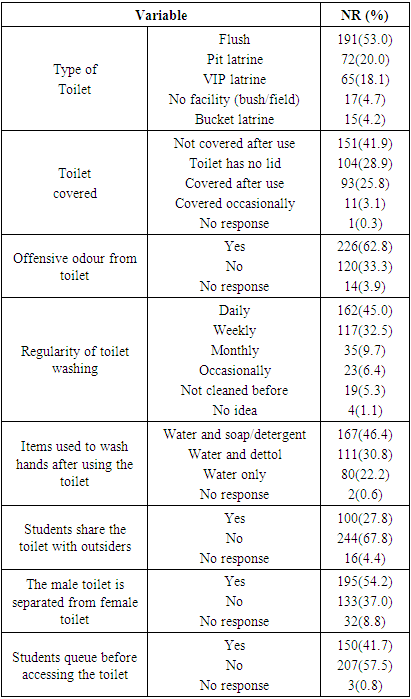
- Adequate provision of toilet facilities coupled with sound sanitary conditions promotes public health. The toilet facilities respondents used, and their sanitary conditions are presented in Table 3.
|
3.4. Hygienic Practices in Schools
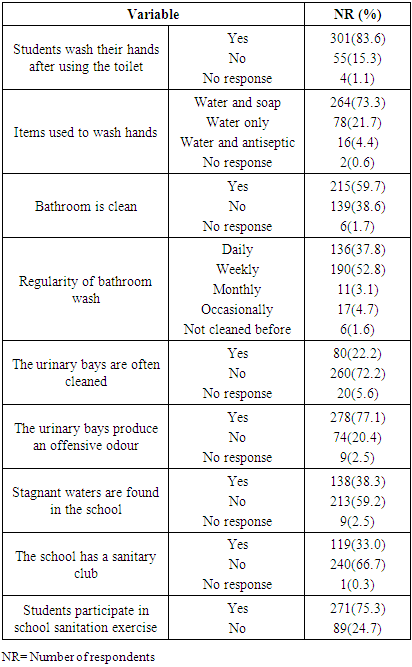
- Proper hygienic practices help avert the spread of diseases and improve public health. The hygienic practices among respondents are shown in Table 4.
|
|

|

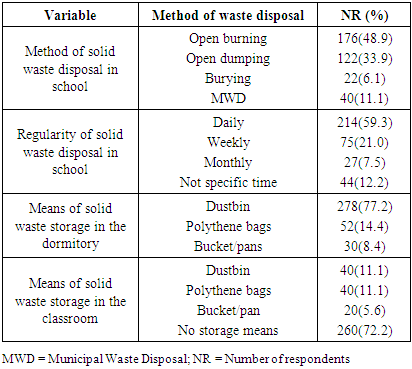
3.5. Solid Waste Disposal Methods in Schools
- Waste disposal is an integral component of the waste management hierarchy. The method employed in schools to dispose of solid waste is shown in Table 7.
|
4. Discussions
- The study evaluated the status of environmental sanitation and hygienic conditions in senior high schools in the Western North Region of Ghana. The female students involved in the study were 9.0% more than their male counterparts (Table 1). Also, most of the respondents (77%) involved in the study were 18 years and above while a few respondents (23.0%) were within the age group of 14 to 17. The study revealed that tap water was the main source of drinking water respondents (54.4%) used, followed by groundwater (22.2%) and sachet water (16.4%). These sources of drinking water when quality could reduce water-borne diseases such as diarrhea and typhoid among respondents by 10% [28]. However, very few respondents used stream water (3.1) and rainwater (3.6%) for drinking. The finding of this study is in contrast with a study conducted in communities in Gomoa East District in Ghana where 72.5% of inhabitants used tap water, 12.2% used sachet water, 6.9% used borehole water, 6.7% used rainwater, and 1.7% used stream water as their main sources of drinking water [29]. It was found that about half of the participants stored their drinking water in closed containers. The few participants (23.6%) who stored their drinking water in open containers might be exposing their water to dirt and pathogens, which exposes participants to a high risk of waterborne diseases after drinking the water [30]. In addition, few participants (23.6%) took water directly from the source for drinking without storage. Again, the finding of this study is in contrast with a study carried out in Akwa Ibom State, Nigeria where 6.1 and 81.2% of respondents stored their drinking water in open and closed containers respectively whilst 10.5% of respondents took water directly from the source for drinking without storage [31]. Similarly, it was reported that people who stored their drinking water in closed and open containers in communities in Gomoa East District in Ghana were about 87.0 and 9.0% respectively [29]. This study revealed that a little above half of the participants (52.0%) never treated their water before drinking. This might expose participants to a high risk of waterborne diseases as untreated drinking water might contain pathogens and other contaminants [30]. Nonetheless, participants who treated their water at the point of use reduced 30 to 50% of waterborne diseases [32]. A little above half of the participants used a flush latrine, which is an improved toilet facility. Notwithstanding, few participants (18.0 to 20%) used pit latrine and Ventilated Improved Pit (VIP) latrine. However, about 1 out of 20 persons defecated in bushes and fields while about 1 out of 25 persons used bucket latrine, even though its use has been banned in Ghana [33]. Open defecation is classified as unimproved sanitation [34] and increases the risk of humans’ exposure to pathogens which could pose significant health risks such as transferable infectious diseases, diarrhoea, typhoid, cholera, and viral infections [35]. The finding of this study is in contrast with a study conducted in schools in Zambia where 23% of students used flush toilet latrines, 40% used Ventilated Improved Pit latrine, and 5% of students had no toilet at all [11]. Similarly, the finding of a study carried out in Jos North Local Government Area of Plateau State in Nigeria, which revealed that 7.5% of students defecated in bushes [15] differs from the finding of this study, which showed that about 5.0% of students defecated in bushes and fields. The findings of the results showed that male and female toilet facilities in the schools were separated, and most respondents (57.5%) never queued before using the toilet facilities. This implied that the toilet facilities in the schools were gender friendly. Again, this finding is in contrast with the study carried out in public secondary schools in Southwestern Nigeria where 40% of the schools never had separate latrines for male and female students. Furthermore, most toilet facilities in the study area produced offensive odour, even though it was scrubbed weekly [13]. Offensive odour emanated from the toilet facilities because they were not covered after use and some too had no lids as reported. This creates the impression of the insanitary state of toilet facilities in the study area. The exposure of students to offensive odour could pose students to high risk of cough, palpitation, nausea, headache, chest tightness, throat irritation, and other toxicological effects [36]. Also, it was found that some participants (46.2%) washed their toilet facilities with water and soap while a few respondents (22.2%) did so with water only. The washing of toilet facilities without soap implies that those toilet facilities were not hygienic and as a result students who used those facilities were exposed to a high risk of infectious diseases such as typhoid fever [15]. In addition, urinary bays in the study area were unclean and so produced offensive odour. Nonetheless, bathrooms in the study area were clean because they were washed weekly whilst few participants washed them daily. The clean nature of bathrooms in the study area will help reduce the exposure of participants to infectious diseases. A high proportion of participants (83.6%) washed their hands after using toilet facilities and did so mostly (73.3%) with water and soap. This was a hygienic practice as it would help reduce over 40% risk of infectious diseases such as typhoid fever exposure [32]. However, 1 out of every 16 persons washed their hands with water only. Furthermore, a little above half of the participants (52.9%) reported having stagnant water in their schools. Stagnant water could provide breeding grounds for insects including mosquitoes [37] and serves as an incubator for bacteria and parasites that transmit diseases [38]. It was also found that most schools had no sanitation clubs. Nonetheless, respondents participated in school sanitation exercises. There was statistically significant difference between mean response of male (M= 1.30, SD = 0.45) and female students (M =1.2, SD = 0.40) in relation to their participation in school sanitation exercise (t =4.415, p= 0.000<0.05). The null hypothesis that there is no statistically significant difference between male and female participants’ mean responses about their participation in school sanitation exercises was rejected. However, the null hypothesis that there is no statistically significant association between gender and their participation in school sanitation exercise (B = 0.100, Wald test = 0.100, p = 0.752, p >0.05) was accepted. The study revealed that solid waste generated in schools was mostly disposed of through unwholesome means such as open burning and a few instances through open dumping. Open dumping and burning of waste pose great environmental hazards and cause natural resources degradation and environmental pollution [39]. The finding of this study differs from the finding of the study conducted in Orlu, Imo State in Nigeria where the commonest solid waste disposal practice among respondents were open dumping (49.8 %) [40]. The participants stored their solid waste in dustbins in their dormitories. Moreover, it was found that most schools (72.2%) had no storage means for solid waste generated in classrooms. This could make students litter classrooms with refuse generated, making the place untidy and unhygienic [18]. All in all, because stagnant water was found in most schools, toilet facilities and urinary bays produced offensive odour, and solid waste generated in schools were disposed of through unwholesome environmental means such as open burning and dumping, the state of environmental sanitation, and hygienic conditions in senior high schools in Western North Region was not encouraging. The inadequate environmental sanitation and insanitary conditions in the study area expose students to infectious diseases [18,41].
5. Conclusion and Recommendations
- The study showed that senior high schools in the Western North Region of Ghana have sanitation challenges. The main source of drinking water students used was tap water (54.4%) followed by groundwater (22.2%), which was mostly treated, through boiling and stored in closed containers. Most students (53.1%) used flush latrine followed by pit latrine, which was washed daily with water and soap. However, toilets were never covered after use and some too had no lids, as a result, produced offensive odour. Urinary bays in the schools were unclean, which as a result produced offensive odour. It was found that the majority of students (83.6%) washed their hands after using toilet facilities with water and soap. However, 1 out of every 16 persons washed their hands with water only. Stagnant water was found in the schools and schools never had sanitation clubs. Unwholesome environmental practices such as open burning and open dumping were the major ways of solid waste disposal in schools. It can be concluded that the level of environmental sanitation and hygienic conditions in senior high schools in the Western North Region was inadequate and needs to be improved.It is recommended that; 1. Teachers and heads of senior high schools in the Western North Region of Ghana should ensure proper maintenance of toilet facilities and urinary bays and equip students to drain all stagnant water on school premises to improve upon the sanitation situation in their schools.2. Heads of senior high schools in collaboration with the Regional Environmental Health and Sanitation Directorate should organise periodic seminars to educate students on good sanitation practices to discourage improper solid waste disposal and open defecation. 3. Teachers at senior high schools should ensure solid waste generated in schools is properly segregated and recycled. Also, students should be encouraged to form sanitation clubs and educate club members on good sanitation practices.
ACKNOWLEDGEMENTS
- We would like to thank the headmasters and teachers in senior high schools in the Western North Region of Ghana for their cooperation and grand support offered during the study.