-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2021; 11(4): 123-131
doi:10.5923/j.phr.20211104.02
Received: Nov. 2, 2021; Accepted: Nov. 23, 2021; Published: Dec. 7, 2021

Correlation of Venipuncture Knowledge, Skills, and Confidence Level with in vitro Hemolysis among Medical Technologists
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJan Bernice C. Talimban, Kashlee Gwyn C. Tan, Pamela Joyce C. Teng, Aubrey Laine A. Santos, Kristine J. San Diego, Felicia Marie L. Advincula, Miguel Carlos G. Arada
Faculty of Pharmacy-Department of Medical Technology, University of Santo Tomas, Manila, Philippines
Correspondence to: Kristine J. San Diego, Faculty of Pharmacy-Department of Medical Technology, University of Santo Tomas, Manila, Philippines.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

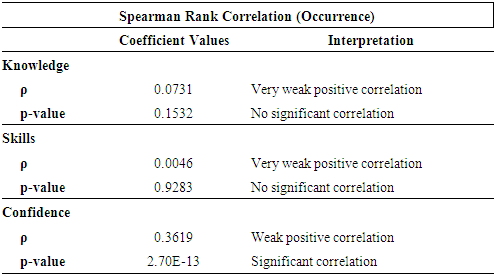
In the Philippines, Registered Medical Technologists (RMT) are the main constituents of specimen collection and laboratory diagnostics. They are highly trained healthcare professionals trained in all areas of the laboratory and tasked to perform venipuncture - one of the most common invasive blood sampling techniques. Venipuncture serves as a vital tool in diagnosing and treating various medical conditions, but despite its importance, it is often overlooked in routine laboratory medicine. Laboratory testing has three phases: preanalytical, analytical, and post-analytical, with approximately 70% of laboratory errors occurring in the preanalytical phase. Among the various preanalytical errors frequently encountered in laboratories, hemolysis was identified as the major source of error and biological interference that compromises the quality of blood specimens. Numerous studies have cited that in vitro hemolysis, specifically, was the common cause of unsuitable specimens resulting in poor analyte determination and unreliable results in the preanalytical phase. It was reported to be dependent on the collection devices, operator's usage of techniques, theoretical knowledge, and compliance to procedures. There are only limited investigations exploring the association of operator-related factors such as their knowledge, skills and confidence levels in performing venipuncture with the likelihood of in vitro hemolysis to occur. To the best of the researchers’ knowledge, none have been conducted in the Philippine setting yet. Therefore, the main objective of this study was to assess the correlation of the RMTs’ level of knowledge, skills, and confidence with the occurrence of in vitro hemolysis during venipuncture procedures. Data from 383 RMTs employed in Metro Manila with one (1) year working experience were selected to participate. Online survey questionnaires using Google forms were used to collect data from March to April of 2021 and were analyzed using Microsoft Excel and R statistical programming language. Findings showed no significant correlations with the knowledge (p-value = 0.15) and skills (p-value = 0.93) in performing standard operating procedures in venipuncture with the likelihood of hemolysis to occur. In addition, a significantly weak positive correlation (p-value = 2.7x10-13) was determined between confidence in performing venipuncture and the occurrence of hemolysis. Similarly, a significantly weak positive correlation was determined between confidence and the variables: educational attainment (p-value = 0.0014), length of practice (p-value = 0.0050), and training attended on phlebotomy (p-value = 0.022). In conclusion, RMTs are highly knowledgeable, skilled and confident in performing venipuncture procedures. However, confidence was the only significant factor that possibly contributed to the occurrence of in vitro hemolysis in venipuncture, while both knowledge and skills in venipuncture did not show a significant impact. Due to the weak correlations determined between variables, further studies are recommended.
Keywords: Medical technologist, Hemolysis, Knowledge, Skills, Confidence
Cite this paper: Jan Bernice C. Talimban, Kashlee Gwyn C. Tan, Pamela Joyce C. Teng, Aubrey Laine A. Santos, Kristine J. San Diego, Felicia Marie L. Advincula, Miguel Carlos G. Arada, Correlation of Venipuncture Knowledge, Skills, and Confidence Level with in vitro Hemolysis among Medical Technologists, Public Health Research, Vol. 11 No. 4, 2021, pp. 123-131. doi: 10.5923/j.phr.20211104.02.
Article Outline
1. Introduction
- Venipuncture is one of the most common invasive blood sampling procedures and is a vital tool in diagnosing various medical conditions [6,7]. Despite its complexity, it is one of the most overlooked routine procedures in laboratory medicine [8]. Based on WHO’s guidelines, accurately performing phlebotomy is one of the paramount steps in preanalytical quality assurance [6]. Some of the frequent factors contributing to unsatisfactory blood specimen quality include lack of knowledge and training, non-compliance of phlebotomists and improper phlebotomy procedures [9]. Improper performance of venipuncture often results in hemolysis, which is defined as accelerated erythrocyte (RBC) membrane breakdown that may result in biological and analytical interference during laboratory analysis [10]. In vitro hemolysis is a notorious problem for diagnostic laboratories due to preanalytical errors in specimen handling and transportation, intra-laboratory processing, and specimen storage [11]. Numerous pieces of evidence have also stated that hemolysis is the most common cause of specimen rejection, occurring in 40-70% of specimens with the prevalence of up to 3.3% in routine specimens [2,13]. Aside from this, it is also highly dependent on the operator and the devices used to draw blood samples [10,12]. Furthermore, the hemolysis of blood specimens can cause significant and detrimental effects on the reliability of the results and patient diagnosis. Quality indicators (QI), which are means to measure the competency and the total testing process of the laboratory, cannot improve quality automatically despite it being the only available mechanism to mediate these errors. Therefore, it is still essential to look into operator-related factors [3]. With this, registered medical technologists (RMT) should possess the knowledge, technical skills, communication skills, analytical decision making, and supervision and management to perform well in any task, such as venipuncture to prevent specimen rejection [14]. Makhumula-Nkhoma et al. conducted a study to determine the association of the relationship between the clinical staff and the phlebotomists' level of confidence in performing venipuncture and their knowledge on the possible causes of hemolysis [15]. The confidence level of the healthcare professionals, based on their staff category and the first and last venipuncture, showed that they were more confident with their last venipuncture. With variable knowledge scores, venipuncture training had a small impact in reducing blood sample hemolysis during the preanalytical phase of laboratory testing. The researchers were able to consider the level of confidence and knowledge as factors that impact the performance of venipuncture and hemolysis. Similarly, Milutinović et al. found a high confidence level with their last venipuncture among all healthcare professionals as well as the number of years of experience and the confidence level among the healthcare professionals [7]. Moreover, most of the participants correctly identified the common causes of in vitro hemolysis. Other factors such as years of experience, educational attainment, and phlebotomy training can also contribute to the RMTs’ performance in venipuncture procedures. Adiga et al. included skills as a factor affecting venipuncture and hemolysis. It was concluded that the number of years of experience does not result in increased knowledge and skills [16].The findings were envisioned to benefit health institutions, RMTs, medical technology students, and future researchers and studies as a baseline study. This research is geared towards improving the role of medical technologists in the standard operating procedures in venipuncture to reduce the occurrence of the major cause of specimen rejection that is in vitro hemolysis. Hence, this study aimed to determine the correlation of knowledge regarding in vitro hemolysis, skills, and confidence level in performing venipuncture with the occurrence of hemolyzed samples among RMTs in Metro Manila. Additionally, to determine the correlation of educational attainment, length of practice, and phlebotomy training attended by RMTs with their knowledge, skills, and confidence level in venipuncture and the occurrence of in vitro hemolysis.
2. Methodology
2.1. Study Design
- This study employed a descriptive quantitative research design, more specifically, a non-experimental survey research. Measurement of variables was performed using a self-administered online questionnaire with the numerical data analyzed statistically.
2.2. Participants or Source(s) of Data
- A total of 383 RMTs working in Metro Manila with at least one year of professional practice participated in the study. Metro Manila was chosen as the region for the collection site as it is where the majority of the country's medical technologist workforce are employed and was also the most accessible to the researchers. The sample size used for this study was determined using Raosoft, an online sample size calculator based on a confidence level of 95% and a 30,000 estimated population.
2.3. Materials or Instruments
- A 33-item online survey questionnaire was created using Google Forms. The study by Makhumula-Nkhoma et al. served as the basis for the questions concerning the knowledge, while the WHO’s guidelines was used as the basis for constructing the skill-related questions [6,15]. Confidence levels were measured using a 5-point Likert scale. The questionnaire was divided as follows: (1) demographic profile, (2) theoretical knowledge, (3) practical skills, (4) confidence level, (5) experience with hemolysis.
2.4. Procedure for Data Collection and Analysis
- A non-probability convenience sampling technique was employed for determining the respondents in this study. The Google form was disseminated through social media platforms from March 15 to April 11 of 2021. To ensure their single response, respective email addresses of the respondents were also collected. For data analysis, Microsoft Excel and R statistical programming language softwares were used. A descriptive analysis was performed on the demographic data and test scores of the respondents to generate frequency, percentage, and average. Additionally, Spearman Rank Correlation, Point Biserial Correlation, and Cramer’s V Correlation were used to correlate the independent and dependent variables.
2.5. Ethical Considerations
- The study’s research protocol was approved by the Faculty of Pharmacy Research Ethics Committee. An informed consent form was provided to the respondents which indicated that their participation was completely voluntary and they may withdraw any time.
3. Results
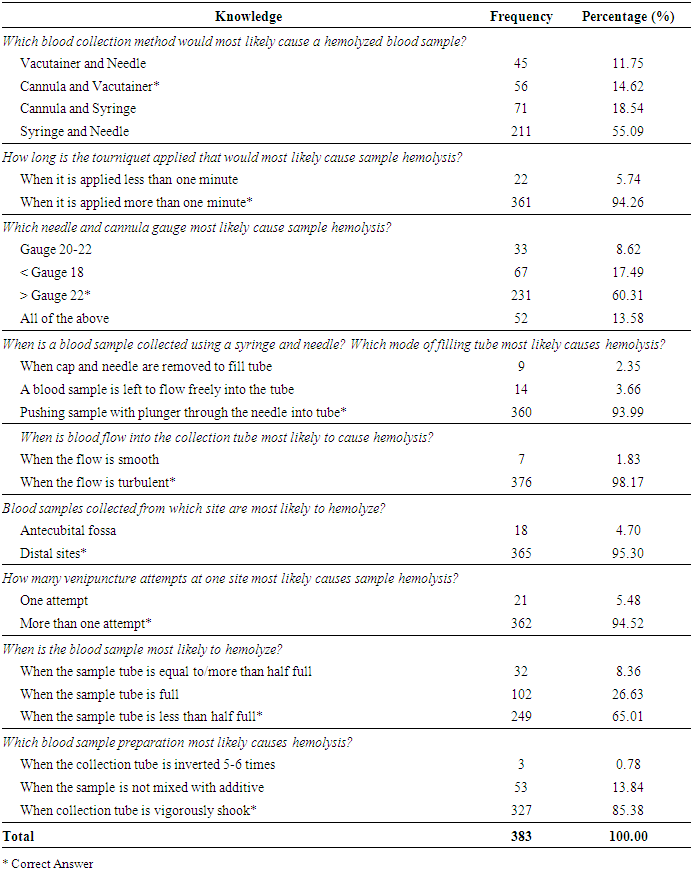
- In Table 1, the frequency and percentage for the knowledge section of the questionnaire are presented. Findings determined that only 14.62% (n=56) of the respondents answered ‘cannula and vacutainer’ correctly for the blood collection method with the majority (55.09%, n=211) answering ‘syringe and needle’ incorrectly. For the remaining items, majority of the respondents answered ‘when it is applied more than one minute’ correctly for the tourniquet application (94.26%, n=361); ‘> gauge 22’ correctly for the needle and cannula gauge (60.31%, n=231); ‘pushing sample with plunger through the needle into a tube’ correctly for the mode of filling the tube (93.99%, n=360); ‘when the flow is turbulent’ correctly for the blood flow (98.17%, n=376); ‘distal sites’ correctly for the site collection (95.30%, n=365); ‘more than one attempt’ correctly for the number of venipuncture attempts, ‘when sample tube is less than half full’ correctly for the blood sample and sample tube (65.01%, n=249); and lastly ‘when collection tube is vigorously shaken horizontally’ (85.38%, n=327) correctly for blood sample preparation.
|
|
|
|
|
4. Discussion
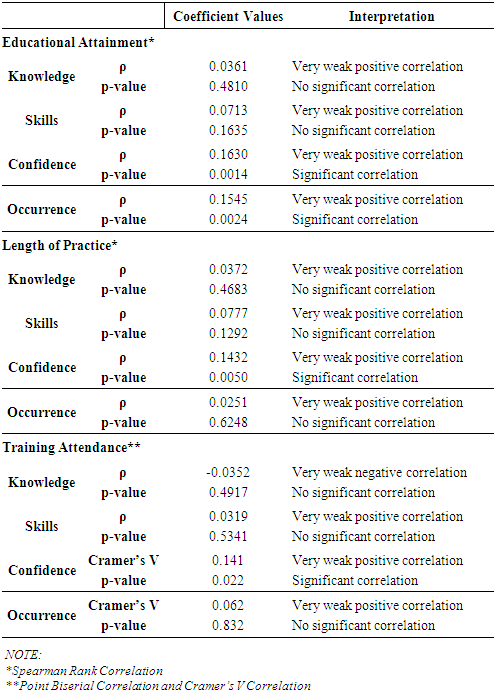
- According to the Human Capital Theory, the more knowledgeable and educated an individual is, the more contributions and accomplishments one has [17]. Contrary to this, the results of the study found that as an RMT’s knowledge increases, the occurrence of hemolysis also increases. Additionally, it was found that as educational attainment and length of practice increase, knowledge also increases. Whereas in terms of training attendance, there was a weak negative correlation with knowledge. It is noted that all of the results aforementioned, were insignificant and weakly correlated therefore, it cannot be concluded that knowledge affects the occurrence of hemolysis and that educational attainment, length of practice, and training attendance have an association with knowledge.Results of the study involving the skillset of RMTs, showed that an increase in skills increases the occurrence of hemolysis. This, however, was reported as insignificant. Fischer's skill theory states that skills can be affected by the context of the task and are developed over time when an individual is exposed to increasing complexity and differentiation in the interactions with oneself and their environment. Differences in the level of knowledge, experience, and environment of each respondent, as well as, the variable SOPs followed may have caused result variability. Furthermore, the educational attainment, length of practice, and training attendance all presented positive correlations with skills although weak and insignificant. Performance relies on factors such as knowledge, skills, and motivation based on the WHO guidelines [6]. Ng and Feldman also stated that educational attainment enables one to be competent to complete tasks successfully. Therefore, education serves as a basis for the skills and productivity of an individual [17].In addition to this, the Social Cognitive Theory states that the social environment determines one’s behavior and confidence [26]. The study has concluded that confidence was the only significant factor that likely influences the occurrence of hemolysis and an increase in confidence also increases the occurrence. This is supported by Woodman et al. which states that a decrease in self-confidence could increase effort, which, in turn, improves performance [28]. Confidence, however, was found to not strongly influence the occurrence of hemolysis due to the weak positive correlation present. With regards to educational attainment, length of practice, and training attendance, an increase in these variables, also increases the level of confidence.Results have shown that as educational attainment increases, the occurrence of hemolysis also increases. This contrasts the statement by Kasika, stating that higher educational attainment leads to better performance, hence the low occurrence of in vitro hemolysis [30]. Even with significant results, the presence of a very weak correlation means that educational attainment does not strongly influence hemolysis occurrence. In addition to this, the length of practice and training attendance both showed an insignificantly weak positive correlation with the occurrence of hemolysis. Therefore the study agrees with knowledge and venipuncture training showing little to no effect in the prevention of hemolysis as stated by Makhumula-Nkhoma et al. [15]. However, it is noted that the association between the factors was found to be weak and insignificant. Lastly, a weak positive correlation between training attendance and the occurrence of hemolysis contradicts the knowledge integration principle which states that by integrating new knowledge, individuals can accumulate knowledge. It should be noted , that in the Philippines, training is supported by the Professional Regulation Commission wherein Continuing Professional Development units are required for the renewal of license for healthcare professionals including medical technologists.
5. Conclusions
- To summarize the findings of this study, the majority of the respondents obtained a high score on knowledge and skill questions, thus were highly knowledgeable on the causes of in vitro hemolysis and skilled in proper venipuncture practices. In terms of confidence levels, RMTs exhibited high confidence levels in performing venipuncture even when presented with challenging circumstances. Among the variables, only the confidence level in performing venipuncture was found to significantly correlate with the likelihood of hemolysis to occur. Likewise, correlation of confidence level with the three sociodemographic variables was revealed to significantly impact confidence level. However, since confidence does not have a strong correlation with the occurrence of hemolysis and with the other variables, it cannot be precisely determined if this has a definitive causative relationship with one another. Furthermore, weaknesses in the methodology of the study may have caused the variability of results. Findings of the study suggest that in order to limit the occurrence of hemolysis, it is necessary to build environmental conditions that are ideal for performing difficult tasks and institutions should aim to standardize SOPs. Increasing the overall confidence of medical technologists may help in reducing the occurrence of hemolysis. In addition to this, undergoing training accreditations, extending practice in the field, and achieving higher educational status, may increase the competencies of medical technologists and therefore, reduce the occurrence of hemolysis. Reaching high confidence is also achieved by increasing the factors aforementioned, however, excessive confidence may affect performance leading to increased hemolysis occurrence. However, obtaining a higher educational attainment may also increase the occurrence of hemolysis. Therefore, it is important to find a balance among all of these factors to improve performance and enhance task outcomes in preventing the occurrence of hemolysis. Future studies are encouraged to improve on this study’s methodology: utilizing a different research design, increasing the sample size, employing a probability sampling technique, and improving the reliability of the questionnaire. The paper focused primarily on the operator-related factors that possibly contribute to the occurrence of the hemolysis of blood samples, specifically their level of knowledge, skills, and confidence in performing standard operating procedures (SOP) for venipuncture, as suggested by the World Health Organization (WHO). Other causes of in vitro hemolysis in specimen handling, processing, and transportation, other operator-related factors, and patient characteristics may also be investigated upon by future researchers.
ACKNOWLEDGEMENTS
- The researchers would like to extend their profound appreciation to their thesis adviser, Sir Miguel Carlos G. Arada, their statisticians- Ms. Febrina Roy Andam and Ms. Zea San Andres, to the University of Santo Tomas Faculty of Pharmacy - Department of Medical Technology, and to their research sponsor, Science Education Institute of the Department of Science and Technology. To God be the glory.