-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2021; 11(3): 99-110
doi:10.5923/j.phr.20211103.03
Received: Oct. 10, 2021; Accepted: Oct. 23, 2021; Published: Oct. 30, 2021

Knowledge, Attitude and Practice of Oral Health among School Students in Balochistan, Pakistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSahibzadi Baloch 1, Sanaullah Panezai 1, Ghulam Murtaza 2
1Department of Geography and Regional Planning, University of Balochistan, Quetta, Pakistan
2Department of Disaster Management and Development Studies, University of Balochistan, Quetta, Pakistan
Correspondence to: Sanaullah Panezai , Department of Geography and Regional Planning, University of Balochistan, Quetta, Pakistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Ensuring good oral health among school students is of great importance because it protects them from dental issues, like bad breath, dental caries, plaque and food-born bacteria. Objectives: This study is aimed to assess the knowledge, attitude and practice about oral health among school students in Mastung district, Balochistan province, Pakistan. Methods: For this cross-sectional study, the knowledge, attitude and practice (KAP) model was used to assess the oral health of school students in Mastung district, Balochistan. For this study, sixteen schools (8 boys and 8 girls) were selected randomly for data collection. The data were collected through questionnaire from 400 students of 9th and 10th class. The data was collected in the month of March and April of 2019. Descriptive statistics and Chi-square test were used to analyse the data. Results: The findings of this study revealed that knowledge about dental caries affect dental appearance, knowledge about importance of tooth care, impacts of bad oral hygiene, knowledge about the dental plague led to dental caries, good impacts of regular use of toothbrush on oral, adverse effects of sweets and soft drinks on teeth, knowledge on oral health and hygiene were greater in male students as compared to female students. In the case of attitude towards oral health, majority of the students believed that maintaining good oral hygiene can prevent teeth decay, visits to dentists for check-up were reported as important as well as the sequence of dental visits and fear of needles and drilling, pain, infection, long waiting time, high cost, no clinic nearby were the important factors due to which they were reluctant to visit dentists. In the case of practice about oral health, majority of male and female students were cleaning tooth once a day. Tools used for cleaning tooth included toothbrush, wooden toothpicks, plastic toothpicks, charcoal and chewstick/miswak, toothbrush was changed once in month, male had more visits than female to dentists for seeking dental care and the reason for last visit to dentist included consultation with dentist, pain or trouble with teeth or gums, treatment/ follow-up treatment and routine check-up/treatment respectively. Conclusions: This study concluded that People’s Primary Health Care Initiative (PPHI) Balochistan should devise a comprehensive strategy for improving oral health and hygiene among school students in the province. Effective coordination between District Education Office (DEO), PPHI Balochistan and District Health Office (DHO) in Mastung district is required for promotion of oral health education at school level. Moreover, trainings are needed for school teachers on spreading awareness about oral health and hygiene, and the community-oriented sessions on oral health hygiene and promotion are very important to improve parents’ knowledge about oral health and hygiene.
Keywords: Oral health, Oral hygiene, School students, Knowledge, Attitude and Practice, KAP Model, Balochistan, Pakistan, PPHI
Cite this paper: Sahibzadi Baloch , Sanaullah Panezai , Ghulam Murtaza , Knowledge, Attitude and Practice of Oral Health among School Students in Balochistan, Pakistan, Public Health Research, Vol. 11 No. 3, 2021, pp. 99-110. doi: 10.5923/j.phr.20211103.03.
Article Outline
1. Introduction
- Oral health, a vital part of general health, refers to a state saving mouth from facial pain, oral sores, oral and throat cancer, birth defects: cleft lip and cleft palate, gum (periodontal) disease, tooth loss and tooth decay, and related disorders and diseases which affect the oral cavity (WHO, 2012). Nutrition, oral hygiene, tobacco use, alcohol use, and general diet are the main factors of oral health illnesses and disorders (Scaglia & Niknamdeh, 2017). Zahid et al, (2014), mention that, in developing countries, the main oral cancer factors are poor infrastructure for healthcare system, poor socioeconomic status, chewable tobacco, betel nut, tobacco, sunlight, alcohol consumption and smoking and the low literacy rate. Most important is the oral hygiene that includes the activities which prevents teeth, mouth from different diseases like bad breath, periodontal diseases, dental caries, plaque and sticky film of bacteria and food forms on teeth (Kabir & Gul, 2013). Globally, oral health issues are of major concern for both the developing and developed countries. However, Al-Omiri et al. (2006) have reported that compared to the Jordanian peers, the children of developed countries have better dental knowledge, attitudes, and health. In today’s fast-changing world oral health issues are in much higher rate among developing and developed countries. Moreover, little is known about the oral health, knowledge, attitude and practice among children in developing countries compared to developed countries (Ahmed et al., 2015).Several studies have highlighted on oral health (OH) among school going students in Pakistan (Khwaja Khail et al., 2019). In Pakistan, research studies have reported that the availability of oral health care is limited (Basharat & Shaikh, 2016), and due to the lacking of oral health services and prevention and control, the burdens of oral diseases exist in the population. According to Mirza et al. (2007), oral diseases are widespread and their prevention and control is poor due to weak oral health care services in the country. Shah et al. (2011) reported that disparities existed in access to oral health care services. Research conducted by Jabeen and Umbreen (2017) shows that majority of the rural areas have low literacy rate as compared to urban areas in Pakistan. Naeem et al. (2016) found in their study that undeveloped oral health care is common in rural areas of country. Research studies have reported that oral health educational programs can minimize the oral health issues (Haleem et al., 2012). Particularly, the initiation of oral health education strategy at school level through educating of teachers can improve oral health situation (Dawani et al., 2013). Schools play vital role in improving the awareness, knowledge and promotion of oral health (Dawani et al., 2013). Teachers are the main source of knowledge and mostly students spend significant time of the day at school with their teachers (Dawani et al., 2013). The study conducted by Khwaja Khail et al. (2019) had revealed the deficiency of knowledge among school children about oral health in Quetta, Balochistan. This study also mentions that no program or activity has been organized health department on oral health at school level. Similarly, compared to the fluoride deficient countries, less frequent dental caries have been observed in children of Quetta, Pakistan (Sami et al., 2016). Oral health care is poor in Pakistan (Basharat & Shaikh, 2016). Majority of the population is school going children, who suffer from dental caries and periodontal diseases. This is an alarming situation as far as oral hygiene is concerned (Jabeen & Umbreen, 2017). Research studies have assessed oral health among children at school level in Pakistan (Jabeen & Umbreen, 2017; Khwaja Khail et al., 2019; Sami et al., 2016; Shah, 2008; Shah et al., 2002). Several studies have been conducted in the context of Balochistan province. Baloch et al. (2013) have reported high prevalence of fluorosis among primary school children in Quetta, particularly in urban areas. Moreover, poor oral health is reported among school children in Lasbela district (Mustufa et al., 2017). Similarly, another study reported low parental knowledge on prevention of oral diseases (Khawaja Khail et al., 2021). Assessment of students’ knowledge about oral health and hygiene is important for the better management of primary health care (PHC) services in the province. Studies have well-documented the low utilization of PHC services in Balochistan (Bazai & Panezai, 2020; Hameed et al.; Naseem et al., 2020; Panezai et al., 2020; Panezai et al., 2017; Panezai et al., 2019). Oral health promotion is the basic mandate of PHC. However, Ali and Panezai (2021) have reported poor dental services at basic health units (BHUs) level in Balochistan. Thus, this study contributes to the body of knowledge by assessing the knowledge, attitude and practice of school students about the oral health in the context of Balochistan province.
2. Methods
2.1. Study Design
- This study employed quantitative methods and has taken Mastung district as case study. The case study design enables researcher to examine the data within a specific context. A limited number of events, situations and their relationship are investigated in case studies through detailed contextual analysis.
2.2. Setting
- Mastung, a rural dominant district of Balochistan province, Pakistan (Rehman et al., 2019), was selected as the study area for this research (Figure 1). 1n 1991, it became a separate district. Earlier it was the part of Kalat District which consists of three Tehsils including Dasht, Kardegap and Mastung. The Mastung district is divided into 12 Union Councils (UCs) for administrative purposes. The ground elevation of Mastung District varies from 934 to 3414 meters above sea level. It is mostly consisted of mountainous, barren and rugged topography. According to 2017 census data, the population of the district is approximately over 266,461 (Pakistan Bureau of Statistics, 2017). The district covers an area of 5,896 square kilometers. Major languages are Brahvi and Balochi, whereas at minor level Pashto is also spoken. The educational conditions of Mastung District are similar to the other districts of Balochistan province. There are a total of 366 schools in Mastung District. Some 91% of the schools are located in rural areas. The literacy ratio among female is low compared to males (Mastung District Education Plan, 2017).
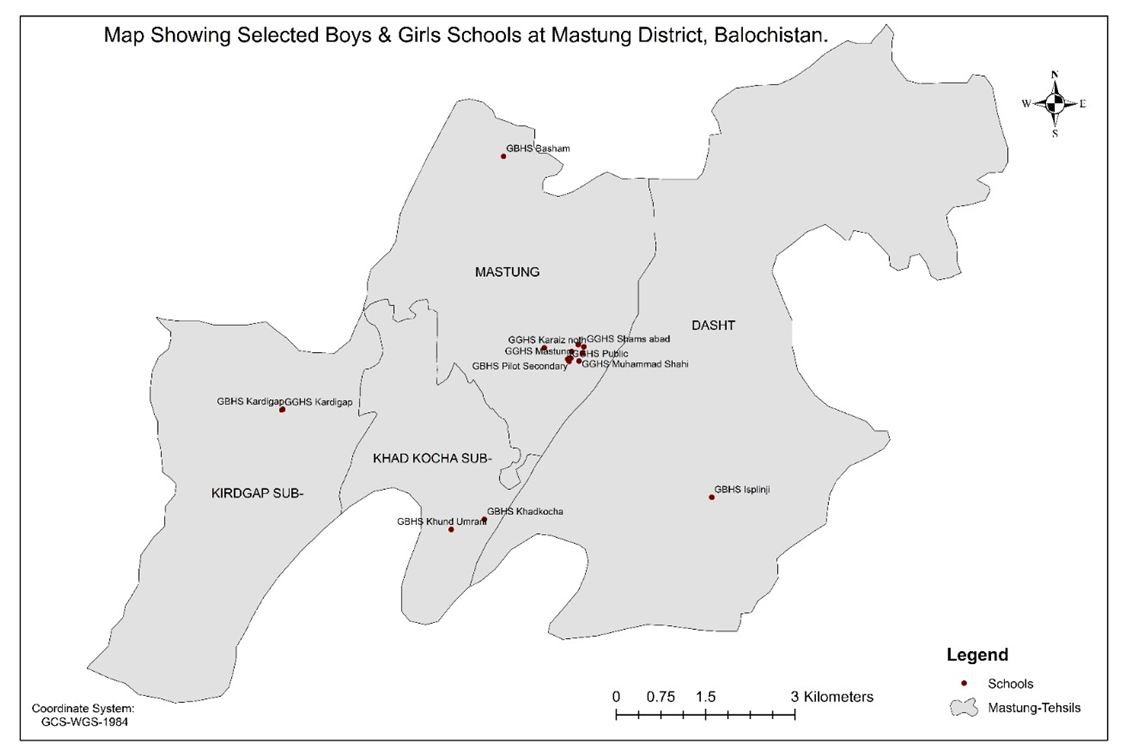 | Figure 1. Map showing Selected Boys and Girls Schools at Mastung district, Balochistan, Pakistan |
2.3. Selection Criteria of Participants
- For this study, male and female students of government high schools of 9th and 10th classes were selected as the participants. Furthermore, the students were selected randomly from the school registers.
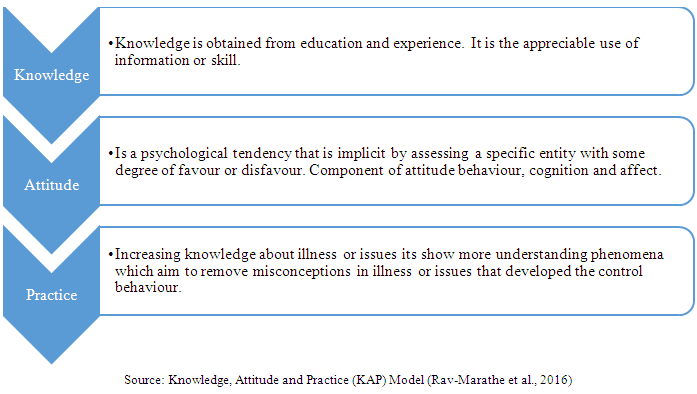
2.4. Knowledge, Attitude and Practice (KAP) Survey Model
- In 1950s, for the first time, the knowledge, attitude and practice (KAP) model was introduced for surveys in the fields of population studies and family planning. According to KAP survey model, “K’ denotes the extent of knowledge about public health issues. ‘A’ represents attitude inwards illness and a health issue, and ‘P’ is used for treatment-seeking practices in the illness or health issues. These are interconnected with each other and directly influences on it (Launiala, 2009).
2.5. Study Variables
- This study has used socio-demographic characteristics and variables related to knowledge, attitude and practice among school students in Mastung district, Balochistan province.
2.5.1. Socio-Demographic Characteristics
- For socio-demographic information, age, gender, class, family size, family type, house type, father’s education, mother’s education, father’s occupation, mother’s occupation, and average monthly household income were the variables used.
2.5.2. Variables on Knowledge
- Variables of knowledge included knowledge on dental carries, knowledge on bleeding gums, dental caries affects dental appearance, importance of tooth care, impacts of bad oral hygiene, regular use of the toothbrush provides a healthy mouth oral hygiene tool, teeth caries affects, treatment of toothache, impact of bad oral hygiene, dental plaque (calcareous) lead to dental caries, sweets and soft drinks affect teeth adversely.
2.5.3. Variables on Attitude
- For variables on attitude, ways to avoid tooth decay, importance of tooth care, importance of dental visits, importance of sequence of visits, fear of not visiting dentists were used.
2.5.4. Variables on Practice
- For variables on practice, frequency of tooth cleaning, tools used for cleaning teeth, changing toothbrush, last visit to dentist, reason for last visit to dentist, taught about oral hygiene tooth and evaluate your oral health were used.
2.6. Data Sources
- The primary data was collected from 16 randomly selected high schools of Mastung District. 8 girl’s high schools and 8 boy’s high schools. The questionnaire was pretested and modified accordingly. The data were collected from students of 9th and 10th class in the month of March and April of 2019.
2.7. Sampling Design
- Sampling design refers to the procedure which is used for the identification of sampling method and sample size. Sampling method refers to the system and measures by which a number of elements of the people are incorporated in the sample (Buckland et al., 2001).
2.8. Simple Random Sampling
- The simple random sampling method was used for the selection of students at school level for this cross-sectional study. In a simple random sample, all samples have the same probability of selection. Firstly, the boys’ and girls’ schools were identified. Then equal number of government schools were selected for the survey. In total, 16 schools were randomly selected through lottery method. Secondly, students were selected randomly from the registers of 9th and 10th classes in the selected schools.
2.9. Sample Size
- In total, there were 366 schools in Mastung District. Out of the total, 126 schools were for girls and 240 schools was for boys (Mastung District Education Plan, 2017). In these schools, the total number of students were 10631 (District Education Office, 2019). For the selection of students as a sample size, this study has used the formula given by Yamane (1967). The formula is given below.
 | (1) |
2.10. Data Analysis Methods
- Descriptive statistics was used for analysis of the data. Moreover, Chi-square test was applied for comparison of the knowledge, attitude, and practices (KAP) of oral health among male and female students in the schools of the study area. For suggestions and strategies for promoting oral health, qualitative analysis was conducted. The quantitative data was analyzed using Statistical Package for Social Sciences (SPSS) version 23.0.
3. Results
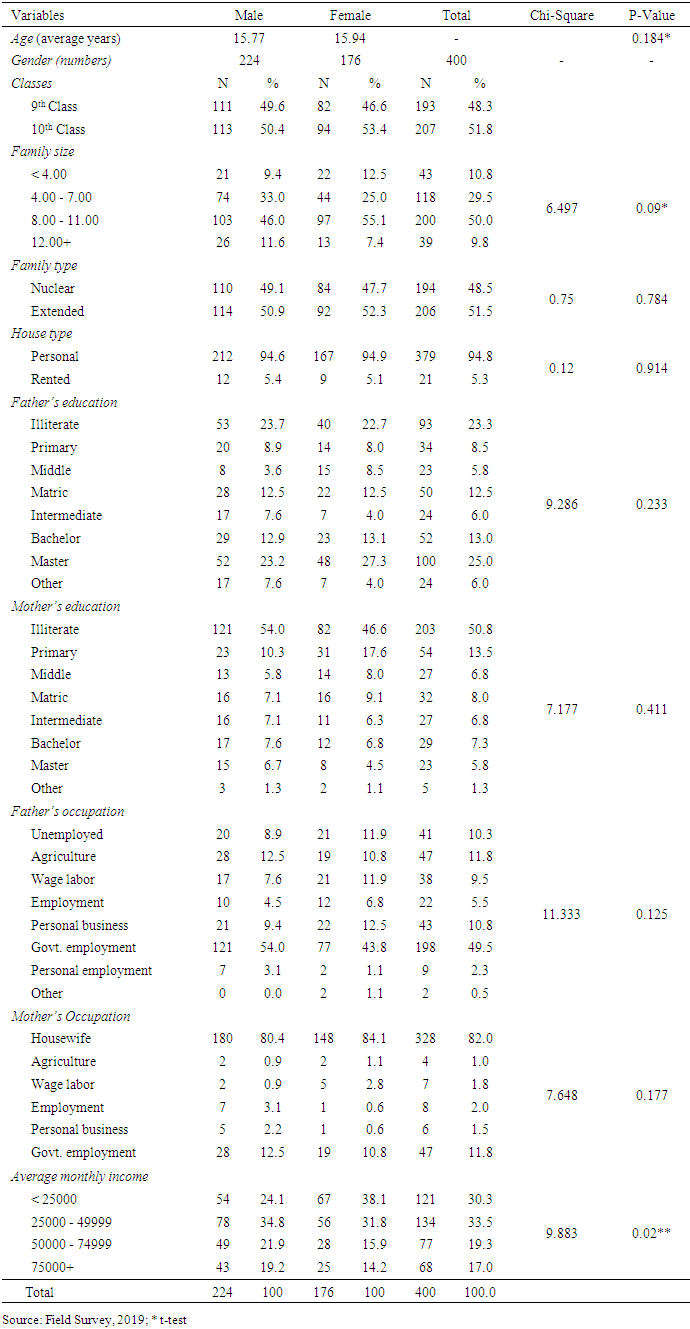
3.1. Socioeconomic Profile of the Students
- The findings in Table 1 demonstrates the socio-demographic profile of the school students. More than half and little less than half of the students were boys and girls, respectively. The family size of Majority of respondent students was from 8 to11. The mothers of the students were twice more illiterate than their fathers. This showed that ratio of illiteracy was high among mothers than fathers of the students. The family type was almost equally distributed among nuclear and extended families. The fathers’ major occupation was government employment whereas majority of the mothers were housewives. There was no significant difference between the occupation of the mothers (P=0.177) and fathers (P=0.125) of students. The average monthly income of the respondents’ households was below 50,000 rupees.
|
3.2. Knowledge of Students about Oral Hygiene Tools
- The findings in Figure 2 showed the knowledge on oral hygiene tools among school going students in Mastung district. The results showed that male students had more knowledge about toothbrush (54.8%) than female students (45.2%). Similarly, male students had more knowledge about the use of miswak (62.4%) than female students (37.6%). Likewise, the knowledge about Dandassa in male was a little more (57.1%) than the female students (42.9%). The knowledge of dental floss was also high 80.0% in male students as compared to female students (20.0%). Overall, the findings showed that male students had more knowledge about oral hygiene tools as compared to female students. Female student needs regular dental training in school level.
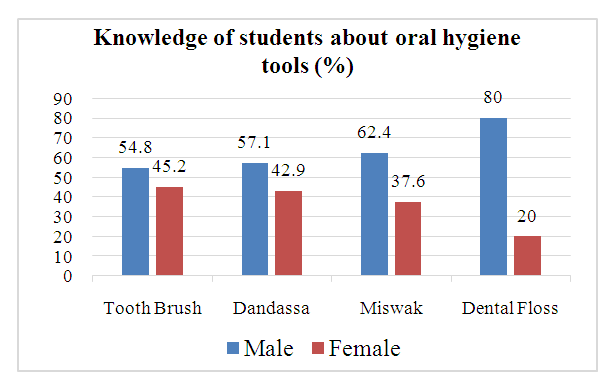 | Figure 2. Knowledge of students about oral hygiene tools (Source: Field Survey, 2019) |
3.3. Knowledge of Students about Dental Caries
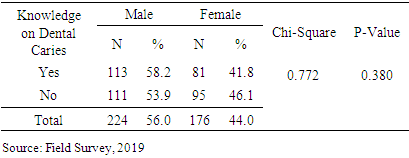
- The findings Table 2 shows knowledge on dental caries among school going students in Mastung district. The knowledge level about dental caries 58.2% in male was high compared to female students (41.8%). However, the difference was not statistically significant. Comparatively, male had more knowledge about dental caries as compared female students. These results imply that dental hygiene should be included in schools’ curriculum for awareness among school students.
|
3.4. Knowledge on Factors Causing Dental Problem
- The results in Figure 3 showed the knowledge on factors causing dental problem among school going students in Mastung district. The findings revealed that more male students (62.5%) were of the view that eating chocolates is the main cause of dental problems compared to female students (37.5%). Similarly, a high proportion of male students (64.9%) were also of the view that the use of tobacco causes dental problems than female students (35.1%). However, in the case of using sugar, female students viewed it as the main cause (65.2%) compared to the male students (34.8%). A little difference was found between male and female students in the case of not brushing regularly where little more than half (56.5%) of male students viewed it as cause of dental problems compared to female students (43.5%). The findings show that both male and female students had sufficient knowledge about the causes of dental problems.
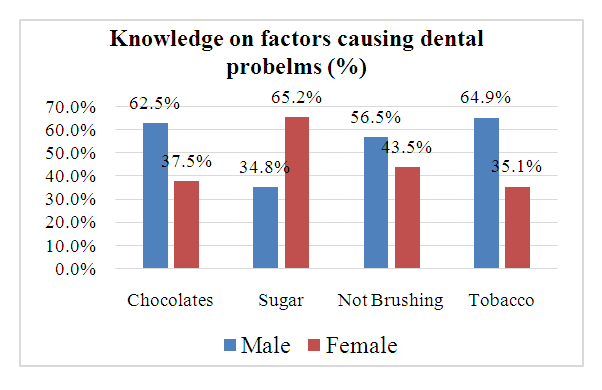 | Figure 3. Knowledge on Factors Causing Dental Problems (Source: Field Survey, 2019) |
3.5. Knowledge of Students about Oral Health
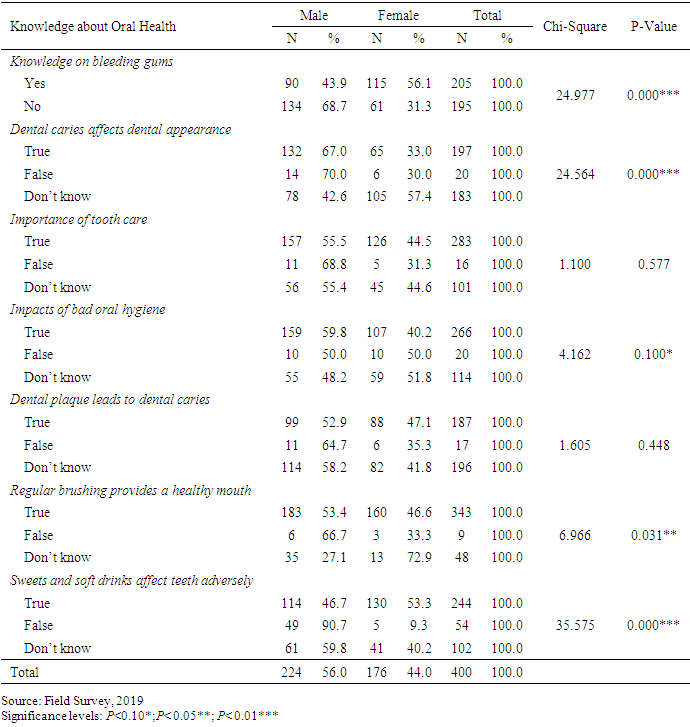
- The findings in Table 3 show the knowledge of school students about oral health in Mastung district. There was significant difference (Chi-square=24.977, P=0.000***) between male and female students on the knowledge about the causes of bleeding gums. A significant majority of the male students had more knowledge about dental caries that affect dental appearance (67.0%) (Chi-square=24.564, P=0.000***). Similarly, knowledge about importance of tooth care was greater (55.5%) in male students as compared to female students (45.5%). In the case of the impacts of bad oral hygiene, having significant difference (Chi-square=4.162, P=0.10*), knowledge among male students was high (59.2%) compared to the female counterparts (41.8%). Similarly, there was a little difference between male and female students’ knowledge about the dental plague (calcareous) lead to dental caries, where little more than half male students had more knowledge than female students. With regard to the good impacts of regular use of toothbrush on oral health, there was a significant difference between (Chi-square=6.966, P=0.031**), and a little more than half (53.4%) male students had more knowledge than female students (46.6%). Almost same results were reported in the case of the adverse effects of sweets and soft drinks on teeth, having a highly significant difference (Chi-square=35.575, P=0.000***) between male (46.7%) and female students (53.3%) in the study area. The analysis of the results showed that comparatively, in the case of knowledge on oral hygiene shows that the knowledge about oral health hygiene is greater in male students as compared to female students.
|
3.6. Attitude of Students about Oral Health
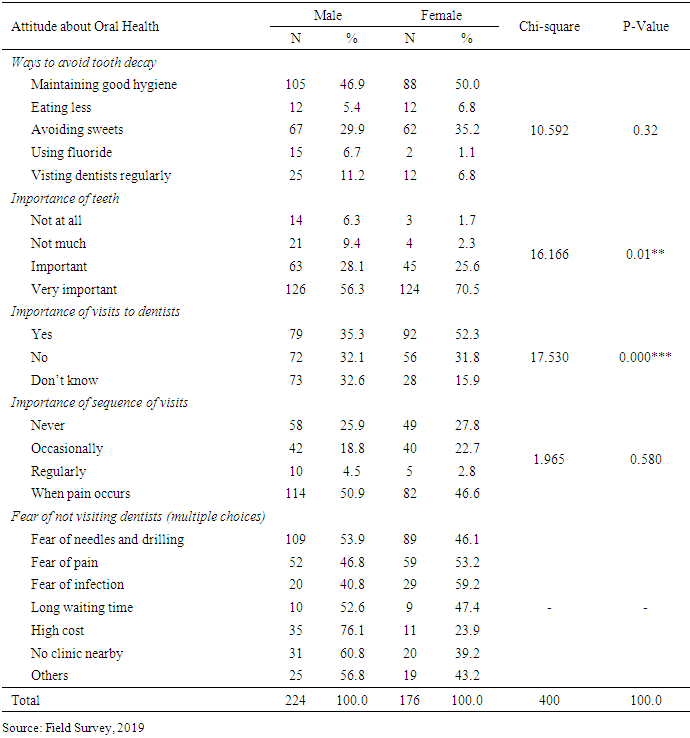
- The results in Table 4 demonstrate the attitude towards oral health among school students in Mastung district. Almost half of the students responded that maintaining good oral hygiene can prevent teeth decay. There was no statistically significant difference (Chi-square=10.592, P=0.32) between male and female students. In the case of importance of teeth, majority of school students ranked it as “very important” i.e., male (56.3%) and female (70.5%). However, the difference between them was statistically significant (Chi-square=16.166, P=0.01***). Similarly, with regard to the importance of visits to dentists for checkup, female students were more positive (52.3%) compared to male students (35.3%). The difference between male and female students was statistically significant (Chi-square=17.530, P=0.000***). Almost similar responses were found in the case of importance of the sequence of dental visits. Majority of male (50.9%) and female (46.6%) reported that they think that dental visits are important only when teeth pain occurs, and had no statistically significant difference (Chi-square=1.565, P=0.580). The attitude of school students for not visiting the dentists was guided by the fear of needles and drilling, fear of pain, fear of infection, long waiting time, high cost, no, clinic nearby and others (Table 4).
|
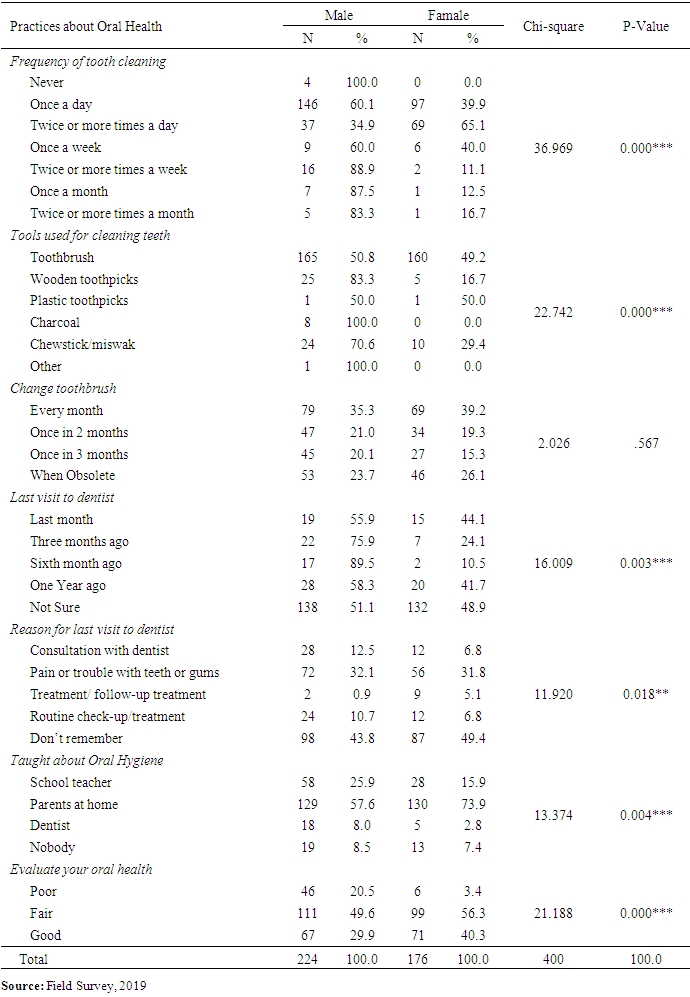
3.7. Practices of Students about Oral Health
- The findings in Table 5 show the practices of school students about oral health in Mastung district. Regarding frequency of cleaning tooth, majority response was once a day cleaning among male students (60.1%) and females (39.9%). The results of chi-square showed that the difference between them was statistically significant (Chi-square= 36.969, P=0.000***). In the case of tools used for cleaning teeth, toothbrush, wooden toothpicks, plastic toothpicks, charcoal and chewstick/miswak were used. However, toothbrush was the highly used tool i.e., 50.8% among male and 49.2% among female students. The difference between them was highly statistically significant (Chi-square=22.742, P=0.000***). The toothbrush was changed once in month, after two-month, three month and when obsoletes by male and female students. There was no statistically significant difference between them. In the case of last visit to dentist, both male and female students did not remember the time. However, male had more visits than female to dentists for seeking dental care and the difference between them was statistically significant (Chi-square=16.009, P=0.003***). The findings show that the reason for last visit to dentist included consultation with dentist, pain or trouble with teeth or gums, treatment/ follow-up treatment and routine check-up/treatment, however, the majority of male (43.8%) and female (49.4%) students did not remember the last visit. The result of the chi-square test shows that the difference between male and female students was statistically significant (Chi-square=11.920, P=0.018**). In the case of teaching about maintaining oral health and hygiene, the highly reported source were parents for both male (57.6%) and female (73.9%) female students. Moreover, the difference between male and female students was statistically significant (Chi-square=13.374, P=0.004***). Lastly, the results show that the evaluation of oral health was ranked ‘fair’ by both male (49.6%) and female (56.3%) students and, the difference between male and female students was statistically significant (Chi-square=21.188, P=0.000***).
|
4. Discussion
- This research was carried to assess the knowledge, attitude, and practices about oral health among school students in Mastung district, Balochistan province. The socio-demographic characteristics of the research was showed that students mostly belong to the lower middle-class households. The average age of the students was below 16 years. The students were living in both nuclear and extended families. Majority of them owned their personal houses. This district is ethically consisted of Baloch, Brahvi and Pashtun tribes. As this study surveyed the government schools for both boys and girls, therefore, gender-based comparison has also been conducted. With regard to knowledge of school students about oral health, majority of the male students had knowledge than female students. Particularly, knowledge about dental caries affect dental appearance, knowledge about importance of tooth care, impacts of bad oral hygiene, knowledge about the dental plague (calcareous) lead to dental caries, good impacts of regular use of toothbrush on oral, adverse effects of sweets and soft drinks on teeth, knowledge on oral health and hygiene were greater in male students as compared to female students. Both had low knowledge about significant factors affecting oral health, particularly female students had low knowledge about oral health and hygiene. This implies that female students need more training about oral health and hygiene. The nutrition, oral hygiene, tobacco, alcohol, and general diet are the main factors producing oral health issues. However, tooth decay and carries can be prevented by increasing knowledge about maintaining good hygiene, avoiding sugary foods, and regular brushing teeth after each meal. In the case of attitude towards oral health among school students, the findings showed majority of the students believed that maintaining good oral hygiene can prevent teeth decay and they ranked teeth as very important part of the body. They findings also revealed that visits to dentists for checkup were reported as important as well as the sequence of dental visits. They also responded that dental visits are important only when teeth pain occurs and fear of needles and drilling, pain, infection, long waiting time, high cost, no clinic nearby were the important factors due to which they were reluctant to visit dentists. In the case of practice about oral health, majority of male and female students were cleaning tooth, once a day, tools used for cleaning tooth included toothbrush, wooden toothpicks, plastic toothpicks, charcoal and chewstick/miswak, toothbrush was changed once in month, after two-month, three month and when obsoletes by male and female students. Moreover, In the case of last visit to dentist, both male and female students did not remember the time, male had more visits than female to dentists for seeking dental care and the reason for last visit to dentist included consultation with dentist, pain or trouble with teeth or gums, treatment/ follow-up treatment and routine check-up/treatment respectively. For maintaining oral health and hygiene, the advice from parents was highly responded compared to school teachers. Lastly, the results show that the evaluation of oral health was ranked as fair. The findings of our study endorse the findings of Dawani et al. (2013) who argued that schools play vital role in improving the awareness, knowledge and promotion of oral health and teachers are the main source of knowledge and mostly students spend significant time of day at school with their teachers (Dawani et al., 2013). Similarly, our findings are in agreement with those of Khwaja Khail et al. (2019) who had revealed the deficiency of knowledge among school children about oral health in Quetta, Balochistan. Moreover, our findings also support the suggestions of earlier studies that have reported that oral health educational programs can minimize the oral health issues (Haleem et al., 2012). Particularly, the initiation of oral health education strategy at school level through educating of teachers can improve the knowledge about oral health situation. Research studies have reported that oral health care is poor in Pakistan (Basharat & Shaikh, 2016). Most importantly, majority of the population in the country consists of school going children, who suffer from dental caries and periodontal diseases. Poor oral health care has made alarming situation of oral hygiene is the population (Jabeen & Umbreen, 2017). Research studies have assessed oral health among children at school level in Pakistan (Jabeen & Umbreen, 2017; Khwaja Khail et al., 2019; Sami et al., 2016; Shah, 2008; Shah et al., 2002). Our findings support the body of evidences that show that in developing country the knowledge about oral health is poor compared to the developed countries as reported by Al-Omiri et al. (2006) who had compared the oral health knowledge of the Jordanian children with those of developed countries. Almost similar findings have also been reported by Ahmed et al. (2015).
4.1. Limitations of the Study
- The study has few limitations. This study was conducted in government schools in Mastung, a rural district of Balochistan province. Health care services in Pakistan are unequally distributed among rural and urban areas. People in rural Balochistan face shortage of oral health facilities, unavailability of dental surgeons. Moreover, the findings of this study may not be equally valid for the children going to private schools. Therefore, caution is needed while generalizing the findings of current study.
5. Conclusions
- Maintaining oral health is essential for a healthy life. The purpose of this study was to assess the oral health knowledge, attitudes, and practices among school students in Mastung District. This study found that overall students had insufficient knowledge, particularly female students had low knowledge about oral health compared to male students. The findings of current study revealed that majority of the student had acquired knowledge and advice from their parents compared to teachers. This shows the weak institutional arrangements about oral health and hygiene at school levels for students. Moreover, the findings also endorse the weakness of primary health care management in reaching the schools children for oral health promotion. The study demands for taking integrated steps for rooting oral health education programs in boys and girls schools in the Masting district. PPHI Balochistan should devise a comprehensive strategy for improving oral health and hygiene among school students in the province. Strategies to improve oral health among school students For promoting oral health, oral health sessions at school level should be managed on regular basis with the coordination of District Education Office (DEO) and People’s Primary Health Care Initiative (PPHI) Balochistan and District Health Office (DHO) in Mastung district. Promotion of oral health education at school level can be initiated with the health of the basic health units (BHUs) staff. Moreover, training for school teachers on spreading awareness about oral health and hygiene should be conducted. For this purpose, PPHI Balochistan should be requested to prepare pamphlets and advertising boards that should be displayed in classes at schools for spreading awareness about oral health and hygiene. Similarly, the role of parents cannot be ignored at household levels. The findings of our study revealed that majority of the students received advise from parents about maintaining oral health and hygiene. For improving oral health knowledge and education, parents can be educated through the Lady Health Visitors (LHVs) who have presence at union council level in both urban and rural areas of the country. Particularly, the community-oriented sessions on oral health hygiene and promotion are very important to improve knowledge about oral health and hygiene. Lastly, oral health education should be made part of school curriculum in order to ensure better oral health and hygiene among school students.
ACKNOWLEDGEMENTS
- The authors acknowledge the support of Mr. Abdul Basit, GIS Specialist who prepared the GIS-based map of schools of Mastung district and Mr. Nadeem Sultan who helped in getting the coordinates of schools for the map.
Declarations
- Funding: This research received no external funding.Conflicts of Interest: No conflict of interest.Ethical considerations: This study involved as such no ethical issues. However, the confidentiality of students was ensured.