-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2020; 10(2): 35-40
doi:10.5923/j.phr.20201002.01

Retention of Bystander Cardiopulmonary Resuscitation Skills: Comparison of Standard and Chest Compression-Only Training Techniques
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Senior Lecturer, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Professor of Orthodontics, Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Senior Lecturer, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Although there are few reports in Nigeria supporting the effectiveness of both conventional and chest compression-only (hands-only) CPR training methods in producing potential bystander CPR providers in our environment, there is no single report on the comparative CPR skills retention rates in Nigeria. This study aimed at assessing the comparative retention of these two common methods of producing by bystander CPR providers for the public. Methods: The study was carried out using a quasi-experimental design with initial cohort of forty-one (41) teachers. Victims of cardiac arrest were simulated using manikins and the teachers, after their initial trainings on CPR skills, were asked to carry out the CPR skills on the victims. Fifteen (15) months later, thirty-one (31) of them who participated in the final re-assessment for retained CPR skills were scored by the same American Heart Association (AHA)-trained instructor, using a modified AHA CPR Skills Evaluation Guide. The AHA conventional CPR training standard was followed and the data analyzed using both descriptive statistics and paired samples T-test. Results: The participants in the two groups comparatively retained good CPR skills 15 months later. However, the hands-only group relatively retained CPR skills with statistically significant better retention of the cycle / min and placement of victim in correct recovery position than the conventional group (P < .001). Conclusion: Both CPR training methods produced satisfactory retention of CPR skills after 15 months of initial trainings but the participants trained using the hands-only method had better CPR skills retention. Recommendation: Either of the CPR training methods could be used to increase the number of potential bystander CPR providers in Nigeria, but preferably the hands-only CPR training method because of its superior effectiveness and efficiency.
Keywords: Comparison, CPR Skills Retention, Standard, Hands-Only, CPR Training Techniques, Nigeria
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Retention of Bystander Cardiopulmonary Resuscitation Skills: Comparison of Standard and Chest Compression-Only Training Techniques, Public Health Research, Vol. 10 No. 2, 2020, pp. 35-40. doi: 10.5923/j.phr.20201002.01.
Article Outline
1. Introduction
- Concerning the usefulness of both standard (conventional) and hands-only (chest compression only) bystander cardiopulmonary resuscitation procedures in providing effective service to victims of out-of-hospital cardiac arrest (OHCA), there is sufficient literature supporting this globally [1-15]. In response to the public health burden of OHCA, many nations of the world have advanced in their published data and practice of bystander cardiopulmonary resuscitation but the story is different in many African countries including Nigeria.In the relatively recent years, Nigeria has some related published data on bystander CPR skills following conventional and hands-only training methods [16-22]. Out of these publications, only two were on retention of skills [17,20] while only one [22] compared conventional and hands-only CPR in a Nigerian population.In pursuant of the desire to popularise bystander CPR and possibly have its teaching and training incorporated in the schools curricula in Nigerian with the expected multiplier effect in potential bystander CPR providers, there is need for more relevant data on this subject. Retention of bystander CPR skills by potential providers after their exposure to the teaching and training remains central in the provision of effective bystander CPR to victims of OHCA. In the Nigerian setting,Hitherto, there is published data that compared the retained CPR skills following different methods of CPR training. The conventional (standard) and hands-only methods are globally recognized as effective methods in training potential bystander CPR providers. Therefore, this study aimed at comparing the level of retention of CPR skills between two groups (cohorts).of participants who previously were trained separately using hands-only and conventional (standard) CPR methods. It was hypothesized that there would be no statistically significant differences in the retained CPR skills in the three common CPR skills domains of the two groups 15 months after their initial trainings.
2. Materials and Methods
2.1. Study Design
- Quasi-randomized experimental design was employed in this study. At the onset of this study in March 2018, the conventional (standard) CPR training group had seventy (70) participants and the hands-only CPR training group also had seventy (70) participants [22]. The two groups were 200-Level undergraduate students of the Department of Human Kinetics and health Education, Faculty of Education, University of Port Harcourt. The same cohorts were recalled and asked to carry out the same procedures they did immediately after their respective trainings 15 months ago. They did not receive any further teaching or training on any form CPR skills before carrying out their procedures again 15 months after. See Appendix for the skills assessed (Note: no airway & breathing skills for the hands-only cohort).
2.2. Immediate Post-training Stage
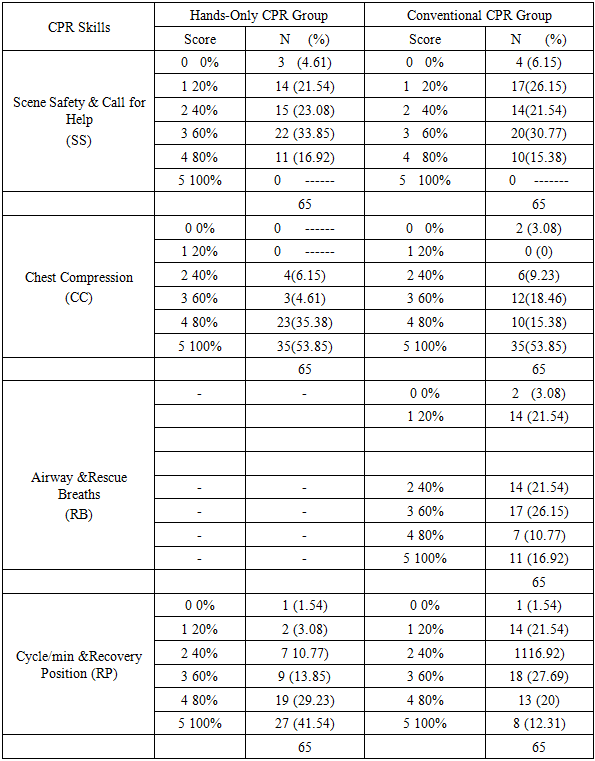
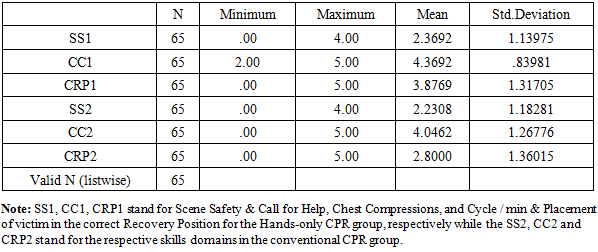
- For conventional CPR training method cohort, using the modified AHA Skills Evaluation Guide, the following four domains of CPR skills were assessed: (1) Scene Safety and Call for Help (SS); (2) Chest Compression (CC); (3) Airway / Rescue breaths; and (4) Cycle /min and Placement of victim in correct Recovery Position (RP). For the hands-only CPR training group, the same domains were assessed except the Airway / Rescue Breaths (ventilation) domain [22].
2.3. Retention Stage or Phase (15 Months Later)
- The same CPR skills domains in both conventional and hands-only groups were re-assessed while maintaining the same standard. The same lead researcher (AHA-certified CPR Instructor) who assessed them while carrying out the CPR skills in their first time (immediately post-training CPR) was the same who assessed them in this later practice (retention phase). During this retention phase, only sixty-five (65) participants were in each cohort (group) with each having fifty (50) males and fifteen (15) females.The following null hypothesis (Ho) was generated and tested: There would be no statistically significant differences in the retention rates of CPR skills between the two cohorts after 15 months of their initial trainings.
2.4. Determination of Good and Poor CPR Skills
- For both cohorts, retained CPR skills of 50% and above were considered as acceptable (Good) while those less than 50% were deemed as unacceptable (Poor).
2.5. Data Analysis
- The Statistical Package for Social Sciences (SPSS) was used in the analysis of data. The matching of the immediate post-training data and the retention data was easily done as teach data collation form used had the matriculation number of each participant. In addition to descriptive statistics used, one sample and two samples T-test were employed. The significance level was set at P < .05.
2.6. Ethics and Participants Consent
- Institutional review and consent was not necessary as the programme was within the course work of the students and was completely non-invasive. In addition, the students were very enthusiastic to participate in the study because of the obvious benefit they would derive from it. In all, the participants freely gave their consent.
3. Results
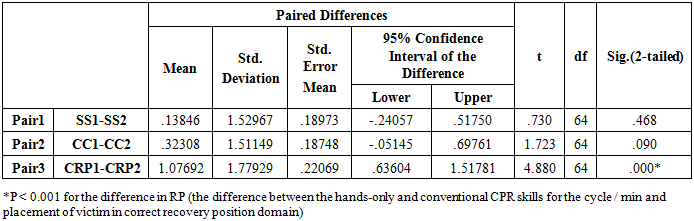
- The age ranges and means for the two cohorts were as follows: 18-31 years with mean of 22.11 + 2.80 (SD) and 18-29 with mean of 22.22 + 2.64 (SD), for hands-only and conventional CPR groups, respectively.Table 1 provides the comparison of the retained CPR skills performance of the participants in the different domains for both training groups with hands-only CPR group having better retention in all the common three domains of CPR skills – scene safety and call for help (50.77% against 46.15%0, chest compression skill (93.84% against 87.69%) and cycle / min and placement of victim in correct recovery position (84.62% against 60%).
|
|
|
4. Discussion
- This Nigerian comparative study on the retention of CPR skills following hands-only and conventional (standard) techniques has shown no statistically significant differences in two out of the three CPR skills domains assessed. The results suggest that generally the hands-only CPR training technique produced superior retentive ability in the participants. To the best of knowledge of the authors, there is no previous report from Nigeria on the comparative retention of CPR skills following conventional and hands-only CPR skills trainings.Kim et al [15] reported that after three months of the initial CPR trainings using hands-only and conventional methods, the hands-only group had significant drop in their chest compression skills unlike the conventional group. They concluded that conventional technique was more retentive of chest compression skills than the hands-only method. Similar to the findings of Kim et al [15] are those of Andresen et al [23], Berden et al [24] and Isbye et al [25]. Our present findings do not support their reports and could be due to the number of months post-training when they re-assessed the retention and possibly the larger number of participants in their training. Our present study re-assessed the retention of the participants 15 months later while they re-assessed theirs just after 2 to 6 months. Also, this type of study does not encourage too many participants at a time so as to carry out proper training initially. In addition, it is important to note that our present study did not record poor skills in relation to artificial ventilation skills in the conventional group even as 15 months after the initial training because quite over half of them retained this skill sufficiently well (60% to 100%) as compared to the Korean study [15]. Meanwhile, our present Nigerian study supports the earlier report of Nishiyama et al [26] where they concluded, based on their findings, that the shortened compression‐only CPR training programme appeared to help the general public retain CPR skills better than the conventional CPR training programme.It is interesting to note that Nishiyama et al [26] re-assessed their retention after 12 months similar to our present Nigerian study. Other earlier studies that our present Nigerian findings are in agreement with are those of Hupfl et al [27], Nishiyama et al [28] and Heidenreich et al [29]. The meta-analysis by Hupfl et al [27] on the chest compression-only and standard cardiopulmonary resuscitation concluded that chest compression-only CPR should be the choice in instructing lay rescuers for adult bystander CPR services However, Nishiyama et al [26] showed that the CPR skills were poor at 6 months after the initial training but better at 1 year period, suggesting the need for refresher courses after 6 months but the cost of such programmes remains a challenge except for personal refresher courses by individuals.Another highlight of our present Nigerian study is the fact that both methods of CPR training produced acceptable retention results after 15 months of initial trainings. This seems to affirm that either of these methods would serve effectively as a means of helping the public retain the needed CPR skills to provide bystander CPR to victims of out-of-hospital cardiac arrest (OHCA) in our environment. Earlier reports have shown that hands-only CPR training is shorter to carry out and produces comparatively effective bystander CPR with conventional CPR training and as such it is much better to provide bystander CPR to victims of OHCA than to leave them alone [4,5,21,26-28]. Our present study seems to support the use of hands-only (compression-only) CPR training for increasing the number of bystander CPR providers in our community. In fact, Lim et al [14] in their retention study involving lay people reported that during the test, conventional CPR groups did significantly fewer chest compressions per minute than Chest compression-only groups (57.8±23.7 versus 77.7±24.2, adjusted p<0.001). Their report [14] further stated that for those who were trained in conventional CPR group, only 3.7% were able to perform ≥10 effective ventilations in 5min. [Bobrow et al [4] in their earlier study also reported that victims of out-of-hospital cardiac arrest (OHCA) who had chest compression-only (hands-only) CPR survived better than those who received the conventional CPR or did not have any form of bystander CPR attention. Strengths and Limitations of the StudyThis Nigerian study could be said to have the merit of being the first in our environment and equally among a very strategic population in the advocacy of increasing bystander CPR awareness in the country. It could also be the first in African continent. However, it is limited by the fact that it was a simulated manikin trial and as such the outcomes might not be exactly the same in real life situation. Therefore, the generalization of the results should be done with some caution.
5. Conclusions
- The two methods of bystander CPR trainings have shown acceptably comparatively good retained CPR skills after 15 months of earlier trainings. However, those who received the compression-only (hands-only) CPR retaining significantly retained better in the skills domain of cycle / min and placement of victim in correct recovery position than the conventional group.
6. Recommendations
- Considering the fact that it is faster to train participants in hands-only CPR and its comparative effectiveness, if not better, with conventional hands-only CPR, we recommend that this method of bystander CPR training should be encouraged in.Nigeria where there is need to urgently increase the number of potential bystander providers because of the current very low number of such trained providers in our communities
ACKNOWLEDGEMENTS
- The authors are very grateful to the participants who showed encouraging enthusiasm throughout the period of this study.