-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2020; 10(1): 12-20
doi:10.5923/j.phr.20201001.02

Maternal Socio Demographic Characteristics are Associated with Child Stunting in Alamura Subcity of Hawassa, Ethiopia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFikadu Reta Alemayehu1, Ruth Gebre Mariam1, Eskindir Loha2, Anchamo Anato1, Derese Tamiru Desta1
1School of Nutrition, Food Science and Technology, Hawassa University Ethiopia
2College of Medicine and Health Science, Hawassa University Ethiopia
Correspondence to: Derese Tamiru Desta, School of Nutrition, Food Science and Technology, Hawassa University Ethiopia.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Stunting remains a problem of greater magnitude than underweight or wasting, and it more accurately reflects chronic malnutrition. In early childhood, it results in diminished cognitive and physical development. Studies indicated that stunting is prevalent and associated with low socio-economic status, low educational level of parents, poor water supply and sanitation, and high infectious diseases burden. Objective: The study was aimed to assess the associated socio demographic factors of stunting among under-five children in Alamura Subcity of Hawassa. Methods: Cross-sectional survey was conducted among 330 under five children. Study participants were selected using systematic random sampling. Pre-tested structured questionnaire was used. Socio-demographic and other determinants were included. Anthropometric indexes were collected from the selected children using well-calibrated weighing scale and height measuring board. Stunting was determined using WHO reference 2007 cut offs. Other data were cleaned for completeness and analyzed using SPPSS V20. Multivariate logistic regression was employed to see association of explanatory variables with stunting. Results: The prevalence of stunting was found to be 29.7%. Maternal education and occupation, age of child and diarrhea episodes were the explanatory variables associated with stunting. An odd of being stunted among the children was 4 times higher from mothers who had no formal education. Housewife’s had 9 times higher to have stunted child with 95% CI (2.49, 33.44) compared with other type of occupation (Merchant and other type of occupation). Childs age was another predictor of stunting. Under-five children with older age (48-59 month) had higher likelihood to be stunted with AOR of 5.15, 95% CI (1.89, 14.02). Diarrheal episode in the last 2 weeks was associated with stunting. Children who had diarrhea in last two weeks were 7.71 times higher odds of stunting compared with children who had no diarrhea. Conclusion: Maternal education and occupation, family size, land ownership and age of the child were the associated socio demographic factors with stunting. Hence, it is suggested to plan nutrition interventions associate demographic factors. Further study to determine other predictors of stunting is also recommended.
Keywords: Stunting, Socio demography, Under-five, Children
Cite this paper: Fikadu Reta Alemayehu, Ruth Gebre Mariam, Eskindir Loha, Anchamo Anato, Derese Tamiru Desta, Maternal Socio Demographic Characteristics are Associated with Child Stunting in Alamura Subcity of Hawassa, Ethiopia, Public Health Research, Vol. 10 No. 1, 2020, pp. 12-20. doi: 10.5923/j.phr.20201001.02.
Article Outline
1. Introduction
- Stunting, a reduced growth rate in human development, is a primary manifestation of malnutrition (or more precisely under nutrition) and recurrent infections, such as diarrhoea and helminthiasis, in early childhood and even before birth, due to malnutrition during fetal development brought on by a malnourished mother. It is an indicator of chronic malnutrition, meaning long-term or accumulated nutritional deficiency resulting from lack of adequate dietary intake over a long period of time and/or recurrent illness. Stunting is defined on the other hand as height-for-age (HAZ) z-score below two SDs of the median WHO standards [1,2]. It is a largely irreversible outcome of inadequate nutrition and repeated bouts of infection during the first 1,000 days of life beginning with conception, through a mother's pregnancy and up until the age of two is the most critical period in a child's development [3]. This irreversible health condition can have an intergenerational effect in which a mother who is stunted may in turn give birth to a small baby, because the fetus's growth in the womb may have been restricted [1,3]. Stunting in early childhood also results in diminished cognitive and physical development, which puts children at a disadvantage for the rest of their lives. They may perform poorly in under five. And as adults they may be less productive, earn less and face a higher risk of disease than adults who were not undernourished as children [4,5]. Height at 2 years of age is clearly associated with enhanced productivity and human capital in adulthood, so early nutrition is also an important contributor to economic development in which a 1% loss in adult height due to childhood stunting is associated with a 1.4% loss in productivity [1]. Progress in reducing childhood malnutrition in developing countries has been slow. The larger burden for Africa is stunting that is the failure to grow in stature. In Africa, this has seen an overall reduction of just 2% in 20 years from 40.3% in 1990 to 38.2% in 2010 [3,7]. Stunting is considered as a severe public health problem in the community when its prevalence in children is greater than 40% (WHO, 1995). In Ethiopia, according to demographic and health survey of 2016, 38% of children under 5 are considered short for their age or stunted, and 18% are severely stunted. Stunting was stable in the first 6-8 months of life, the prevalence of stunting increases steadily from age 9 months through the first4 years of life, before declining slightly in the fourth year of life. Children age 24-35 months had the highest proportion of stunting (48%). It was slightly higher among male than female children (41% versus 35%). Greater prevalence was found to be among children in rural areas (40%) than urban areas (25%). There were some regional variations; it ranges from a high of 46% in the Amhara region to a low of 15 % in Addis Ababa. According to the survey, mother’s education and wealth quintile are both inversely related to children’s stunting levels. More than 4 in 10 children born to mothers with no education (42%) are stunted compared with 18% of children whose mothers have more than a secondary education. Similarly, stunting decreases from 42% among children in the lowest wealth quintile to 27% of those in the highest wealth quintile [8]. It was also documented that in the north western Ethiopia, stunting was correlated with child age, occupational status of household head, family size, and fathers’ education [13].In general there are several factors thought to be causes for stunting in Ethiopia. Stunting correlates with demographic and socio economic characteristics including wealth index, education of caregivers and age of child [9,24,10]. Environmental and health care characteristics including drinking unsafe water and immunization also account for stunting [27]. Whereas, dietary factors are the majorly associated factors for stunting. The major dietary factors encompasses suboptimal breastfeeding and complementary practices [11,27]. In addition of the aforementioned factors, stunting is greatly dependent on several factors including socio-culture, livelihood, and different residence settings. However, to the date little is known about the causative factors within these contexts specifically in the urban settings of Ethiopia. This study is therefore, aimed to identify socio economic, demographic and other associated factors of stunting among under five children in Alamura kebele Tula sub city, Hawassa, Ethiopia.
2. Materials and Methods
2.1. Study
- The study was conducted in Hawassa, capital city of Southern Nations, Nationalities and Peoples Region (SNNPR) and Sidama Zone. It is located at 70’ 03” latitude and 80’29” east longitude. It is bordered by Wondo Genet District in the East, South Dore Bafeno District in the South, by Oromia region in the North, and by Hawassa Lake and Oromia region in the West. The city is divided in to 8 sub cities and 32 kebeles. According to the report of Housing and Population Census, the projected population of Hawassa city Administration in 2011 was 374,034 out of which 190,757 were males and 183,277 were females. The annual population growth rate is 4.02% [6]. The study was conducted in Alamura subcity. The subcity was selected randomly from the existing sub cities.
2.2. Study Population and Sampling
- A community based cross-sectional study design was conducted to assess the prevalence of stunting and associated factors in under five age children from May to September, 2017. The study population comprises of children 6-59 months of age who lived with their mothers in the Alamura kebele Tula sub city of Hawassa. All children 6-59 months of age who lived with their mothers and whose mothers where available in the selected households was included in the study. Conversely, children whose mothers were both critically ill and unable to respond for the interview and disabled children because of inability to give physical measurements as well were excluded from the study. A total of 330 sample size using single proportion formula was calculated based on study conducted among under five children in Hawassa Zuria district [14]. Systematic random sampling method was used to recruit Under-five children who live in the sub city. Considering two months’ study period, 1683 household were expected to visit during the study period based on the kebele statistics and document review. This number was divided for the sample size to get the sampling interval (k value) which was found to be 5.1. Of the first four house hold, one was randomly selected by lottery method, and then every 5th household was selected to participate in the study until the calculated sample size was achieved within two months of data collection period.
2.3. Variables
- Key variables as per the objective of the study were identified. Prevalence of stunting was considered as dependent variable. Whereas socio-demography, environmental characteristics, dietary and health care factors were the considered as the major independent variables.
2.4. Data Collection Procedure and Analysis
- In this study data were collected by trained data collectors with supervisions of the researcher. Prior to data collection, training was given for data collectors for four days on method of extracting the needed information through interviewing, how to fill the information on a structured questionnaire and the ethical aspect in approaching the care givers. Structured questionnaire was used to collect data on demographic, socio-economic, environmental, healthcare and dietary characteristics among children age (6- 59months) from Alamura kebele Tula subcity, Hawassa. The structured questions were developed through review of literatures. English version questionnaire was developed. Later, it was translated to Amharic language and again translated back to English to check by experts who are fluent in both languages to check consistency. To determine stunting data on age, length and height of the child were collected. Length measurement for children below 24 months was taken in laying down or recumbent position and standing height was taken for children 24-59 months and the measurement was taken to the nearest 0.1 cm using Short's Height Measuring Board (Short Productions, Woonsocket, RI, United Kingdom), with the subjects shoeless [15]. The child's age was collected from the mother and confirmed by using birth certificate or vaccination cards and also we was use a "local-events calendar" [5,15]. In order to achieve a good data quality; pretesting the questionnaires prior to data collection was conducted. Later, actual data collection was done by experienced enumerators. The collected data was undergone for data entry and cleaning by using SPSS V20 and anthropometric measurements were entered in WHO Anthro 2008. WHO reference 2007 cut-offs was used for comparison of the prevalence result. The anthropometry measurement of height for age (HAZ) was calculated through ENA SMART software, and children less than -2 SD were classified as stunted. Those children with HFA indices between -2 and -3 SD were classified as moderate stunting while < -3 SD were classified as severe stunting. Data was also exported to SPSS version 20 for further analysis and identification of factors associated with stunting [13].The descriptive statistic was carried out to compute the different frequency, percentage and different diagrams. To determine the actual predictors for the stunting, binary logistic regressions was applied. The variables found to have association with the outcome variable at p-value <0.05 were entered into multivariate analysis which for controlling confounding factors. Finally, the variables which have significant association were identified on the basis of p-values at 0.05 and AOR, with 95% CI to measure the strength of the associations.
2.5. Ethical Considerations
- Ethical clearance was obtained from Ethical Review Board (IRB) of Hawassa University. Following the clearance, the purpose of the study was explained in detail to the respondents and their consents were sought. Study participants were involved in the study based on their agreement. Information obtained from the respondents was kept confidential. At the end of data collection, nutrition education was given for the caregivers. The emphases of the education were on child health (proper nutrition, exercise, personal hygiene) and child nutrition for those who are interested after data collection.
3. Results
3.1. Demographic and Socio-economic Characteristics
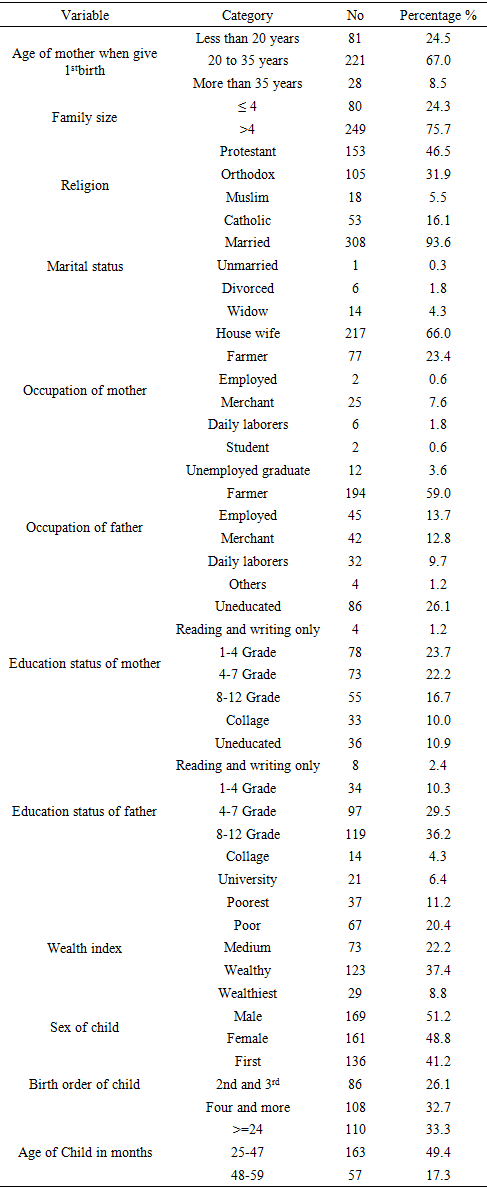
- A total of 330 children aged 6-59 months were included in the study with 100% response rate. The mean of mothers’ age in completed years was 28.55(SD ± 6.457). Mothers in the age interval of 25-29 were dominant and accounts about 93 (28.3%). Majority, 308 (93.6%) of mothers were married during the time of survey. More than half, 221 (67.0%) of mothers reported that they gave their first birth at the age interval of 20 to 35 years. Of the 330 under-five age children, 169 (51.2%) were male and 161 (48.8%) were female. The mean age of children was found to be 38.73(SD ± 10.13) months.From over all 330 participants mothers, 153 (46.5%), 105 (31.9%), 18 (5.5%) and 53 (16.1%) were Protestant, Orthodox Muslim and Catholic religion followers respectively. With regard to education, (29.4%) mothers had attended grade 8 and above and the rest 86 (26.1%) were did not attend any formal education (Table 1).
|
3.2. Prevalence of Stunting and Other Nutritional Indices of Under Five Children in the Study Area
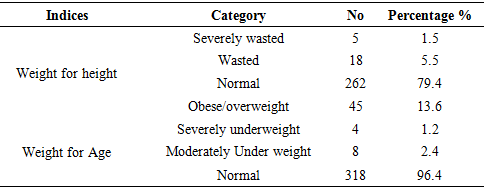
- In this study stunting was defined as having a-z score below – 2 SD of the WHO standards. Overall prevalence of stunting in Alamura kebele Tula sub city was found to be 98 (29.7%) with 95% CI (24.6%, 34.8%). Prevalence of severely stunted children was 37 (11.2%) with 95% CI (7.7%, 14.8%). Among the total, 262 (79.4%) were normal for weight-for-height indices. More than five percent of the children 23(6.69%) were low for weight for height indices (Table 2).
|
3.3. Health Care Characteristics
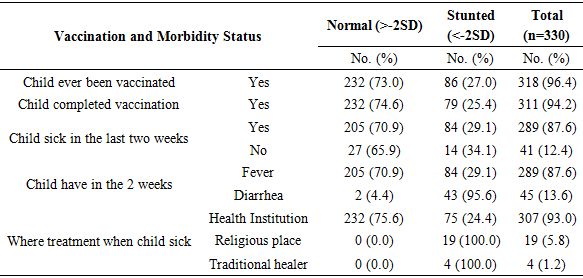
- Out of 330 under five age children participated in the study, 311 (94.2%) were fully immunized during the time of survey. Among the children, 289 (87.6%) experienced illness in the last two weeks at the time of survey. The majority, 289 (87.6%) had got diarrhoea during two weeks’ period prior to data collection and 289 (87.6) got fever (Table 3).
|
3.4. Dietary Habits
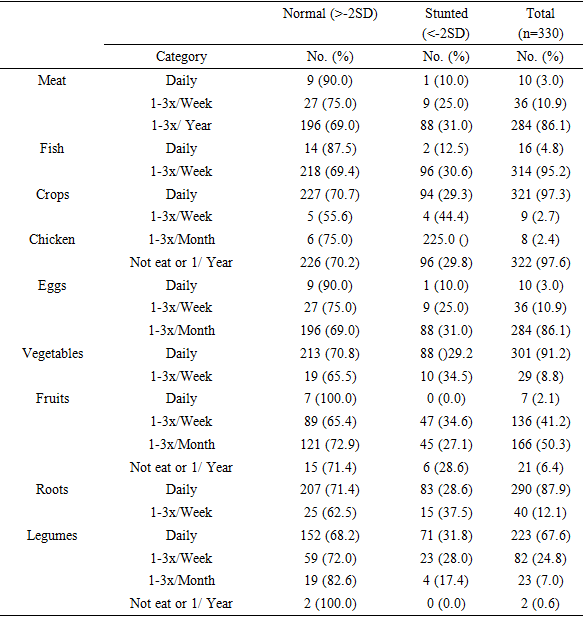
- More than three fourth of the under five children consumed meat and meat products 1-3 times a year. Only 16(4.8%) of the children consume fish on daily basis. Majority 321(97.3%) of the children consume crops variety of food on daily basis. Less than half of the under five children consumed fruit products on daily or 1-3x/Week basis. With regard to vegetable consumption, almost more than 90% consume daily (Table 4).
|
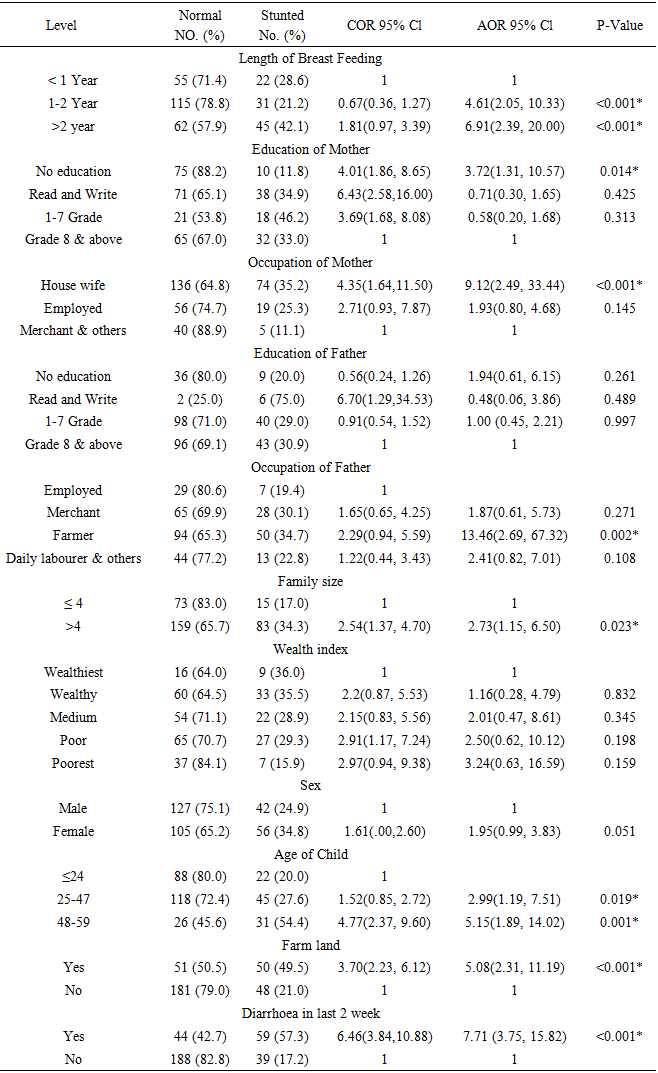
3.5. Factors Associated with Stunting
- Binary logistic regression analysis was conducted in order to identify the candidate socio demographic variables. During binary logistic regression analysis, educational status of father and mother, family size and wealth index variables were the associated socio demographic factors. Following binary logistic regression multivariate analysis were conducted. As Table 5 describes the odds of having stunting child was 3.72 times higher in mothers who had no formal education at 95% CI (1.31, 10.57). The under five children whose mothers are housewife compared with other types occupation were 9 times higher to be stunted at 95% CI (1.31, 10.57). Family size associated with stunting. Under five children whose family member greater than four were 2.73 higher to be stunted at 95% CI (1.15, 6.50) compared with less than four family members. Older children aged 48-59 months had high risk to be stunted with AOR 5.15, 95% CI (1.89, 14.02) and whereas 25-47 months of age children also had higher risks to be stunted with AOR 2.99, 95% CI (1.19, 7.51) compare to younger age. Stunting was also higher in the children who had diarrhoea in last two week with AOR 7.71, 95% CI (3.75, 15.82) who had no diarrhoea.
|
4. Discussions
- This study showed that magnitude of stunting among Under-five age children in Alamura kebele Tula sub city of Hawassa city was 29.7% with 95% CI (24.6%, 34.8%). This finding is consistent with recent report from Shamina Garmama, Doyo Chale and Tankaka Umbullo kebeles at Hawassa Zuria district which was 26.60% [14]. The Ethiopian Demography and Health survey of 2016 also reported relatively the same prevalence in the urban areas of the country (25.4%). However, the prevalence of stunting in the study was higher than study conducted in Gambella (23.5%) and Addis Ababa (14.6%) [8]. This difference might be due to population migration in the study area from rural to urban in order to get better job and living condition, decreased purchasing power of the community, increment of food prices. Again differences in infant and young child feeding practices and child health care could also results in higher prevalence.On the other hand, the study report was lowest of the previous reports in stunting among under- five children in Hawassa Zuria district of Sidama zone was 45.8% [17] southern Ethiopia 38.6% and national average 38% children under 5 are considered short for their age or stunted [8]. This discrepancy might be due to socio-economic difference. Sex of the children had no statically significant association with stunting in this study. Similar findings were obtained at Mwanza district of Tanzania and EDHS 2016 report of Ethiopia. However, study conducted in Hawassa Zuria district in Ethiopia revealed that being male contributed for increased odds of stunting [8,16,18]. The age of child was one of the predictors of stunting in this study. As the age of child increases, the prevalence of stunting also increased. In the study area this trend was seen. Children within age group 24-47 months and 48-59 months were more likely to be stunted. The finding was in agreement with the studies in Egypt [19] and the Ethiopian demographic and health survey [9]. This might be due to stunting in children age 24 months and above were resulted from poor nutritional status of mother’s at pregnancy, inappropriate infant and young child feeding practices and other related factors which were needed to be undergone beginning form conception, through a mother’s pregnancy and up until the age of two which was the most critical period in a child’s development after child reaches above 24 months of age stunting was irreversible. Children who were born with parents who lack farm land ownership had also statistically significant association to child stunting. The finding was in agreement with the studies report conducted by bulletin of the World Health Organization 2006 on the links between agriculture and health an intersectoral opportunity to improve the health and livelihoods of the poor. This might be due to agriculture and health is linked in many ways. However agriculture is essential for good health and it produces food, fibre and materials for shelter; in many countries it is also an important source of livelihood among the poor. At the same time, agriculture can be linked with poor health, including malnutrition, malaria, and food borne illnesses, livestock-related diseases, chronic diseases and occupational ill-health.Regard to health status of a child who had diarrhoea in last two week had high risk to stunt/ short to their age when compare with who had no diarrhoea. The finding was in agreed with the studies conducted in Hawassa Zuria district, southern Ethiopia [20,16]. This may be due to health and physical consequences of prolonged states of malnourishment among children are: delay in their physical growth and motor development; lower intellectual quotient (IQ), greater behavioural problems and deficient social skills; susceptible to contracting diseases.Mothers’ educational level and occupation also did not show a significant association with stunting. Whose mothers had no education were more likely to be stunted as compared to mother with educational status of above secondary. This finding was consistent to the study conducted in India [21], Tanzania [18], and Nairobi Kenya [23] and also in Ethiopia [14,25,24]. However educational status of father also had no statically significant association with stunting. This might be due to mother who had no education had shortage of knowledge which related to better child feeding and caring, low income and low living conditions. This study shows that poorest wealth index or children from household with low wealth index were more likely to be stunted than children from high wealth index or wealthiest households. This result consistent with the study conducted in India [21], Tanzania [18], and Nairobi Kenya [23] and also in Ethiopia [14,25,24]. This might be children from low income households had low access to adequate dietary intake in kinds and the amounts and also it may be due to increment of food prices, decreased purchasing power of the family and also shortage of other important materials and utilities.
5. Conclusions
- In general prevalence of stunting was found to be 29.7%. Maternal education and occupation, family size, land ownership and age of the child were the associated socio demographic factors with stunting. An odd of being stunted among the children was 3.72 times higher whose mothers had no formal education. Under five children who were from housewife mothers were 9 times higher odds of being stunted compared with other type of occupation (Merchant and other type of occupation). Childs age was another predictor of stunting. Under-five children who were older age (48-59 month) had higher likelihood to be stunted with AOR 5.15, 95% CI (1.89, 14.02). Diarrheal episode in the last 2 weeks was associated with stunting. Under five children who had diarrhoea in last two weeks were 7.71 times higher odds of stunting compared with children who had no diarrhoea. Hence this study suggests planning nutrition interventions to effectively address the aforementioned demographic factors with participation of stakeholders and community at large. Additionally, further studies to determine non demographic predictors of stunting are recommended for further stunting prevalence reduction measures at the study area.
ACKNOWLEDGEMENTS
- We greatly acknowledge the data collectors and respondents participated in the present study. We are also grateful for the School of Nutrition, Food Science and Technology, Hawassa University for supports given during the data collection processes. We are happy to thank NORAD project Hawassa University for funding this study.