-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2019; 9(4): 87-98
doi:10.5923/j.phr.20190904.03

Unintended Pregnancy and Childbearing among out-of-school Unmarried Young Women Living in Metropolitan City Slums, South-West Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdebowale A. S. 1, Tinuoya A. F. 1, Olowolafe T. A. 1, Gbadebo B. M. 1, Onwusaka O. C. 2
1Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria
2Department of Public Health, Faculty of Allied Medical Sciences, University of Calabar, Calabar, Nigeria
Correspondence to: Olowolafe T. A. , Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: High rate of unintended pregnancy (UPr) and childbearing among young women have always been reported in Nigeria. This study assessed the level of UPr and childbearing among unmarried out-of-school young women living in urban slums in Kosofe Local Government Area, Lagos metropolis, South-West, Nigeria. Method: A cross-sectional community-based study was conducted using a multi-stage sampling technique to select 372 unmarried out-of-school young women (10-24 years). Qualitative and quantitative methods were used for data collection. Data were analyzed using Atlas Ti and logistic regression model (α=0.05). Results: Mean age and mean age at first sexual intercourse of the women was 18.9±2.8 years, and 16.9±2.1 years respectively. About 32.1% have had at least a child, 29% reported ever had an UPr, 13.3% had induced abortion, 2.9% had ever had miscarriage, and 13% are currently pregnant. Visit to health facility, age, knowledge of ovulation, and who the respondent lives with were significantly associated with UPr and childbearing. Age and visit to health facility were the identified predictors of UPr and childbearing. Non-use of contraceptives, lack of parental care, pre-marital sex, covetousness, and peer pressure were mentioned as the common reasons for unintended pregnancy. Participants expressed their interest to delay childbearing. Conclusion: High incidence of unintended pregnancy and childbearing was reported in this study. Framework on female education and youth friendly fertility control services should be strengthened in the study area.
Keywords: Female youths, Unintended Pregnancy, Fertility, Urban slum, Lagos State
Cite this paper: Adebowale A. S. , Tinuoya A. F. , Olowolafe T. A. , Gbadebo B. M. , Onwusaka O. C. , Unintended Pregnancy and Childbearing among out-of-school Unmarried Young Women Living in Metropolitan City Slums, South-West Nigeria, Public Health Research, Vol. 9 No. 4, 2019, pp. 87-98. doi: 10.5923/j.phr.20190904.03.
Article Outline
1. Introduction
- Unintended pregnancies are pregnancies reported to have been either unwanted or mistimed [1]. Although, not all unintended pregnancies lead to unintended childbearing but it constitutes a large proportion of births among out-of-school unmarried young girls. Unintended pregnancy and childbearing are two fertility related demographic problems because of their implications on fertility itself, population growth and maternal and child health [1-3]. While some advanced nations have social supports for young single mothers, the effects and consequences of unintended pregnancy and childbearing are more pronounced among their counterparts living in less developed countries like Nigeria where no such supports exist. Globally, unintended pregnancy constitutes 40% of all pregnancies and the trend shows a downward trend [4]. The level of unintended pregnancy is higher among the low income countries than the developed countries [4] and its prevalence among young women in sub-Saharan Africa is lower than the estimate for Nigeria [4,5]. Despite the variation in the level of unintended pregnancy by region, place of residence, and other socio-economic factors in Nigeria, there is likelihood that higher rate will be observed in the urban slums than main urban or even in the rural areas. In this study, youth period consists of adolescent (10-19 years) and young adults (20-24 years). This period is characterized by several sexually related health problems [6]. Youth period are marked by quick physical, cognitive, and social changes that create a platform for lifetime capacities and ambitions [7,8]. Moreover, the period is marked with mind development that primarily alters young persons’ thought and how they engage the world realities [7-9]. During youth, social relationships often expand beyond the family unit and youth begin to acquire behaviors from their environment that could have reflective influence on the later part of their life. Many health risk behaviors like smoking, alcohol intake, multiple sexual partners, drug abuse and others that often translate to health challenge in the later part of life begin during the youth period [10-12]. Thus, early sexual initiation for a girl child specifically if it results in unintended pregnancy and childbearing can negatively affect her socioeconomic and career advancement.The Nigeria population is young and the universal basic education emphasizes free primary education for all, but female enrolment rate is still low [13]. Many young women are out-of-school for reasons related to poverty, cultural factors, pregnancies and childbearing [14,15]. The harsh economic condition in Nigeria affects mostly the poor majority of the household population. Lack of financial capacity to meet school demands can lead to school dropout among children. In such circumstance, the out-of-school women living in urban slums become exposed to risk of unprotected sexual activities and pregnancy. These they encounter in most cases in the course of meeting their daily needs and contributing to the well-being of their families. The study area is known to have large number of school drop-out children being urban slums and cases of unintended pregnancy are common among young women. In few instances, cases of abandoned newborn babies are observed in the study area. This raises the curiosity of the researchers to assess the level of unintended pregnancy and childbearing in the area. The poor economic conditions in most Nigeria households and lack of adequate sexual and reproductive health programs in Nigeria bring unintended pregnancy and childbearing among unmarried youths into sharp focus. Although there is a growing body of literature on the factors influencing young women’s health, [16,17] but less is known about the risk and protective factors of unintended pregnancy and childbearing among young women living in urban slums in Nigeria. Such is the focus of the present study and its outcome is expected to fill the gaps in research on young women’s reproductive health in Kosofe LGA, Lagos State.
2. Literature Review
- Unintended pregnancy and childbearing among young women are social and health problems that have generated much attention of researchers in the contemporary times and the issues are widely debated in the literature because of the evolving and changing cultural norms in different parts of the world. The setting where young women live have implication on their pregnancy risks [18]. Human development mainly begins at the family level. Barber et al [19] identified three core parental behaviors: connection, encouraging autonomy and behavioral regulation and these are learnt by children on daily basis. A caring and committed guardian/parent can shape the life of individuals who grow up in a bad setting from its associated consequences. Contrariwise, young women who grow up in homes with good education and strong financial capabilities can be disrupted by peer pressure or community effects. The protective effect of the positive family relationship, parental connectedness and involvement on youth regarding early sexual initiation and pregnancy have been widely established in literature [18,20,21]. Additionally, the tight relationship that exists in some rural settings may allow parents to depend on neighbors to watch out for their young women but this neighborhood effect may disappear in cities. Therefore, young girls with low levels of parental/guardian monitoring and community supervision are at a particularly greater risk of early sexual debut if they live in the city slums. The risks associated with unintended pregnancy are amplified if they occur among young unmarried women [22]. Physiological immaturity which marks young women as not mature enough to safely carry a fetus to term or to bear a baby and lack of adequate health care further increase the risk [22]. In Nigeria, the education policy does not allow pregnant pupils to remain in school and this has truncated formal education of many young women. However, a few ones find their way back to school after baby delivery. Low levels of education as a result of early motherhood may confine young girls to unskilled jobs and low socioeconomic status in life. High maternal mortality ratio of 560 per 100,000 in Nigeria are mainly attributed to pregnancy related complications and abortions among young women [23-25]. An Ethiopian study among pregnant woman attending ANC showed that the prevalence of unintended pregnancy was 27.1% and its associated factors were marital status, parity, and contraceptive awareness [26]. In Nairobi Kenya’s study, the prevalence of unintended pregnancy was found to be lower among women in slum settlements (21%) than those in non-slum settlements (27%) and age, marital status and type of settlement were identified as determinants of unintended pregnancy [27]. Being in age group 15-19 years and unmarried showed higher risk for unintended pregnancy than older women and ever-married women respectively [27]. In a study conducted in Nigeria which used a national survey data to understand issues that are related to teenage fertility and pregnancy among young women, age and marital status were found as important predictors of pregnant or having at least a child [28]. In Ajala’s study, an increased age was found to be associated with higher odds of being pregnant and childbearing among young women and the author recommends that teenage pregnancy and childbearing are severe policy mediation area in order to check the current trend in population growth rate in Nigeria [28].In South-West Nigeria, a study conducted to determine the prevalence and determinants of unintended pregnancy among women found prevalence of 35.9% while that of induced abortion was 33.5% [29]. A similar study at national level found 28% prevalence of ever had an unwanted pregnancy and about half of this women said they have attempted to terminate the pregnancy mainly because they were; unmarried, too young or in school [30]. The likelihood of adolescent pregnancy was higher among older adolescence than younger ones and the risk was higher in male-headed households and households headed by older individuals (30-44 years) than female and younger individual (15-29 years) headed households respectively [31]. A comparative study of teenage pregnancy in Lagos State University Teaching Hospital obtained 1.01% as incidence of teenage pregnancy and majority of such pregnancy occur at ages 17 to 19 years [32]. A study implemented in Sagamu, a city in south-west Nigeria, the prevalence of teenage pregnancy was 22.9% and higher unwanted pregnancy was reported by teenagers than the older age group. The predictors of teenage pregnancy found were low social class, religion, being a student and employment status [33].With respect to problems associated with early pregnancy, Afrose and colleagues research findings showed that the teen mothers have more obstetric complications mainly due to their underdeveloped pelvis and they have premature and low birth weight babies [18]. In a multi-country survey on maternal newborn’s health by Ganchimeg et al. among young mothers and their infants, it was established that, adolescent mothers had higher risks of; eclampsia, puerperal endometritis, systemic infections, low birthweight, preterm delivery and severe neonatal conditions than mothers aged 20-24 years [34]. A retrospective cohort study of pregnant young women with a live birth during 1995 and 2000 in the United States showed that, all teenage groups were associated with increased risks for pre-term delivery, low birth weight and neonatal mortality and higher risk of lower Apgar score after adjustment for possible confounding factors [35]. In a Nigeria study, pregnancy and delivery complications associated with young women were hypertensive disorders of pregnancy, anemia in pregnancy, cephalopelvic disproportion and caesarean section [32].
3. Method
3.1. Study Area
- The study was carried out in Kosofe Local Government Area (LGA), Lagos State. The Local Government has a population of about 665,393 people [41] and is characterized with several communities, some totally urban while some semi urban and there exists urban slums in the LGA. Kosofe is very densely populated with a balanced mixture of educated elites and uneducated residents. The major occupation includes administrative jobs and petty trading. Fishing, carpentry, tailoring, mats weaving, mechanics and technicians, and also self-owned businesses are also source of income to the people in the LGA. The people in the LGA are predominantly of Yoruba origin but other tribes are present in large number in the LGA. There are quite a number of young women who are out of school in the LGA. The population structure reflects Nigeria pattern. Even though, primary and secondary schools are found in every nook and cranny of the LGA, women who have dropped out of school who migrated from other parts of Nigeria are seen in large numbers in the LGA.
3.2. Study Design and Study Population
- The sample design used was community-based cross sectional survey. The study population was out-of-school young unmarried sexually active females from ages 10 to 24 years (n=372). Out-of-school in the context of this study is defined as any person who has no formal education or has not completed her secondary education but has dropped out of school. The studied women are those who are usual resident in the study area and must have lived in the LGA for at least a period of 5 years. However, women who were sick and those who were younger than 18 years but could not provide either a guardian or parent to grant approval for the interview were excluded from the study.
3.3. Variable Description
- The dependent variables were; ever experienced unintended pregnancy (no=0 or yes=1) and ever had at least a child (no=0 or yes=1). The variables that were examined included; age, education, religion, residence, contraceptive use, number of children, recent sexual activity, currently pregnant, miscarriage, abortion, birth, sexual communication, sexual reproductive and health knowledge, alcohol consumption, ethnicity, number of sexual partners.
3.4. Data Collection Method
- The study used a method mix approach. Interviewer administered questionnaire was used to address the quantitative arm of the study and four focus group discussions (FGDs) were carried out for the qualitative arm. A semi-structured interviewer administered questionnaire was used to obtain information from the eligible respondents. Some of the questions contained in this instrument were adapted from the questionnaire used for the 2013 Nigeria Demographic Health and Survey. The draft questionnaire was pre-tested at a different Local Government Area (LGA) in Lagos State by trained research assistants. Thereafter, internal consistency and reliability tests were carried out (Cronbach alpha = 77%, non-response rate = 8%. The questionnaire was revised after the pre-test. The revised questionnaire was used for the actual survey exercise.The study participants were selected using a multi-stage sampling approach. At the first stage, 4 political wards were randomly selected from the priority wards in the community. The priority wards are the wards in the part of the LGA which have slums domicile in them (Ikosi Isheri, Agboyi, Ajegunle and Odo ogun). In each of the selected wards, sampling frame of out-of-school young unmarried women was constructed through household enumeration and subjects were systematically selected from the list. However, in a household, where there are more than one eligible respondents, balloting was used to pick the person who will participate in the study.For the qualitative arm of this study, four FGDs were carried out in each of the four priority selected political wards within Kosofe LGA. These wards were those used for the quantitative arm of the study. Eight participants were recruited into each group and the interview lasted for at least 45 minutes. Comprehensive discussion was held with the groups based on questions on issues in the areas of unintended pregnancy and child bearing. The participants in the FGD were out of school young unmarried women within the ages 10 to 24 years. They were divided into two categories based on their level of education, those who had no formal education constituted the first category while those who have at least primary education were in the second category. We also ensured that each participant in the FGD must be (i) sexually active (ii) have experienced unintended pregnancy or child birth prior the survey. Question guide that contains 10 questions on the issues around pregnancy and childbearing was used to interview the respondents. Tape recorder and note taken were used to record responses of participants and later transcribed.
3.5. Data Analyses
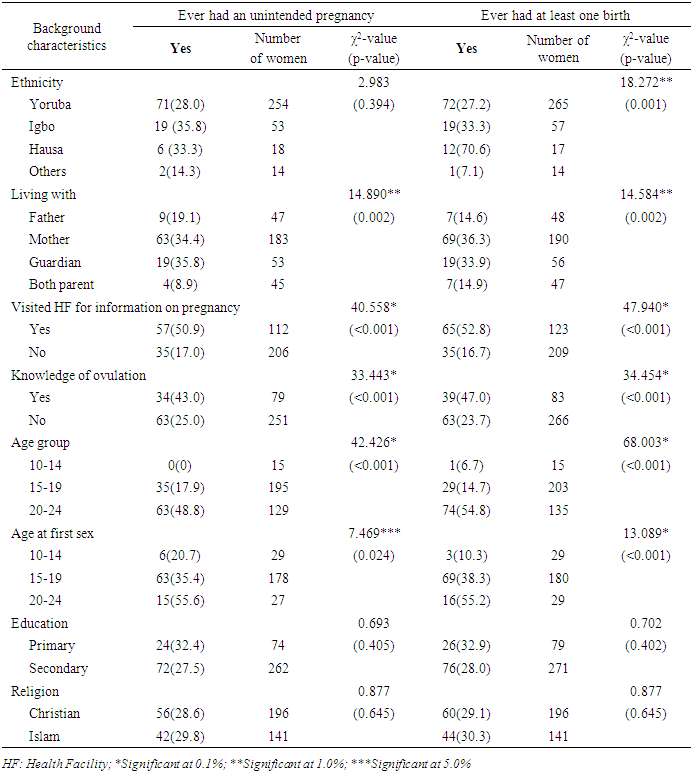
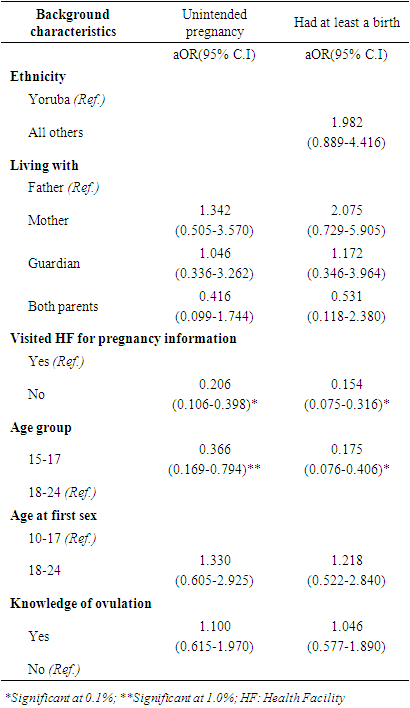
- The quantitative data were analysed using descriptive statistics, Chi-square and logistic regression models (α=0.05). The Chi-square was used to examine the association between unintended pregnancy and socio-demographic characteristics of the women. The same analysis was conducted for ever had at least a child, a measure of fertility experience of the women. The dependent variables were dichotomous and as such, logistic regression was used to identify the predictors of unintended pregnancy and childbearing among the subjects. SPSS version 21 software was used for the analysis. The collected qualitative data were analyzed in a systematic, sequential, and continuous manner using open coding method. The themes emerged mainly from the research questions and from the narratives of research participants. Data analysis involved: data examination which was achieved by listening to tapes, reading the observational notes taken during interview and summary notes written immediately after the interview severally; identification of the themes by writing memos in the margin of the text in the form of short phrases, ideas or concepts arising from the texts and beginning to develop categories; indexing which comprises sifting the data, highlighting and sorting out quotes and making comparisons both within and between cases; charting, we lifted the quotes from their original context and re-arranged them under the newly-developed appropriate thematic content in order to reduce the data. In order to arrange, reassemble, and manage the theme in a systematic way, we used ATLAS Ti, software.
3.6. Ethical Considerations
- Formal ethical approval was obtained from the health review ethical committee of Lagos University Teaching Hospital, Lagos before the commencement of the study. Advocacy visits were made to the study areas where discussions were held on the objectives and significance of the study with the community head and opinion leaders. During the data collection exercise, informed consent was obtained from the participants. For the participants who were younger than 18 years (classified as ‘child’ by Nigeria Human right law, an informed consent was obtained from their parents or guardians who must be at least 18 years at the time of the implementation of this study. The anonymity and confidentiality of the information they provided were assured. Where the researchers felt intervention might be needed, the participant’s approval was sought.
4. Results
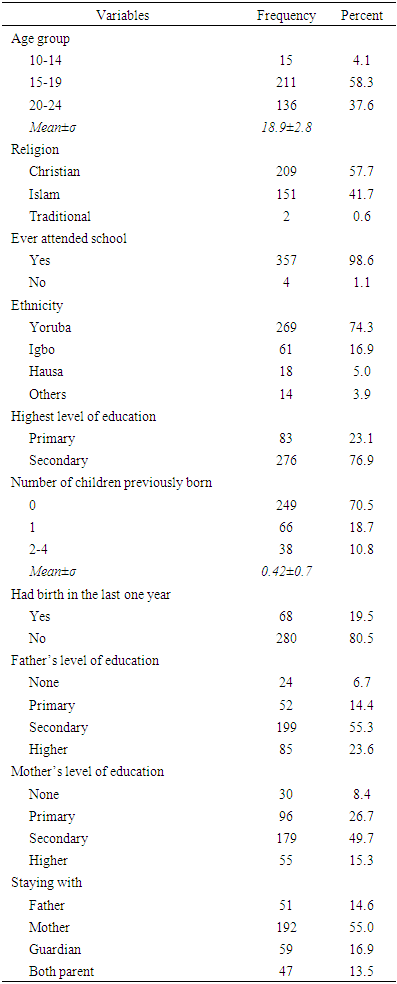
- Table 1 shows that more than half (58.3%) of the respondents falls within the age group 15 to 19 years, while only 4.1% were 10-14 years. The predominant religion was Christianity 57.7%, followed while Islam was 41.7%. All the respondents who reported information about their level of education had at least primary education. Yoruba ethnic group constituted 74.3% of the respondents. The majority of the respondents said they have no children (70.5%), while 10.8% said they have at least 2 children. Regarding the respondents’ level of education of their parents: the majority said that their father and mother had secondary as the highest level of education; while 6.7% of the fathers and 8.4% of the mother have no education respectively. About 55.0% of the respondents stay with their mothers, 13.5% stay with both parents, 13.3% were living with both parents and 16.9% reside with guardian.
|
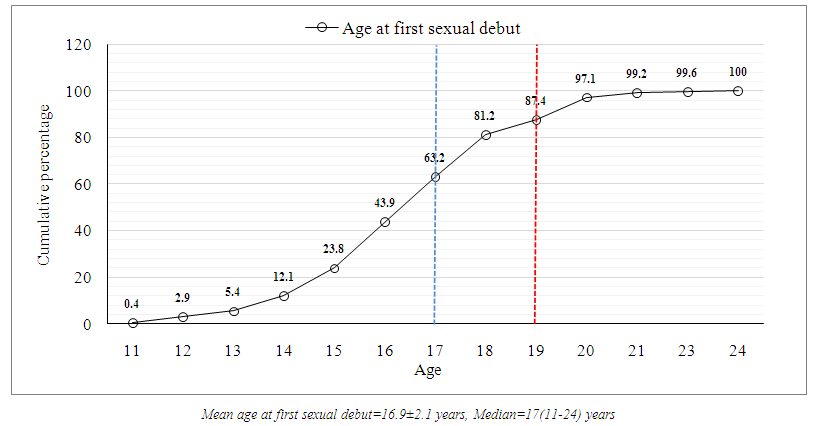 | Figure 1. Cumulative frequency distribution of age at first sexual debut |
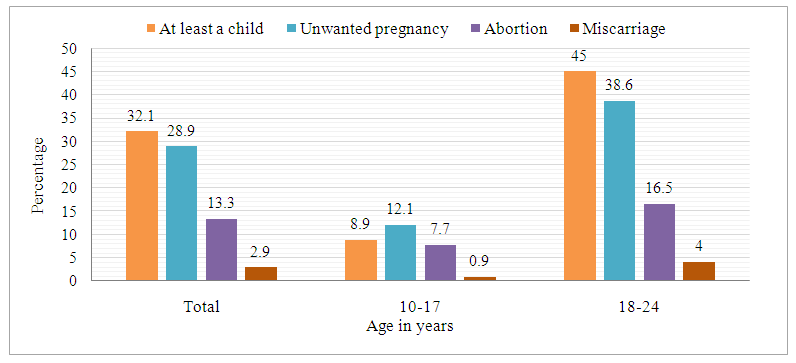 | Figure 2. Percentage distribution of the respondents by type of pregnancy problem ever had according to age of the women |
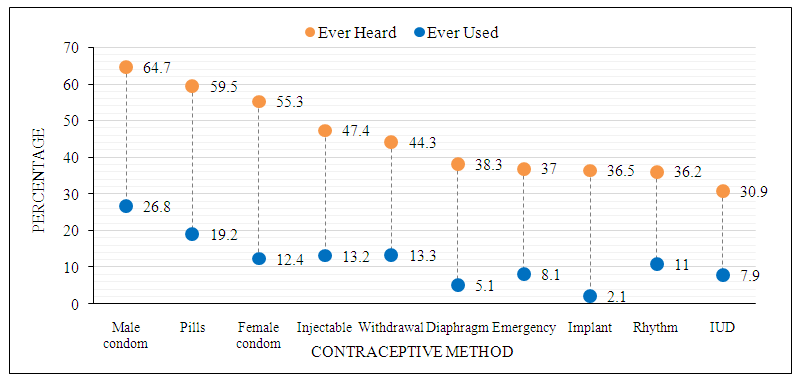 | Figure 3. Percentage distribution of the respondents by type of contraceptive method ever heard and ever used |
|
|
5. Discussion
- The mean age at first sexual intercourse was 16.9±2.1 years. The observed mean age at first sexual intercourse in this study is similar to 17.6 years obtained among young women from a national survey previously conducted in Nigeria [42] and totally in agreement with the figure reported in a similar study conducted in Nigeria [43]. However, while our study focused on out-of-school young women, the national survey focused on all women of reproductive age and this may account for slight disparity in the reported figures. Adolescent and youth periods are characterized with some sexual risk behaviors that make women susceptible to pregnancy [7,42,44,45]. Regrettably, in most cases, young women are raped, forced to have sex, consensual sex and the end result is unwanted pregnancy. Conscious of the severe punishment and shame awaiting her, some of the victims do not report such pregnancies to their parents or guidance while some others don’t even know that they are pregnant at the first instance. Nigeria law does not permit abortion except if it is done to safe the live of the woman. In this context, young pregnant women and their male sexual partners habitually result to self-medication through patent medicine store’s attendants and illegal abortion. This situation has led to untimely death of many young women in Nigeria. Some of the highlighted issues above were reported during the focus group discussion in this study. We also found that about one-third of the women who participated in this study had experienced unintended pregnancy. The high prevalence observed can be explained by the selection criteria used (unmarried, out-of-school, living in urban slum and young women) in this study. A study conducted in Kenya and Ethiopia substantiates our finding [26,27]. In Nigeria, childbearing only receives societal blessing if it is practiced within marriage. In the South-West part of Nigeria where this study was conducted, adolescent childbearing particularly if it occurs out-of-wedlock is not acceptable. Often, the parents, guardian and the entire community of the victim will stigmatize against them and in most situations they are neglected [18]. The health and social implications of childbearing and rearing among young women are enormous and these challenges are aggravated if such birth occurs out of marriage [23,25]. In this study, about one-third had had at least a live birth prior the survey. The context specific nature of our study could be attributed to this high observed birth rate among the women. Nigeria education policy does not support pregnant pupils to remain in school during pregnancy. It is also likely that some of the women dropped out of school because of pregnancy as found in the qualitative arm of this study. The identified predictors of unintended pregnancy and childbearing were age and visit to health facility for pregnancy information. Being in the younger age group was found to be protective of unintended pregnancy and childbearing. This direction of relationship is expected due to the longer years of exposure to the risk of pregnancy by women in older age group (18-24 years) than those in the younger age group (15-19 years). In addition, any individual younger than 18 years is considered as a child according to Nigeria Child’s Right act so the risk of high coital frequency is lower among women in the age category than those who are above 18 years or older. The pattern found in our study regarding age, unintended pregnancy and childbearing has been reported in earlier studies in Nigeria and other parts of Africa [18,26,28]. It is rather surprising that those who has visited health facility for pregnancy information experienced higher unintended pregnancy than their counterparts who did not. Since the timing of health facility visit was not captured in the study’s questionnaire, it is cumbersome to speculate which comes first ‘unintended pregnancy or health facility visit’. Therefore, it is possible that some of the young women who already had unintended pregnancy visited health facility for care about the pregnancy (antenatal services) and this may account for our finding. In the qualitative part of this study, women who already experienced unintended pregnancy believed that the reasons for its occurrence was mainly because they did not use any pregnancy prevention method. Other reasons mentioned are failure on the part of their parents to meet their daily needs, living with non-biological parents, the living environment and peer pressure. These reasons have been consistently reported in literature [20,46,47]. Aside modern contraception, some of the common ways of preventing unwanted pregnancy highlighted by the women because of their simplicity and easy access were; mixing lime with bicodin, salt and water, 7up drink and salt, 7up drink and alabukun (a malaria drug). The women also expressed their feelings during their first pregnancy experience, some of them however thought they only had fever and flu at that time and were seriously sad when it was revealed to them that they were pregnant. In their opinion, they said they might terminate their future pregnancy if their partner rejects it outright or pregnant during breastfeeding to avoid shame or if gang raped or rejected by their family. It is interesting to know that some of the participants expressed intention to delay childbearing until they are financially buoyant. LimitationDue to the sensitive nature of this study, there is the likelihood of report bias by women who claimed that they had never experienced unintended pregnancy or childbearing. Also, there is possibility that the number of women who are currently pregnant or had experienced pregnancy termination will be a little higher than what was reported in this study. Having conscious of these limitations, the researchers ensured that they were minimized by probing to ascertain the authenticity of the information the respondents provided during the interview.Policy implication of the study The high prevalence of unwanted pregnancy and childbearing found in this study call for the need for policy on family-planning counselling, information, education, communication and services, including access to safe and effective contraceptive methods in the study area. Such policy should also include prevention of unsafe abortion, management of the abortion consequences and appropriate counselling on human sexuality and reproductive health. Community assessment of unintended pregnancy among young sexually active women as implied by this study will facilitate improvement in understanding of the future fertility situation and the level of unmet need for contraception and family planning in the study area.
6. Conclusions
- Unintended pregnancy, abortion and fertility rate were high among unmarried young women living in slums in Kosofe Local Government area, Lagos State. These indices were found to be more prevalent among women aged 20-24 years, those with primary education, Muslims and those living in the main urban in the study area. The prevention practices often used by out-of-school young women in the study area were majorly not modern contraceptive methods and poverty was identified as the main reason for having unwanted pregnancy and early childbearing. In order to reduce unintended pregnancy and its associated consequences in the study area, sexual and reproductive health enlightenment campaigns should be strengthened. Free access to modern contraceptive by youths in Kosofe LGA, Lagos State can bring about a quick reduction in premarital pregnancy in the study area.