-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2019; 9(4): 77-86
doi:10.5923/j.phr.20190904.02

Socioeconomic, Demographic and Disease-Related Determinants of Quality of Life among Thalassemia Patients in Gaza Strip - Palestine
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAshraf Eljedi
Faculty of Nursing, Islamic University of Gaza, Gaza Strip, Palestine
Correspondence to: Ashraf Eljedi, Faculty of Nursing, Islamic University of Gaza, Gaza Strip, Palestine.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Thalassemia is the most common hemoglobin disorder in the world and thalassemia major and intermedia stand among the most severe forms. Quality of Life (QOL) and its determinants has emerged as an important parameter for assessing the quality of health care of patients with thalassemia disease. The QOL of thalassemia patients in the Gaza Strip has not previously been studied. This study aimed to determine the socio-demographic and disease-related determinants of QOL among patients with thalassemia disease in Gaza Strip, using the Short Form-36 (SF-36) questionnaire. Descriptive, analytical, cross-sectional study has been performed on 200 eligible thalassemia patients at two hematology centers in Gaza in 2014. After collecting the participants’ socioeconomics, demographics and disease characteristics, they filled out the SF-36 questionnaire. T-test and ANOVA were used to determine the relationship between various variables and the QOL score. The results showed that study participants had a medium perception level of QOL (mean score was 41.98, SD=19.24). The overall mean percentage for SF-36 domains scores ranged from 24.68% to 53.85%. The general health domain got the highest score (53.85%) while the lowest domain was physical role limitation (24.68%). Finding showed that males had poorer QOL than female (40.93% compared with 43.02%). QOL was better at the older age (26-85 years) participants (45.66%), compared with the younger age (18-25 years) participants (40.80%). In addition, married participants (47.51%) had better QOL compared with unmarried (41.45%). Moreover, employed participants with high income had better QOL (44.23%) than those with low income (40.94%). In addition, findings showed that, patient with university educational level had significantly better scores than those with secondary educational level or less (p=0.046). For disease related variables, finding showed patients with thalassemia major (41.62%) had poorer QOL than patients with thalassemia intermedia (45.03%). The association between the previous variables did not reach significant level. Finally, comorbidities did not have any significant effect on QOL scores. The findings concluded that male, younger age, unmarried, low income, unemployment, low education and thalassemia major were the most prominent determinants of lower QOL among thalassemia patients. Psychosocial, social and financial support may help patients to cope better with their chronic disease. Designing and implementing educational programs for nurses and physicians who work in hematology units would reduce the negative impact of thalassemia on the patients' QOL.
Keywords: Quality of life, Thalassemia, Socioeconomic, Demographic, Disease-Related, Determinants
Cite this paper: Ashraf Eljedi, Socioeconomic, Demographic and Disease-Related Determinants of Quality of Life among Thalassemia Patients in Gaza Strip - Palestine, Public Health Research, Vol. 9 No. 4, 2019, pp. 77-86. doi: 10.5923/j.phr.20190904.02.
Article Outline
1. Introduction
- Thalassemia - as the most common hereditary disorder over the world - is regarded as a serious problem in public health issues in the Mediterranean area [1]. Thalassemia refers to a heterogeneous group of inherited disorders of hemoglobin synthesis characterized by a disturbance of globin chains’ production, leading to anemia, ineffective erythropoiesis and destruction of erythroblast in the bone marrow and blood cells in the peripheral blood [2].It is a life-limiting and potentially life-threatening condition that causes substantial disruption in education and social activities. Patients and their families are conscious of the disabling nature of the condition and chronic therapy is a constant reminder that they are “different”, making it practically impossible to lead a normal life. Generally, the psychosocial burden affects many aspects of the patient’s life, such as education, free-time, physical activities, skills, capabilities and family adjustment, the effects of which, often result in anxiety, isolation and depression and poor quality of life (QOL).QOL is defined as perception of individuals of life, values, goals, standards, and interests in the context of culture. There are a number of factors related to the diseases and related to the social context that can affect QOL. Ages, gender, level of education, the amount of symptoms and distress experienced by individuals with thalassemia have been related to QOL [3].In Gaza Strip (GS) - Palestine, thalassemia is considered an exhausting, lifelong-suffering disease from two aspects; the chronic nature of the disease itself in terms of frequent hospital visits, drug unavailability, side effects of drugs, disease complications and socioeconomic hardships in GS, and implications of the disease on the quality of life of patient regarding the physical, psychological, emotional, and social aspects.Unfortunately, factors influencing QOL of thalassemia patients in GS are not well known. The researcher tries to bridge this gap through exploring the socio-demographic and disease-related determinants of quality of life among thalassemia patients in Gaza strip for the first time in Palestine generally and in GS specifically.
2. Methodology
2.1. Design
- Descriptive analytical cross sectional study has been conducted at the only two main centers providing care for hematology patients. The first center is located at Al-Shifa Hospital in Gaza city while the second center is located at European Gaza Hospital (EGH) in Rafah city. The time allocated for data collection was from 01 August 2014 to 31 October 2014.
2.2. Sample
- The study sample included 200 patients with thalassemia; of them, 137 patients were treated at Al-Shifa Hospital and 68 patients were treated at EGH.
2.3. Inclusion and Exclusion Criteria
- Eligible participants were aged 18 years or older, suffered from beta thalassemia major or beta thalassemia intermedia, agreed to give consent and were able to respond to the questionnaire. Any patient who did not meet the inclusion criteria or were seriously ill were excluded from the study.
2.4. Study Instrument for Assessment of QOL
- The Short-form Health Survey (SF-36) item has been used in this study to assess QOL. The SF-36 survey is a well-recognized, self-administered QOL scoring system. It consists of eight independent scales and two major dimensions. The eight multi-item scales include physical functioning, physical roles, bodily pain, general health, vitality, social functioning, emotional roles and mental health. The first four scales are summarized into the physical health dimension and the last four scales into the mental health dimension [4,5]. It also includes a single item that provides an indication of perceived change in health.SF-36 survey is widely used in many countries and has been translated into many languages and proved to be valid and reliable. The Arabic version is being used in Arabic speaking countries where certain items were modified in order to fit more closely into the Arabic context, and consist with the inherent norms of Arabic societies, which share almost the same socio-cultural norms [6,7].The SF-36 was scored according to the recommendation by McHorney [4]. The SF-36 items describing the eight health concepts were transformed into a score of 0-100 and the items scale averaged to obtain a subscale score. Physical component summary and mental component summary were computed by averaging the values of the respective subscales. A higher score indicated higher levels of function and better health.
2.5. Ethical and Administrative Approvals
- The ethical approval from Helsinki Committee in Gaza and an administrative approval from the Ministry of Health were taken to conduct the study.Before initiation of the data collection a brief introduction on the aim and objectives of the study was presented to the patients. They were informed about their full right to participate or refuse to participate in the study. Moreover the researcher assured the respondents that there would be no invasive procedure included in the study and all the findings of the study would be used to guide the service providers and policy makers to improve QOL for thalassemia patients. A complete assurance was given to participants that all information provided would be kept confidential and their names or anything which could identify them would not be published or exposed anywhere. Their participation and contribution would be acknowledged with due respect. The researcher explained the purpose of the questionnaire to the patients before obtaining consent. Moreover participants were informed that the study results will be used for scientific purposes and no personal data would be revealed. Questionnaires were only distributed to those who had consented to participate in the study.
2.6. Pilot Testing
- Data collection instruments (demographic sheet and the SF-36 item health questionnaire) were tested by 20 participants. The goals of the pilot study were to assess the adequacy of the data collection plan, to explore whether respondents understand the questions in the same way, to minimize the problems which may rise during data collection, to identify all domains and components of instruments, and to estimate the interview duration. The pilot participants were included in the study. Results from the pilot study pointed out that the questionnaire would provide the needed data to meet the purpose of the study.
2.7. Data Collection
- Data were collected through face-to-face SF-36 questionnaire interview and from patients' files. At the start, all questionnaire forms were prepared, organized, and classified with serial numbers to ensure the availability of the needed information.The patients were contacted personally and informed about the aims of the study and that the participation was voluntary. The researcher gave the patients enough time to answer the questions and encouraged them to be open and virtuous, while assuring them that information given in the interview would remain confidential and just used for the purpose of the study. During the interview any vague information were simplified by the researcher to ensure exact and real answer by the responder.
2.8. Response Rate
- According to the eligibility criteria, the researcher selected 200 patients whose age was more than 18 years to participate in the study. A total number of 161 patients agreed, which represented (80.5%) of the study population while 39 patients refused, which represented (19.5%) of the population.
2.9. Statistical Analysis
- Statistical analysis had been done using the Statistical Package for Social Sciences Software (SPSS) version 20.0. The results were expressed as mean values ± standard deviations and proportions, as appropriate. We conducted univariate analysis to determine the correlations between clinical and demographic factors and the QOL score. The independent samples t-test was used to compare scores between pairs of subgroups of patients in relation to each of the variables of gender, age, type of thalassemia and comorbidity. The analysis of variance (ANOVA) test was used to make comparisons between the scores in different categories of patients in relation to educational level and economic class. Two-tailed p-values less than 0.05 were considered statistically significant.
3. Results and Discussion
3.1. Socioeconomic and Demographic Variables
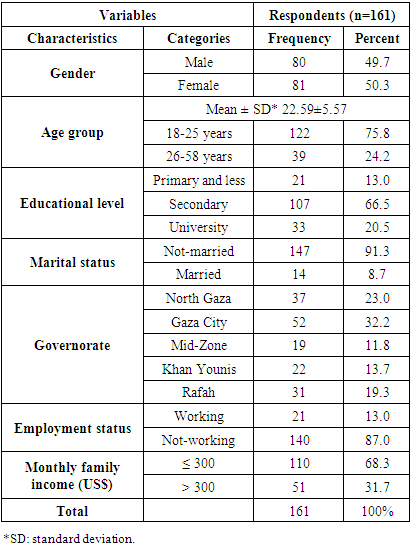
- Of the 200 eligible patients with thalassemia, 161 (80.5%) participated in the study and completed SF-36 questionnaire by interview. Table (1) showed that 81 (50.3%) were females and 80 (49.7%) were males. The average age of participants was 22.59 (range: 18–58 years, SD=5.57). The highest percentage was aged 18-25 years which represented (75.8%) while the lowest was aged more than 26 years which represented (24.2%). Level of education of 66.5% was secondary school whereas (31.0%) had higher education. Concerning the marital status, 91.3% were unmarried while only 8.7% were married patients. About 140 (87.0%) were unemployed while 21 (13.0%) of them were employed. Most of the participants had an income of less 300 US$ (n=110; 68.3%) while 31.7% had an income of more than 300 US$.
|
3.2. Disease Related Variables
3.2.1. Thalassemia Type
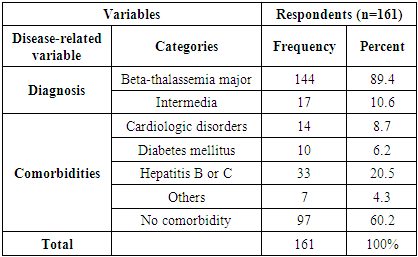
- Of the 161 participants in the study, 144 (89.4%) were diagnosed as thalassemia major while 17 (10.6%) diagnosed as intermedia (Table 2).
|
3.2.2. Comorbidities
- Concerning history of chronic disease, the study revealed that (39.2%) of participants had a history of chronic diseases; of them, (20.5%) had a history of hepatitis B or C, (8.7%) had a history of cardiologic disorders, (6.2%) diabetes mellitus and (4.3%) had other diseases.
3.3. The Effect of Thalassemia on the QOL Domains
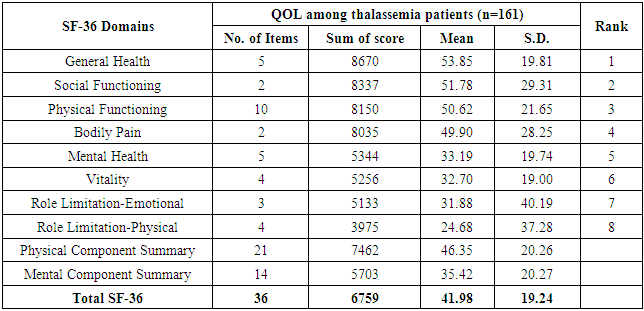
- The Physical Component Summary (PCS) consists from physical function, role limitation due to physical health, bodily pain, and general health. The Mental Component Summary (MCS) consists of vitality, social functioning, role limitation due to emotional problems, and mental health. The researcher considered the median of QOL scores as the referent point. The median was 37.71, so categories were as follows: 25.92 or less (very poor level of QOL); 26.0-37.71 (poor level); 37.8-53.75 (medium level) and 53.76-100 (good level of QOL).Table (3) showed that the mean scores for the SF-36 subscales ranged from 53.85 (SD=19.81) for general health to 24.68 for role limitation due to physical function. Most of the respondents had a medium level (46.35 ± 20.26) of QOL for Physical Component Summary (PCS). The results showed that the lowest domain in PCS was role limitation due to physical function with a mean of 24.68; mean score of bodily pain domain was 49.90; physical function domain was 50.62 (SD=21.65). The results also showed that the general health domain got the highest score (mean=53.85, SD=19.81).
|
3.4. QOL and Socioeconomic Demographic Variables
3.4.1. Differences in QOL According to Gender
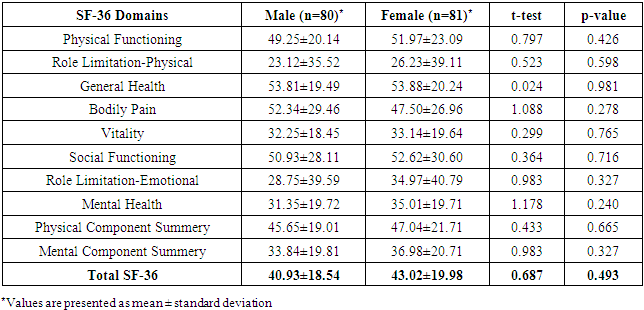
- To differentiate between the scores of QOL of males and females, independent t-test was used (table 4). It showed that, female patients had better QOL than male on seven of the eight subscales (physical functioning, physical role, general health, vitality, mental health, social functioning, and emotional role) and on both summary scales PCS and MCS. However, the differences between overall QOL perception did not reached statistically significant differences (p=0.493). This result is consistent with Safizadeh et al. (2012) who found that female participants had a higher scores in all domains except for bodily pain, when compared to the male participants, such a difference was only significant in physical function and general health domains (p < 0.05) [8]. In addition, results were consistent with Montazeri et al. (2005) who conducted a large population-based study in Iran, and found that women and older age had lower scores on bodily pain domain and role limitation due to emotional problems [9].
|
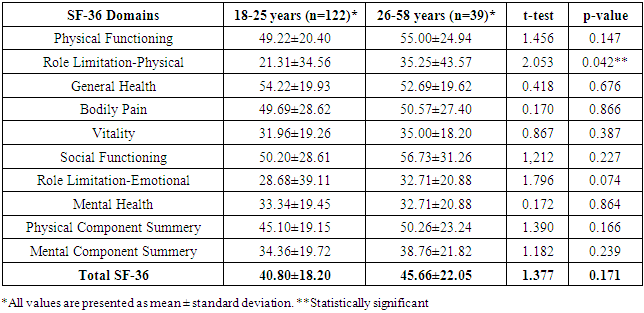
3.4.2. Differences in QOL According to Age
- Table 5 showed that, patients whose age was more than 26 years had better QOL than patients whose age was less than 25 years on seven of the eight subscales (physical functioning, general health, vitality, mental health, social functioning, and emotional role) and on both summary scales PCS and MCS. The differences between the means of the seven QOL domains due to the age group have not reached statistically significant level (p>0.05). Here the researcher noticed that QOL was worse in patients younger than twenty-five years which means that they were incompatible with their disease-related conditions. In addition, disease restricts patients' natural life, which gives them a sense of the weakness in their QOL.
|
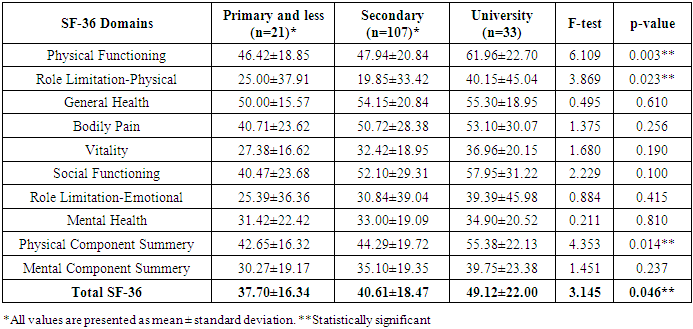
3.4.3. Differences in QOL According to Educational Level
- One-way ANOVA test was used to investigate differences between the scores of QOL domains of thalassemia patients regarding educational level as illustrated in table 6. Finding showed that thalassemia patients at university level had better mean scores in all of QOL domains (physical functioning, physical role, general health, vitality, mental health, social functioning, and emotional role) and on both summary scales PCS and MCS than other educational categories.
|
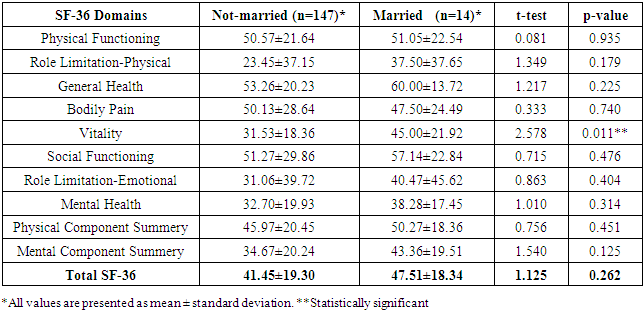
3.4.4. Differences in QOL According to Marital Status
- Table (7) showed that there were no statistically significant differences between overall QOL scores according to marital status (p=0.262), despite the fact that married patients had slightly higher scores in the following domains: physical functioning, physical role, general health, vitality, mental health, social functioning, and emotional role, and on both summary scales PCS and MCS than married patients.
|
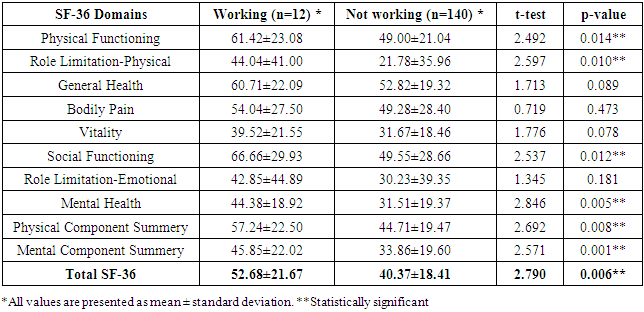
3.4.5. Differences in QOL Scores According to Employment
- Findings show that employed thalassemia patients had statistically significant higher scores in the following QOL domains: physical function, physical role limitation, social function and mental health and on both summary scales PCS and MCS than the unemployed (t=2.49, 2.59, 2.53, 2.84; p=0.014, 0.010, 0.012, 0.005) respectively (table 8).
|
3.5. Disease Related Variables
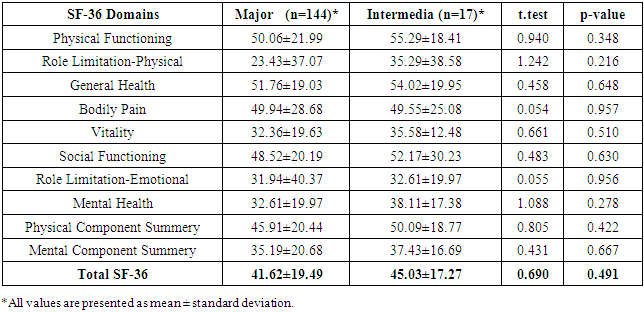
3.5.1. Differences in QOL According to Thalassemia Type
- Table (9) revealed that patients with thalassemia intermedia had better levels of QOL than thalassemia major on the following subscales: physical functioning, physical role, general health, vitality, mental health, social functioning and emotional role, and on both summary scales PCS and MCS. The differences between patients with thalassemia major and thalassemia intermedia were not statistically significant (p>0.05).
|
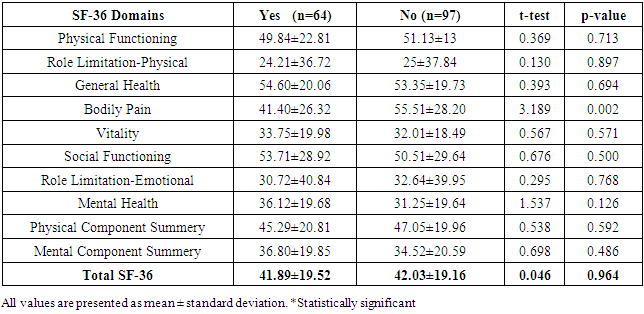
3.5.2. Differences in QOL Scores According to Comorbidities
- Table (10) indicated that thalassemia patients without comorbidities had slightly higher total QOL scores compared with thalassemia patients with comorbidities (cardiologic disorders, diabetes or hepatitis). However, there were no statistically significant differences (p>0.05) between the means of the all of QOL domains and history of chronic disease.
|
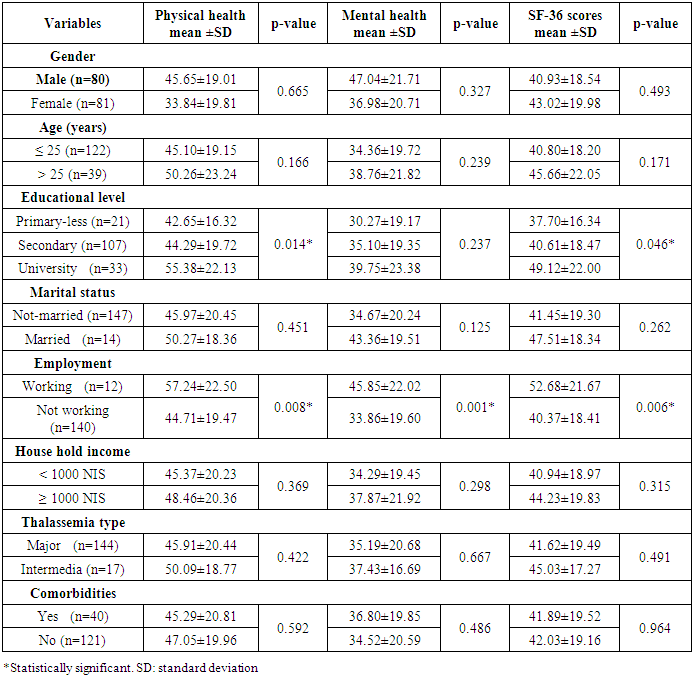
3.6. Univariate Analysis of Clinical and Demographic Factors and QOL Scores
- Table 11 demonstrates the results from the univariate analysis on covariates in relation to the physical health, mental health and total SF-36 scores. There were no statistically significant relationships between the scores and gender, age, marital status, household income, thalassemia type and comorbidities (p>0.05). The patients with higher education level had significantly higher scores for physical health, mental health and total scores, in comparison with patients with primary and secondary levels (p=0.046). Moreover, the patients who work had higher scores than shown by patients who do not work, in all of these three evaluated scores (p<0.001).
|
4. Conclusions
- The overall mean scores of SF-36 domain were at a medium level and ranged from (24.68%) to (53.85%). Significant differences were found concerning socio-demographic and disease-related variables. Patient with university educational level had significantly better scores than patients with secondary educational level or less. Regarding the gender, there were no statistically significant differences between male and female patients in all of QOL domains.Concerning the age of patients, patients aged 26 years and more had better QOL domains such as physical functioning, general health, vitality, mental health, social functioning, emotional role, PCS and MCS in comparison with other age groups. The results also revealed that married patients had better scores than non-married in most of QOL domains. Moreover, employed patients with high income got better scores especially in mental health domain. According to health profile, patients with thalassemia intermedia have better status compared to those with thalassemia major in physical functioning, physical role, vitality, mental health, and emotional role and on both summary scales PCS and MCS. Finally, comorbidities did not have any significant effect on QOL scores.
5. Recommendations
- Based on the findings of the study, the following recommendations would be considered:1) Psychosocial support sessions should be scheduled regularly for patients and their families.2) Availability of social workers and psychologists in the centers are crucial to improve QOL.3) Policy makers and stakeholders should provide social and monetary support for patients and family members that in turn comprehensively reduce the disease burden and the improve QOL of thalassemia patients.4) Training and educating physicians and nurses how to communicate effectively with thalasemia patients to help them cope with their disease.
ACKNOWLEDGEMENTS
- I would like to express my gratitude to all patients who participated in the study. Many thanks also go to the administrations of Gaza European Hospital, and Al-Shifa hospital for their cooperation during the study period. Their sincere contributions made this research possible and fruitful.