-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2018; 8(4): 88-93
doi:10.5923/j.phr.20180804.02

Willingness to Teach, Perform and Other Views about Bystander Cardiopulmonary Resuscitation among Nigerian University Students Following Conventional and Hands-only Training Techniques
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: The bystander CPR training techniques (methods) could influence the willingness of participants to teach others CPR, perform it on victims of out-of-hospital cardiac arrest (OHCA) and their other general views about bystander CPR. This study aimed at comparing two cohorts of Nigerian undergraduate students’ willingness to teach others bystander CPR after training one group on hands-only CPR and the other on conventional CPR; their willingness to carry out bystander CPR after the trainings; and their other views about bystander CPR after the trainings. Materials and Method: Two cohorts of University undergraduate students (70 participants in each group) were trained on bystander CPR – one group on hands-only CPR and the other on conventional CPR. The two groups were randomly selected from the study population. After the trainings, they were served the same self-administered questionnaire on bystander CPR which they filled in during the pre-training stage. The data was analysed using descriptive statistics and analysis of variance (ANOVA) with the P-value set at P < 0.05. Results: 100% of the participants in both hands-only and conventional CPR training groups were willing to teach others CPR after the trainings with high percentages of the participants willing to perform it on different victims. Their overall willingness to teach bystander, perform it on victims and their other general views about bystander CPR were impressive and statistically the same in the two groups (P < 0.05), except in one item. Conclusion: The type of bystander CPR training technique did not significantly influence the participants’ willingness to teach and perform bystander CPR and most of their other views about bystander CPR.
Keywords: Hands-only, Conventional, CPR, Comparison, Willingness, Teach, Perform
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Willingness to Teach, Perform and Other Views about Bystander Cardiopulmonary Resuscitation among Nigerian University Students Following Conventional and Hands-only Training Techniques, Public Health Research, Vol. 8 No. 4, 2018, pp. 88-93. doi: 10.5923/j.phr.20180804.02.
Article Outline
1. Introduction
- Willingness is the quality or state of being prepared to do something; readiness, receptiveness, receptivity, openness – willingness or readiness to receive (especially impressions or ideas) [1].The challenge of the public health burden of out-of-hospital cardiac arrest (OHCA) involving both the developed and developing economies of the world is well documented [2-9]. In response, there have been reports on the need for bystander cardiopulmonary resuscitation (CPR) across the globe [10-17]. According to Mpotos et al [10], although many of the teachers studied claimed previous exposure to CPR training, only a minority of them was feeling competent and willing to teach bystander CPR to their students. Nigeria as a country has not done much in encouraging bystander CPR in line with the growing global trend. It was just recently and understandably so that there were some related Nigerian studies on bystander CPR [18-24]. However, the willingness of the laypersons to participate in the training and provision of bystander cardiopulmonary resuscitation (CPR) remains very key to achieving the target of having adequate number of potential bystander CPR providers in any community in case of emergency situations of out-of-hospital cardiac arrest (OHCA). It is known that the role of bystander CPR providers is central in the chain of survival in out-of-hospital cardiac arrest emergency cases.Although Nigeria is yet to have a defined policy on the promotion of bystander cardiopulmonary resuscitation, there is need to have more relevant data in our advocacy for incorporation of the training in bystander CPR into Nigerian schools’ curricula, including the primary, secondary and post-secondary institutions. This, by extension, will increase the number of potential bystander CPR providers in our communities. Therefore, this study aimed at comparing (1) some Nigerian undergraduate students’ willingness to teach others bystander CPR after exposing the two cohorts to the two CPR training techniques - conventional and hands-only; (2) their willingness to carry out bystander CPR after exposing the two cohorts of students to the two types of CPR training; and (3) their other views about bystander CPR after exposing the two cohorts to the two CPR training techniques. It was hypothesised that: (1) there would be no statistically significant difference in their willingness to teach bystander CPR after the CPR trainings in the two groups; (2) there would be no statistically significant difference in their willingness to perform CPR after the CPR trainings in the two groups; and (3) there would be no statistically significant difference in their other views about bystander CPR after the two CPR trainings.
2. Materials and Methods
2.1. Study Design
- This is a randomized experimental trial study involving seventy (70) participants in the hands-only cardiopulmonary resuscitation training group and seventy (70) in the conventional (standard) group. The participants are 200-level undergraduate Physical and Health Education students in the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria. The study took place in March, 2018.The study population was admitted into the Department of Human Kinetics and Health Education in 2016 and are studying to graduate with Bachelor of Education Degree (majoring in either Health Education or Human Kinetics). They are being trained primarily to become teachers in primary and secondary schools. These student teachers are from different parts of Nigeria.The following null hypotheses were generated and tested:Ho1: That there would be no statistically significant difference in their willingness to teach bystander CPR after the CPR trainings in the two groupsHo2: That there would be no statistically significant difference in their willingness to perform CPR after the CPR trainings in the two groups Ho3: That there would be no statistically significant difference in their other views about bystander CPR after the two CPR trainings
2.2. Stage 1 (Pre-training)
- Prior to the teaching and training on CPR, copies of a questionnaire containing a section on the demographic data of the participants and a section containing some questions on CPR to assess their pre-training cardiopulmonary resuscitation opinions were served to all the participants. The two groups of the participants (the ‘hands-only CPR training group’ and the ‘conventional CPR training group’) were served the same questionnaire to assess their pre-training bystander CPR willingness to perform bystander CPR, willingness to teach others about bystander CPR and their views about bystander CPR after they must have had the bystander CPR trainings.
2.3. Stage 2 (Training and Immediate Post-training)
- After the CPR teaching and training sessions, copies of the same questionnaire on CPR were distributed again to the same participants for re-assessment of their willingness to perform bystander CPR, teach bystander CPR and their views about bystander CPR using the same questions concerning CPR (See Appendix).
2.4. Determination of Satisfactory and Unsatisfactory Willingness for CPR
- For both groups, willingness to perform and teach CPR was dichotomized into ‘satisfactory’ and ‘unsatisfactory’ based on average score of 50%. Those with 50% and above were considered as having satisfactory willingness for CPR while any score less than that was considered unsatisfactory in line with Onyeaso and Onyeaso [25].
2.5. Statistical Analysis
- The Statistical Package for Social Sciences (SPSS) was used to analyze the data. In addition to descriptive statistics, one sample and two samples T-tests statistics were employed in the analysis and testing of the null hypothesis with significance level set at P < 0.05.
3. Results
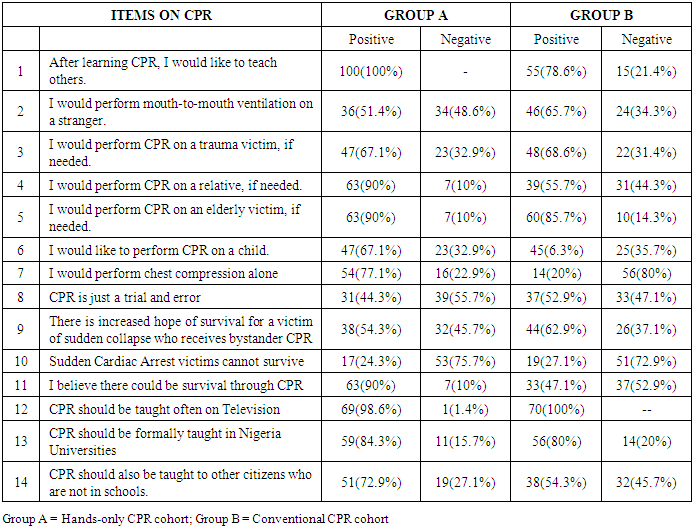
- Table 1 provides the pre-training willingness to teach, perform bystander cardiopulmonary resuscitation (CPR) and other views about bystander CPR for the two cohorts of Nigerian University undergraduate students. All the participants in the hands-only CPR cohort were willing to teach others CPR after learning while 78.6% in the conventional CPR cohort would want to teach others.
|
|
|
4. Discussion
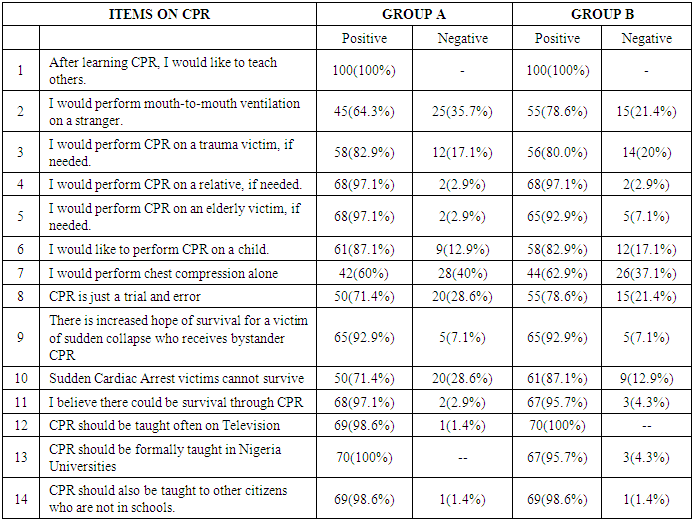
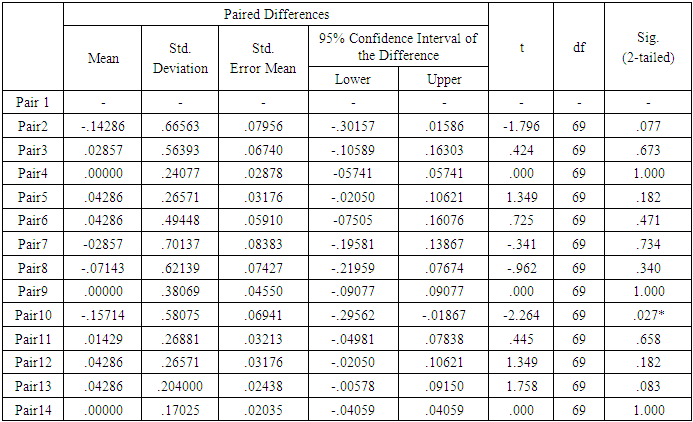
- This first comparative study on the willingness of Nigerian undergraduate students to teach and perform bystander CPR and their other views about bystander CPR between two cohorts trained in either hands-only CPR or the conventional CPR have shown that virtually all the variables did not show any significant difference between the two CPR methods except in one. This means that the CPR training method did not have any significant influence on the participants’ willingness to either teach CPR after training or perform it on different victims. The same applies to virtually all their other views about bystander CPR. According to Niklasson and Bohm [26], laypersons with CPR training were willing to perform bystander CPR to a greater extent than laypersons without CPR training. The laypersons with or without CPR training considered their actions very important in saving lives.Meanwhile, considerably more of the participants had positive responses towards bystander CPR than those who did not irrespective of the method of bystander CPR training. This is consistent with related earlier reports from Nigeria [20-24]. Similarly, Kanstad et al [27] reported that young Norwegians were motivated to perform bystander CPR despite known barriers and concluded that by providing students with good quality basic life support training in school, the upcoming generation in Norway might strengthen the first part of the chain of survival in out-of-hospital cardiac arrest cases. A report by Thoren et al [28] showed that major reasons for not being educated in CPR among cardiac patients were lack of awareness of the availability of CPR training for the public, lack of interest or lack of enterprise. Taniguchi et al [28] and Hunziker et al [30] reported that the main reasons for laypersons not showing willingness to perform bystander CPR were inadequate knowledge and doubt of being able to perform the techniques effectively, fear of disease transmission and fear of possible complications arising in the process. The study by Enami et al [31] showed that the new guideline on the basic life support slightly but significantly augmented the willingness to make an early call by the respondents. A systemic review of basic life support training targeting family members of high-risk patients revealed that although insufficient evidence on patient outcomes, family members are willing to be trained and to provide basic life support for high-risk patients. [32]. The review recommended further research to determine the impact on patient outcomes with possible alternate methods of patient follow-up such as out-of-hospital cardiac arrest (OHCA) and death registries while exploring the role of modern techniques for teaching and skill acquisition. Notwithstanding the type of bystander CPR training the participants received, the present Nigerian study has shown encouraging results of 100% or close to that desiring that bystander CPR should be taught in both television, in the Universities and other schools while 100% of them were willing to teach bystander CPR and impressive percentages willing to perform it.Among Flemish teachers, Mpotos et al [10] reported that 61% were not willing to teach CPR to their students while 69% felt incompetent to perform bystander CPR. Our present study gave 100% each for both hands-only CPR and conventional CPR at post-training stage while their willingness to perform bystander CPR for the various possible victims listed in our present study ranged from the least of 60% to over 97% in some. Although the lack of willingness to teach or perform CPR in the report of Mpotos et al [10] was related to absence of previous CPR training, the current finding immediately after training in our present Nigerian study is considered promising for participants who virtually had never had any previous CPR training.Strengths and Limitation of this StudyBesides being the first Nigerian report comparing the post-training willingness of participants to teach and perform bystander CPR and their other views on bystander CPR for two different cohorts trained on hands-only CPR and conventional CPR, the sample is very much fairly representative of Nigerian University youths because the students were admitted into the undergraduate programme of the University based on an Admission Policy (Quota System) which ensures good spread of the admitted students from different parts of the country. In addition, these students (undergraduates) are the potential primary and secondary school teachers who have the potential of influencing their future pupils and students through teaching/training and thereby increasing the potential bystander CPR providers in our communities. However, this study is limited by the relatively small sample sizes in the two cohorts, implying that the generalization of the results should be done with caution.
5. Conclusions
- This study has shown that generally the participants’ willingness to teach bystander CPR, perform it on victims of out-of-hospital cardiac arrest (OHCA) and their other views about bystander CPR were significantly the same despite the two different bystander CPR training methods employed.
6. Recommendations
- Further similar research should be carried out involving larger sample sizes from other parts of the country while encouraging the incorporation of the teaching / training of bystander CPR in Nigerian schools’ system from primary to the university level.