-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2018; 8(1): 24-30
doi:10.5923/j.phr.20180801.03

Knowledge of Food Safety and Practices among Cooked Food Vendors in the East Mamprusi District of the Northern Region of Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdadow Yidana, Akawani Philip
Department of Community Health and Family Medicine, School of Medicine and Health Science, University for Development Studies, Tamale, Ghana
Correspondence to: Adadow Yidana, Department of Community Health and Family Medicine, School of Medicine and Health Science, University for Development Studies, Tamale, Ghana.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Food safety has become a major public health concern globally as street food vending is a rapidly growing industry in both developed and the developing world. An increasing incidence of diarrhoea cases in Ghana is attributable to unhygienic street food vending. This study was carried out to assess knowledge and practices regarding food safety among cooked food vendors. The research design was a cross-sectional study. A sample size of 81 food vendors was selected. Data was collected using questionnaire. Results showed that 98.9% of the respondents were females. Majority of the food vendors had some knowledge on food safety and hygiene and knew that diarrheal diseases could result from food contamination and/or poisoning. 98% of the respondents said hand washing was necessary at all times but, only 13.6% washed their hands all the time and out of this only 45.5% washed their hands always with soap and running water. Only 21% store leftover foods in the refrigerator whilst 41% store food at room temperature. 35% of the respondents had undergone medical screening for food vendors and out of this percentage, 60% were screened more than six months ago. It was concluded that food vendors in East Mamprusi generally had a fair knowledge of food safety and hygiene but the practice of food hygiene was inadequate. Thus there is the need for health officials and the local government to periodically inspect and encourage food vendors to practice food hygiene and to always to be available for medical screening periodically.
Keywords: Food Safety, Hygiene Practices, Food Vendors, Mamprusi, Northern Ghana
Cite this paper: Adadow Yidana, Akawani Philip, Knowledge of Food Safety and Practices among Cooked Food Vendors in the East Mamprusi District of the Northern Region of Ghana, Public Health Research, Vol. 8 No. 1, 2018, pp. 24-30. doi: 10.5923/j.phr.20180801.03.
Article Outline
1. Background
- Food is any material consisting essentially of protein, carbohydrate, and fat used in the body of an organism to sustain growth, repair, and vital processes and to furnish energy [1]. The increasing number of fast food joints and local eateries in nooks and crannies of major cities and towns in Ghana has been recognized as one of the forces that serve to boost the economy. Street foods generally refer to ready-to-eat foods and beverages prepared either at home or on the streets and sold by vendors, especially on streets and other public places [2]. Statistics by the FAO [3] point out that, 2.5 billion people eat food prepared on the street every day. It is particularly so for women in the developing world, where food prepared on the street serve as a major source of livelihood providing a means of self-employment and the opportunity to develop business skills with low capital investment [4]. There are instances where these foods are not handled well, leading to foodborne diseases, a phenomenon that remains a major public health problem globally [5]. The safety of food prepared and sold on the street is a constant public health concern, and is supported by the fact that in both industrialized and developing countries; the rates of foodborne diseases are increasing and encompass a wide spectrum of illnesses. Estimates by the World Health Organisation [6] suggest that food-borne illnesses account for about 2.2 million deaths annually, out of which about 86% are children. In developing countries, up to an estimated 70% of cases of diarrheal disease are associated with consumption of unwholesome food [7]. Improper and disregard for hygiene measures on the part of food handlers may result in food contamination and its attendant consequences as [8] have alluded to, including food poisoning and spread of diseases with resultant morbidity and occasional mortality. In Africa where sanitation is still a major public health challenge, street foods are easily contaminated almost throughout the supply chain from production through preparation and processing to the final consumer. Street foods, particularly in developing countries have been reported to get contaminated by pathogenic bacteria that could lead to foodborne illnesses [9, 10]. In Africa, the incidence of both food and water-borne diseases is estimated at 3.3 to 4.1 episodes per child per year accounting for between 450,000 to 700,000 deaths in children annually, with many more sporadic cases not recorded [11]. An estimated hospitalization in Ghana due to food-related diseases stands at 420,000 per year, with an annual death rate of 65,000 people [12]. Interestingly, research has it that even vendors who exhibit knowledge about food hygiene still find it difficult associating dirty hands with the transmission of diarrheal pathogens in Ghana [13]. This leads to the argument that about 65,000 people die annually in Ghana from food-borne diseases resulting in the loss of some US$69 million to the economy [14]. The consumption of unwholesome foods creates a vicious cycle of disease, diarrhea, and malnutrition which may significantly impede public health and socioeconomic development. The number of people buying and consuming food prepared in public places has increased as a result of migration, changes in consumer demand and behaviour with urban dwellers needing cheaper foods in the face of harsh economic realities and as a consequence, the risk of foodborne illnesses are more prevalent due to challenges in food safety especially in regions where adequate resources have not been allocated for food safety control and intervention efforts [15]. The role of the food handlers especially the food vendors in effectively reducing the risk of foodborne diseases is critically important as they are in direct contact with the consumers and also, they are the least challenging in terms of implementing food safety control measures.
2. Study Design
- This study was a cross-sectional study design and involved a study of the food safety knowledge and practices among cooked food vendors in Nalerigu in the East Mamprusi district of the northern region of Ghana. The choice of the town was based on the fact that the main referral hospital is located there serving many people including Togolese and Burkinabes. Due to the numerous visitors to the township, cooked food vendors cook and serve them.
2.1. Study Population
- The study population comprised all cooked food vendors in the East Mamprusi district specifically Nalerigu township.
2.1.1. Sample Size Determination
- The sample size was determined using Krejcie & Morgan, (1970) formula for determining sample size for a finite population. Thus;
 Where:S = Required Sample size, X = Z value (e.g. 1.96 for 95% confidence level), N = Population Size, P = Population proportion (expressed as decimal) (assumed to be 0.5 (50%), d = Degree of accuracy (5%), expressed as a proportion (.05); the margin of error. Thus a sample size of 81 was determined. However, seven respondents were added to take care of non-respondents, making the entire sample size to be 88.
Where:S = Required Sample size, X = Z value (e.g. 1.96 for 95% confidence level), N = Population Size, P = Population proportion (expressed as decimal) (assumed to be 0.5 (50%), d = Degree of accuracy (5%), expressed as a proportion (.05); the margin of error. Thus a sample size of 81 was determined. However, seven respondents were added to take care of non-respondents, making the entire sample size to be 88. 2.2. Sampling Method
- A purposive sampling technique was used. The available food vendors in the community were approached with the help of an interpreter, the purpose of the study was explained to them. All of them granted us permission to go ahead with the data collection.
2.3. Data Collection Technique and Procedure
- A survey was done and a questionnaire in a form of structured interview was employed to elicit information from all the respondents. The questionnaire was made up of open and closed-ended questions. The questions were read out to the food vendors with the help of an interpreter in most cases (except those who could speak English language or Twi) and their response was recorded. For those who had difficulty understanding the questions, time was taken to explain in detail before they gave their responses. Data was collected by moving from one food vendor to another in a sequential manner throughout the mornings around 7:30 AM and later in the evening around 4:30 PM daily for five consecutive days.
3. Data Analysis
- Statistical Package for Social Science (SPSS 21st edition) was used to analyze the data. SPSS 21st edition was used to analyze the data. The demographic characteristics of the respondents (age, religion, and educational status) were analyzed by the use of frequency distribution table. Raw data collected on knowledge on food safety and hygiene practices were analyzed using frequency distribution tables and bar graphs. Raw data on the various questions dealing with hygiene practices of the respondents were analyzed with the aid of frequency distribution tables and bar graphs. Raw data collected on periodic medical screening and medical screening status of the food vendors were analyzed with frequency distribution tables and bar graph representations respectively.
3.1. Ethical Consideration
- Ethical clearance was obtained from the Department of Community Health and Family Medicine, University for Development Studies. Permission was also sought from the DHMT through the DDHS of the East Mamprusi District. Also before the face-to-face interview, the essence of the project was briefly explained to respondents and informed consent obtained.
4. Results and Discussion
4.1. Socio-demographic Characteristics
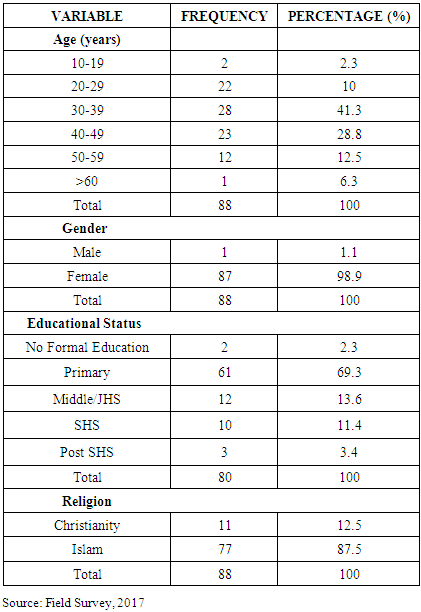
- From the data analysis on socio-demographic characteristics of the respondents, 2.3% were among the 10-19 age group, 25% were between 20-29 age group, 31% were between the age group of 30-39, 26.1% were between the 40-49 age group, 13.6% were between the 50-59 year group and 1.1% were 60 years and above (Table 1). Interestingly, 98.9% of the respondents were females whiles 1.1% were males. The skewness of food vending towards women side may be explained by the perceived gender role of women. This tie-in with Tomlins et al. [16] claim which suggest that majority of food vendors in Accra Ghana were female. The results further showed that 87.5% the respondents were Muslims whilst the remaining 12.5% were Christians. Additionally, 2.3% of the respondents had no formal education, 69.3% of them had primary education, 13.6% had Middle/Junior High School education, 11.4% had Senior High School (SHS) level education and 3.4% had a post-SHS formal education. A cumulative percentage of 97.7% of the total respondents had some form of formal education. This finding shows relatively higher percentage coverage for respondents as against 67% of respondents who have had formal education in a similar research by Apanga, et al. [17]. Formal education is important in the food vending industry because the low level of education could be linked to poor food hygiene practices which could lead to food contamination during food handling, storage, and food preparation.
|
4.2. Knowledge of Food Hygiene
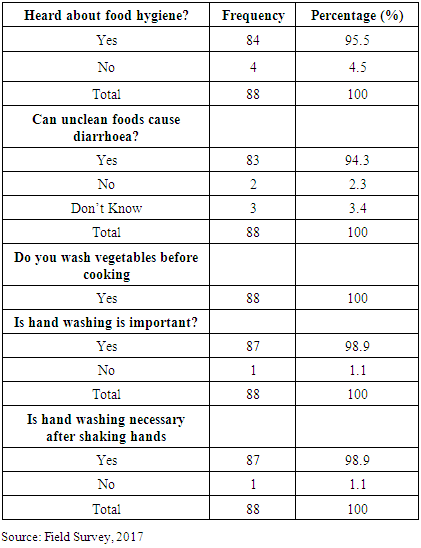
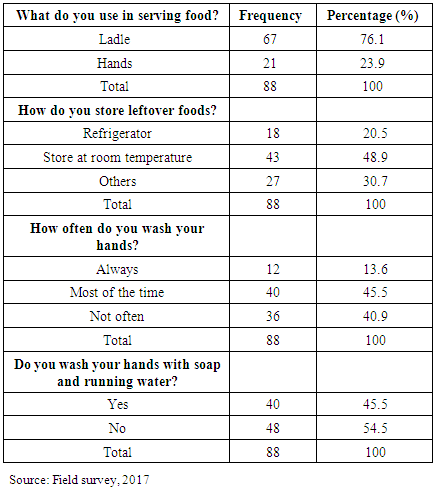
- The study showed that 95.5% of the respondents have heard about food hygiene and could literally expound on the subject of food hygiene. In the same way, 94.3% of the respondents could explain that unclean food could cause diarrheal diseases (Table 2). All the respondents (100%) indicated that they washed vegetables before using them to prepare food. They also indicated that they cover cooked food they sell to the public against flies and other foreign agents. These findings tie in well with Apanga et al. [17] who revealed that knowledge about food safety among street food vendors in rural northern Ghana was 100%. The result is also consistent with Dun-Dery and Addo [18] who claimed that 87% of their respondents were found to be knowledgeable about foodborne diseases and food safety. These two findings contradict what pertains in other countries as Abdalla et al. [19] have indicated that a study in Sudan showed that only 30% of the respondents had knowledge on the foodborne disease and food safety. All the respondents (100%) agreed that hand washing is an integral part of adhering to hygiene practices in the food industry. In the same vein, 98.9% of the respondents demonstrated knowledge of when it becomes necessary to wash hands (after blowing the nose, after shaking a friend, before serving food, etc). This finding is contrary to Abdalla et al. [19] which showed that 70% of food vendors in their study did not see the need to wash hand after scratching or after continuous handling of food. In the same study by Abdalla et al. [19], the majority, however, agreed that washing of hands after eating and after using the toilets is important.
|
4.3. Food Safety Practices
- With respect to safety practices, the study revealed that 13.6% of the respondents relied on pipe borne water for cooking, 47.7% of them relied on well-water (deep/shallow) and 38.6% of them rely on borehole water for cooking (Fig 1). It also emerged that 14.8% of the respondents relied on standpipe for drinking purposes, 45.5% rely on well-water whilst 39.8% rely on the borehole for drinking. The faeco-oral route of transmission of diarrheal diseases particularly enteric fever (typhoid fever) could be traced to the source of their drinking water. This is contrary to findings of Donkor et al. [20] which found that 99% of the source of water for cooking the by food vendors in Accra was standpipe water. This difference in access to standpipe water, one may speculate is purely a developmental gap as the south is more developed than the northern part of Ghana. But in Sudan, only 60% of food vendors used tap water for cooking and yet a current research even showed a much lower percentage, (39%) having access to pipe borne water [21].
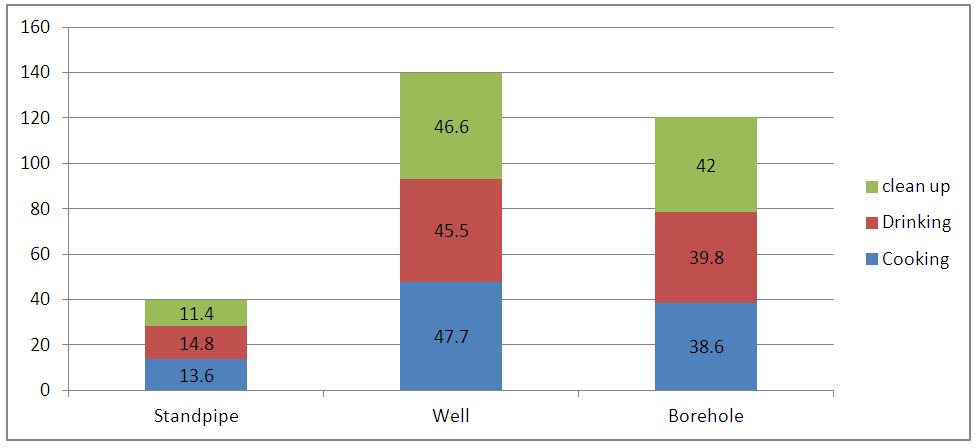 | Figure 1. Source of water (Source: Field survey, 2017) |
|
4.4. Education on Food Safety and Hygiene
- Majority of the respondents (95.5%) indicated that they regularly receive education on food safety and hygiene from different sources. Out of that proportion, 33.3% predominantly received these educational messages from television shows, 35.6% received these educational messages from radio talk shows, 16.1% received education through health officials (sanitary health inspectors and community health nurses), and 15.9% were also educated on food safety through other avenues like community durbars, health talks by the health personnel from health institutions and health talks organised during seasonal meetings of the local Food Vendors Association in Nalerigu. These sources contribute significantly towards helping food vendors in the area to fully appreciate and comply with the food safety principles.
4.5. Periodic Medical Screening of Food Vendors
- Results on periodic medical screening for food vendors showed that 73.9% of the respondents had heard about medical screening exercise for food vendors as against 26.1% who have never heard of it before (Fig 2). Approximately 40% of those who have heard about the medical screening have undergone screening for HIV/AIDS, Typhoid fever, Hepatitis B, and Hepatitis C whilst the greater majority (60%) have never undergone medical screening for the above illnesses. Additionally, 39.8% of those who have undergone medical screening did that in the last six months whilst the remaining 60.2% undertook their recent medical screening more than six months ago.
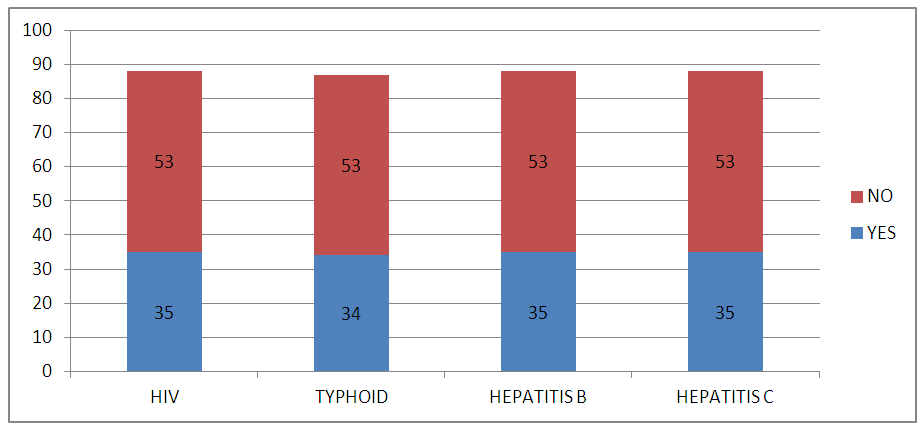 | Figure 2. Medical screening of food vendors (Source: Field Survey, 2017) |
5. Conclusions
- It is referenshing to note that many food vendors have knowledge about food hygiene and food safety practices. Majority of the food vendors washed their hands before serving food, after visiting the toilet. However, quite a number of food vendors still use their bare hands to serve clients. In addition, many of them have not gone through screening for possible diseases. In view of the above, there is the need for public health experts to intensify their campaign on food safety especially the need to screen oneself before joining the food vending business.
ACKNOWLEDGEMENTS
- Authors acknowledge the immense assistance received from the authors whose articles are cited and included in references to this manuscript. The authors appreciate the editors and publishers of all those articles, journals, and books from where the literature for this manuscript has been reviewed and discussed.