-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2017; 7(6): 136-142
doi:10.5923/j.phr.20170706.02

Demand for Reproductive Health Vouchers and Utilization: A Case Study of Output Based Approach in Kilifi Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMary N. Mwangangi1, Urbanus Kioko2, Julius Korir3
1Economist, Ministry of Health, Nairobi, Kenya
2School of Economics, The University of Nairobi, Kenya
3School of Economics, Kenyatta University, Kenya
Correspondence to: Mary N. Mwangangi, Economist, Ministry of Health, Nairobi, Kenya.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Demand side financing initiatives are different forms of financing health services that aim to minimize financial obstacles to accessing health care and also decrease inequities by ensuring that services are made affordable to poor and underserved populations through provision of subsidies. Vouchers have been expected to improve health outcomes by improving on service quality, improving effectiveness while also increasing the utilization of health care services. Despite the fact that vouchers have been implemented in Kenya since 2006, very few studies have focussed on underlying factors that contribute to low utilization even with high demand for the vouchers particularly in Kilifi County. This study investigates the relationship between demand and household and individual characteristics and also the relationship between utilization and household characteristics. The findings indicate that age, education, marital status and occupation had a relationship with demand for the reproductive health vouchers while for utilization of the vouchers only age and marital status were found to be statistically significant.
Keywords: Vouchers, Utilization, Demand
Cite this paper: Mary N. Mwangangi, Urbanus Kioko, Julius Korir, Demand for Reproductive Health Vouchers and Utilization: A Case Study of Output Based Approach in Kilifi Kenya, Public Health Research, Vol. 7 No. 6, 2017, pp. 136-142. doi: 10.5923/j.phr.20170706.02.
Article Outline
1. Introduction
- High cost of healthcare remains a big challenge particularly for the poor groups of the population with very little income; hence vouchers have been used as one of the many ways to deliver assistance in health particularly in many developing countries across the world. Vouchers used for accessing health are a demand side financing mechanism that has been adopted by many developing countries as a way to enhance utilization and service access [10]. Vouchers have been implemented in several countries such as Nicaragua, Bangladesh, Tanzania and Kenya, others especially in reproductive, maternal plus child health as a way of improving the poor health indicators. Vouchers remove barriers to access to services and therefore their demand is usually high since more of the targeted individuals are able to afford. Voucher programs are also known to incentivize health care workers in order to increase their motivation and improve on service delivery in general [25]. Implementation of the voucher scheme in Tanzania has shown that stimulating demand for health services through a subsidized voucher can greatly increase the use of certain targeted services particularly for the poor who are financially constrained [11].High cost of healthcare remains a big challenge particularly for the poor groups of the population with very little income; hence OBA increases the access to these services by creating demand for the services through a subsidized voucher. Therefore, by financing services on the demand side, OBA is aimed at ensuring better access and service utilization, thus contributing towards a decline in neonatal and maternal death [14].The sale of the OBA voucher has seen an increase in demand over the years the programme has been implemented in Kilifi County. However, the low use of demanded vouchers raises a serious concern for policy makers on the underlying reasons that lead individuals to purchase vouchers then end up not using them for the range of services covered. Few studies have focussed on the issue of low utilization of vouchers. Given the policy importance of the programme, there is need to understand the reasons for the relatively low utilization of vouchers. Kilifi County has poor maternal and child health indicators hence understanding reasons for low use of vouchers can help in addressing these issues hence improving the health of women and children in the area and the country in overall and help in achieving both local and international health goals and obligations.Theoretical literature reviewed provides an understanding of the theoretical approaches and models used in understanding the demand and utilization of health services and the factors that affect the decision to demand and use health services. Grossman looks at how health status, age, education and income stimulate how health is produced through the demand for capital for health [9]. The Grossman model yields health care demand as a function of medical care inputs and education. Health is viewed as a capital good, in addition to being both consumption and an investment good. Individuals make choices between two alternatives based on the output or outcome expected from each alternative and that an individual will opt for the alternative that produces more output for him/her [22]. One may obtain the reliable estimates of the parameters using the probit method that may be appropriate to use on the dichotomous variable then using the OLS method thereafter to avoid the problem of selectivity bias [12]. Maddala further stated that these models of self-selectivity may be used to evaluate the benefits of social programs [22].From the empirical literature reviewed, variables have different influences on how demand for health care is shaped in the different studies. The impact of price on various groups with different incomes showed that responsiveness to changes in prices was highly noted among the poor than those who are not poor [29]. They also found that women, people from bigger households and those with longer periods of illness were highly likely to seek care.The discrete choice demand model was used to study the outpatient healthcare demands in the rural zones of Kenya and it was found that numerous individual and household characteristics influence the probability of reporting sickness. The likelihood of whether to report an illness is independent of the utility of looking for treatment [7].A study on the Tanzania voucher scheme sought to establish how subsidies on the prices of insecticide treated nets (ITN) affect the decision by households to buy nets. It was also found that subsidies on price have a positive effect on the coverage for mosquito nets in Tanzania. It was also noted that implementing subsidies on price alone may not help in achieving targets to cover more people among the vulnerable populations [8].Muriithi in his study seeking to establish how health seeking behaviour is influenced by evidence on the quality of health care found that distance, quality of care, land acreage, education, size of the household, waiting time, gender and patient trust affected the decision to seek care [23].Women originating from areas that had been involved in the OBA programme from the year 2006 were considerably more probable to have had their deliveries at a health facility with skilled care in comparison with the ones from areas that had never been involved in the programme [26].Most of the studies from the literature reviewed have focussed on demand and utilization of general services. Further, some have had nationwide focus while others have been focussed in other areas other than area of study (Kilifi). This study seeks to identify underlying factors in low use of vouchers and how the policy recommendations can be implemented in Kilifi and can be adopted in other OBA sites and the country in general.
2. Study Objective
- The study seeks to assess how demand and utilization of OBA health vouchers is shaped in Kilifi County with the focus on low utilization so as to provide policy makers with information that can be used for decision making when designing health programs for the country to ensure that they contribute to the overall health goals.
3. Methodology and Data
3.1. Theoretical Framework
- Discrete choice modelThis model is applied to determine the elasticity of price on health care demand. This model portrays the kind of health services to be consumed and where they are to be consumed. The variable that is dependent is usually determined as the frequency of utilization for different health facilities types or in some instances the amount of health care consumed/utilized is used to determine the demand for health care. This model is obtained from the Random Utility Model (RUM) which conveys the rational theory of the utility of the customer [32]. The utility that is observed comes from the options that are equally exclusive, limited and comprehensive in the discrete model.This model is used when there is a need to clarify or forecast choices among two or additional options for example, whether to seek care or not. These models are able to specify the options that people make if faced by a set of different alternatives. In discrete choice models, the individual is mainly the decision maker and these models are able to associate the decision made by an individual to the characteristics of the individual and also the characteristics of the alternatives/options accessible to the person. The main characteristics of the discrete choice model include: (i) there must be a set of choices available to an individual, (ii) the probabilities of choosing an option must be defined and (iii) utility theory may be used to derive discrete choice models.The utility function is as follows:
 | (1) |
 | (2) |
 | (3) |
 | (4) |
 | (5) |
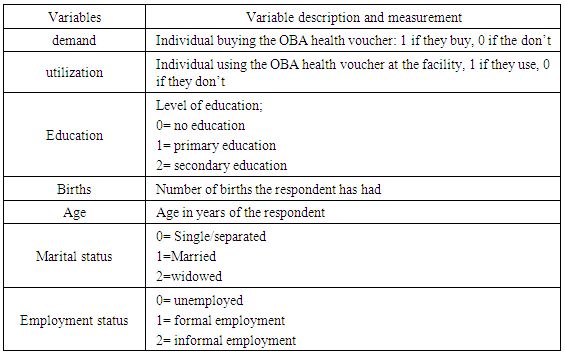
 Where Ui represents the demand and utilization dummies, Ni represents the independent variables and ei is the error termTable 1: Variables, Definition, Categories and Expected SignThis section provides a definition of variables used in the two models. The dependent variables are: utilization and demand of the OBA health voucher.
Where Ui represents the demand and utilization dummies, Ni represents the independent variables and ei is the error termTable 1: Variables, Definition, Categories and Expected SignThis section provides a definition of variables used in the two models. The dependent variables are: utilization and demand of the OBA health voucher.
|
3.2. Data Source
- Data was collected through administering the questionnaire and secondary data sources from existing records. Data on voucher sales from the OBA database was analysed together with data collected from individual responses in order to generalize findings. The minimum sample was 376 but the target was 450. The sample size was distributed proportionately amongst those who purchased the voucher and did not use and those who purchased and used in the Kilifi County for the year 2013.
4. Results and Discussion
- A summary of the results for the demand and utilization model are presented in this section.
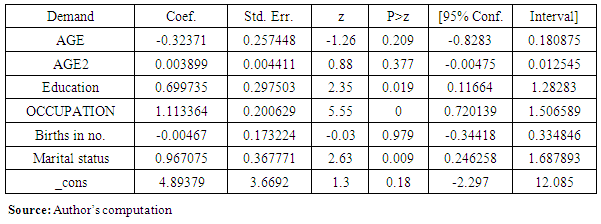
4.1. Determinants of Demand for OBA Health Vouchers
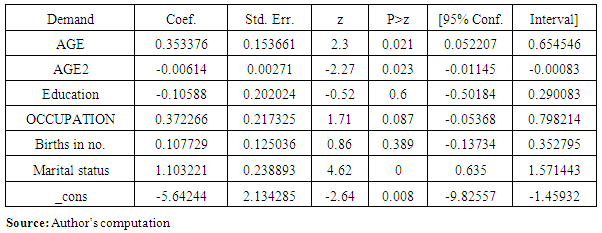
- Table 2 shows the relationship between the dependent and independent variables using the logit model with coefficients of the independent variables at 95% confidence level. The coefficients on education, marital status and occupation were statistically significant at 5% level of significance while age and births were not significant. The coefficient on age was negative implying that an increase in age reduces the demand for the voucher. The coefficient on age squared was positive meaning that an increase in age increases the demand for the voucher. These results on age and age squared show that at a younger age, the demand for the reproductive health vouchers is low but increases as the age increases.
|
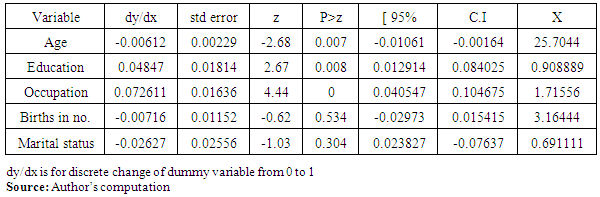
4.2. Marginal Effects in Explaining the Demand for OBA Vouchers
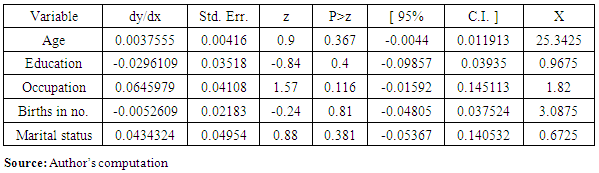
- Table 3 shows the estimated results from the probit model which was used to measure the impact a change in the independent variable has on the expected change of the dependent variable. From the table, inference can be made that education and occupation increases the probability of an increase in demand for OBA health vouchers. The other variables that is, age, births in number and marital status were found to reduce the probability of demand for the vouchers.
|
4.3. Determinants of Utilization of OBA Health Vouchers
- Table 4 shows the relationship between the dependent (utilization) and independent variables using the logit model with coefficients of the independent variables at 95% confidence level. The coefficients that were statistically significant at 5% level were age, age squared and marital status. The coefficient on age was positive implying that an increase in age increases the utilization for the voucher. The coefficient on age squared was negative meaning that an increase in age decreases the utilization for the voucher. These results on age and squared imply that people of a younger age are more likely to utilize the voucher as compared to the older ones.
|
|
4.4. Marginal Effects in Explaining the Utilization of OBA Vouchers
- Table 5 shows the estimated results from the probit model which was used to measure the impact a change in the independent variable has on the expected change in the dependent variable. From the table, inference can be made that age, marital status and occupation may increase the probability utilization for OBA health vouchers. The other variables, that is, education and births in number were found to reduce the probability of utilization for the vouchers.
5. Conclusions
- The purpose of conducting this research was to come up with a detailed analysis of how demand and utilization of OBA health vouchers is shaped by the individual characteristics and those of the household. Further analysis of these individual and household characteristics can provide an avenue for policy making on matters such as how to improve demand and utilization of health services in general. The demand for the OBA voucher has been used as a way of cushioning poor households from experiencing high out of pocket expenditure. High out of pocket expenditure has the tendency to push poor households further into poverty and deny them access to health care services when they need them [13]. Hence these findings may be useful in informing the development of health insurance by looking at how individuals choose to invest in the voucher as a means of preventing payment at the point of service.Education, marital status and occupation were found to have a relationship with demand for OBA health vouchers. An increase in education and occupation increase the demand for reproductive health voucher, this implies that the more educated you are the more information you may have regarding your health and the benefits of having a form of health insurance and it therefore gives you an upper hand in decision making in terms of how to invest in your health. In terms of occupation, the findings imply that having a source of income gives you the economic power to decide on what health investments to make. Age and number of births did not have any association with demand for the OBA reproductive health vouchers. From the results, education plays a key role in the demand for the health voucher hence may be important in influencing the demand for health insurance as a way of cushioning individuals from out of pocket expenditure.The findings from the utilization model suggested that only age and marital status were found to be statistically significant with both of them having a positive coefficient meaning that an increase in age or a change in marital status increases the probability of utilization of the OBA health voucher. Age squared was significant with a negative coefficient thus implying that utilization of vouchers increases up to a certain point then begins to decrease as age increases. Education, occupation and births did not have any association with utilization of the voucher meaning that they do not affect the decision to utilize health services hence suggesting that utilization may be based on the need to seek care/presence of an illness among other factors and not just demand side factors. There is need to work on supply side interventions by increasing the capacity of health facilities to improve service delivery and utilization of health care services [1].Further studies and analysis may be needed to establish other factors that affect the decision to utilize health services other than the variables analysed.The major study limitation was difficulty in reaching the respondents, however this study provides valuable information on what could be done to improve demand side financing initiatives and its contribution to health financing in general.