-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2016; 6(4): 110-118
doi:10.5923/j.phr.20160604.03

Application of Multilevel Binary Logistic Regressions Analysis in Determining Risk Factors of Diarrheal Morbidity among under Five Children in Ethiopia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYilkal Messelu1, Kassahun Trueha2
1MSCinBiostatistics, Departement of Statistics, MizanTepi University, Ethiopia
2MSCinAppliedStatistics, Departement of Statistics, MizanTepi University, Ethiopia
Correspondence to: Yilkal Messelu, MSCinBiostatistics, Departement of Statistics, MizanTepi University, Ethiopia.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Diarrheal disease is the most common cause of illness and the second leading cause of child death in the world. The burden is greatest in the developing world including Ethiopia. The purpose of this study has been to identify socio-economic, demographic, environmental and nutrition proximate predictors that affecting diarrheal morbidity of under-five children in Ethiopia. In this research data from the Ethiopian Demographic and Health Survey conducted in 2011 was used. Multiple and multilevel binary logistic regressions were employed for data analysis. The prevalence of diarrhea, stunting, wasting, and underweight among under-five children were 15.6%, 37%, 10.2% and 35.3% respectively. Both in multiple binary logistic regression and multilevel logistic regression, it was found that age of child, maternal working status, duration of breast feeding, stunting, wasting, and underweight were significant determinants of childhood diarrhea. From multilevel logistic regression, it was found that the random intercept and fixed coefficients model provided the best fit for the data under consideration. The variance of the random component related to the intercept term was found to be statistically significant implying differences in prevalence of diarrhea among the regions. However, the significant predictors did not show underlying variation from region to region. Therefore, the concerned body should give implement on nutritional intervention activities at all level of the community and Efforts should be invested to educate parents about the importance of breastfeeding and initiate to adopt the culture of breastfeeding their children to reduce the exposure of children to diarrhea. Researchers should use multilevel models than traditional regression methods when their data structure is hierarchal as like in EDHS data.
Keywords: Diarrhea, Under five children, Multilevel logistic regression
Cite this paper: Yilkal Messelu, Kassahun Trueha, Application of Multilevel Binary Logistic Regressions Analysis in Determining Risk Factors of Diarrheal Morbidity among under Five Children in Ethiopia, Public Health Research, Vol. 6 No. 4, 2016, pp. 110-118. doi: 10.5923/j.phr.20160604.03.
Article Outline
1. Introduction
- Diarrhea remains one of the most common illnesses of children and one of the major causes of infant and childhood mortality in developing countries [1]. Diarrhea is caused by ingesting certain bacteria, viruses or parasites found in fecal matter which may be spread through water, food, hands, eating and drinking utensils, flies, and dirt under fingernails [2]. Diarrhea can last several days, and can leave the body without water and salts that are necessary for survival. Most people who die due to diarrhea actually die as a result of severe dehydration and fluid loss. Children who are malnourished or have impaired immunity are the most vulnerable for life threatening diarrhea [3].Globally, diarrhea is the third largest cause of morbidity and the sixth largest cause of mortality among population of all ages [4]. Diarrhea disease accounts for approximately 1.34 million deaths among children aged 0-59 months and continued as the second leading cause of death [5].It is widely recognized that exposure to diarrhea pathogens in developing countries is determined by age of the child, quality and quantity of water, availability of toilet facilities, housing conditions, level of education, household economic status, place of residence, feeding practices and the general sanitary conditions (personal or domestic hygiene) around the house [6]. Persons living in developing countries with poor access to safe water, sanitation, or hygiene infrastructure have increased risk of exposure to viral, bacterial, and parasitic pathogens that can cause diarrheal [7, 8].In Africa, a child experiences five episodes of diarrhea per year, and 800,000 children die each year from diarrhea related dehydration [9].In Ethiopia, morbidity reports and community-based studies indicate that diarrheal diseases are a major public health problem that causes excess morbidity and mortality among children [10]. The two-week period prevalence of diarrhea among under-five children in Ethiopia and Oromia region were 30.6% and 17.7%, respectively [11]. The 2000 Ethiopia DHS reported that 24 percent of under-five children have experienced diarrhea in the last two weeks prior to the survey [12]. Child diarrheal morbidity remains a major public health problem in Ethiopia. Diarrhea cannot be tackled without understanding its causes that is why the study was crucial to identify the major socio-economic, demographic, nutritional and environmental factors of childhood diarrhea and to estimate the within-regional and between-regional level of difference for the incidence of diarrhea among under five-children in Ethiopia.
2. Material and Methods
- Data for this study were taken from the 2011 Ethiopian DHS which was conducted for the third time in Ethiopian the first one being in 2000. Information regarding fertility and family planning behavior, child mortality, nutritional status of children, utilization of maternal and child health services, and knowledge of HIV/AIDS and sexually transmitted diseases (STDs) is available from the data set. The 2011 Ethiopian Demographic and Health Survey (EDHS) is designed to provide estimates for the health and demographic variables of interest for the following domains: Ethiopia as a whole; urban and rural areas of Ethiopia (each as a separate domain); and 11 geographic areas (9 regions and 2 city administrations). In general, the DHS sample is stratified, clustered and selected in two stages. In the 2011 EDHS a representative sample of approximately 17817 households from 624 clusters was selected. In the first stage, 624 clusters (187 urban and 437 rural) were selected from the list of enumeration areas based on the 1994 Population and Housing Census sample frame. A total of children less than 59 months were identified in the households of selected clusters. From 11654 children aged less than 59 months only 9554 were measured for anthropometric measurements height and weight, and with complete information. Thus, the analysis presented in this study on nutritional status will be based on the 9554 children aged less than 59 months.
2.1. Variables Considered in the Study
- The response variable of the study is the two weeks incidence of diarrhea prior to the survey and based on the available information, this study examined the influence of the following risk factors for causing diarrhea. Five categories of factors were assessed as independent variables;i. Socio-economic and demographic variables; family size, income, place of residence, maternal education and working status, Marital status, and religion.ii. Child characteristics; Age, Sex, birth order, preceding birth interval, size of child at birth, Having fever recently, and Experience of cough iii. Child caring practices; feeding practice, maternal access to health facilities, and Vaccination status of a child.iv. Maternal Caring and characteristics; number of children ever born, maternal health care, Breast feeding practice, v. Environmental Health condition; Water supply, sanitation and housing conditionsvi. Child anthropometry indicators: stunting (chronic malnutrition), wasting (acute malnutrition) and underweight.
2.2. Statistical Methodology
- In this study single and multilevel logistic regressions were employed to identify determinant factors of diarrheal morbidity among under-five children and to predict the two weeks probability of under-five children experiencing diarrhea. The response variable of the study is the two weeks incidence of diarrhea prior to the survey. Firstly, single level binary logistic regressions was analysed by assuming the occurrence of diarrhea was independent among under-five children. And finally we assessed the effect of determinant factors and regional difference on incidence of diarrhea using multilevel logistic regression model.
2.2.1. Binary Logistic Regression Model
- Let
 be a dichotomous outcome random variable with categories 1 (presence of diarrhea) and 0 (absence of diarrhea) in the two weeks prior to the survey. Let
be a dichotomous outcome random variable with categories 1 (presence of diarrhea) and 0 (absence of diarrhea) in the two weeks prior to the survey. Let  denote the collection of k-predicator variables of the response. Then, the conditional probability that the
denote the collection of k-predicator variables of the response. Then, the conditional probability that the  child has diarrhea given the vector of predictor variables
child has diarrhea given the vector of predictor variables  is denoted by
is denoted by  The expression
The expression  in logistic regression model written in linear combinations of predictors can be expressed in the form of:
in logistic regression model written in linear combinations of predictors can be expressed in the form of: 
2.2.2. Multilevel Logistic Regression Model (Two-Level)
- Multilevel models are statistical models which allow not only independent variable at any level of hierarchical structure but also at least one random effect above level one group [13].The binary multilevel logistic regression model has a binary outcome (presence or absence of diarrhea). In this study the basic data structure of the two-level logistic regression is a collection of N groups (regions) and within-group

 a random sample
a random sample  of level-one units (children). The response variables, i.e., we let
of level-one units (children). The response variables, i.e., we let  if the ith under five children in jth region has diarrhea, and
if the ith under five children in jth region has diarrhea, and  otherwise; with probabilities,
otherwise; with probabilities,  is the probability of having diarrhea for children
is the probability of having diarrhea for children  in region
in region  and
and  is a random cluster effect and often assumed to be
is a random cluster effect and often assumed to be  The standard assumption is that
The standard assumption is that  has a Bernoulli distribution. Let
has a Bernoulli distribution. Let  be modeled using a logit link function. The two-level model is given by:
be modeled using a logit link function. The two-level model is given by: Where
Where  Then level-two model can be rewritten as:,
Then level-two model can be rewritten as:, Where
Where  represent the first and the second level covariates,
represent the first and the second level covariates,  are regression coefficients,
are regression coefficients,  are the random effect of model parameter at level two.
are the random effect of model parameter at level two. 2.2.2.1. Empty Multilevel Logistic Regression Model
- The empty two-level model for a dichotomous outcome variable refers to a population of groups (level-two units) and specifies the probability distribution for group-dependent probabilities pj in
 without taking further explanatory variables into account. We focus on the model that specifies the transformed probabilities
without taking further explanatory variables into account. We focus on the model that specifies the transformed probabilities  to have a normal distribution. This is expressed, for a general link function f (p), by the formula
to have a normal distribution. This is expressed, for a general link function f (p), by the formula where
where  is the population average of the transformed probabilities and
is the population average of the transformed probabilities and  is the random deviation from this average for group j. If f (p) is the logit function, then
is the random deviation from this average for group j. If f (p) is the logit function, then  is just the log-odds for group j. Thus, for the logitlink function, the log-odds have a normal distribution in the population of groups, which is expressed by:
is just the log-odds for group j. Thus, for the logitlink function, the log-odds have a normal distribution in the population of groups, which is expressed by: For the logit function, the so-called logistic transformation of
For the logit function, the so-called logistic transformation of  is defined by
is defined by Note that due to the non-linear nature of the logit link function, there is no a simple relation between the variance of probabilities and the variance of the deviations
Note that due to the non-linear nature of the logit link function, there is no a simple relation between the variance of probabilities and the variance of the deviations  [14]).
[14]). 2.2.2.2. Random Intercept Model
- In the random intercept model the intercept is the only random effect meaning that the groups differ with respect to the average value of the response variable, but the relation between explanatory and response variables cannot differ between groups. These variables are denoted by
 with their values indicated by
with their values indicated by  since some or all of those variables could be level one variables, the success probability is not necessarily the same for all individual in a given group [14].The random intercept model expresses the log-odds, i.e. the logit of
since some or all of those variables could be level one variables, the success probability is not necessarily the same for all individual in a given group [14].The random intercept model expresses the log-odds, i.e. the logit of  as a sum of a linear function of the explanatory variables. That is,
as a sum of a linear function of the explanatory variables. That is, where the intercept term
where the intercept term  is assumed to vary randomly and is given by the sum of an average intercept
is assumed to vary randomly and is given by the sum of an average intercept  and group-dependent deviations
and group-dependent deviations  that is
that is As a result we have:
As a result we have: 
 Thus, a unit difference between the Xh values of two individuals in the same group is associated with a difference of
Thus, a unit difference between the Xh values of two individuals in the same group is associated with a difference of  in their log-odds, or equivalently, a ratio of
in their log-odds, or equivalently, a ratio of  in their odds.
in their odds. 2.2.2.3. Random Coefficient Multilevel Logistic Regression Model
- Suppose that there are
 level-one explanatory variables
level-one explanatory variables  and consider the model where all predictor variables have varying slopes and random intercept. That is
and consider the model where all predictor variables have varying slopes and random intercept. That is Letting
Letting  and
and  where
where  we have:
we have: The first part
The first part  is called the fixed part of the model, and the second part,
is called the fixed part of the model, and the second part,  is called the random part of the model. The random variables or effects
is called the random part of the model. The random variables or effects  are assumed to be independent between groups but may be correlated within groups. Data processing First the data checked for completeness and consistency. Then it was coded and entered in the computer using EPI6 software. The software has a program (Epi – Nut) to convert nutritional data into Z – scores of the indices; H/A, W/H and W/A taking age and sex into consideration using NCHS reference population standard of WHO then, the data exported to SPSS and STATA program for analysis.
are assumed to be independent between groups but may be correlated within groups. Data processing First the data checked for completeness and consistency. Then it was coded and entered in the computer using EPI6 software. The software has a program (Epi – Nut) to convert nutritional data into Z – scores of the indices; H/A, W/H and W/A taking age and sex into consideration using NCHS reference population standard of WHO then, the data exported to SPSS and STATA program for analysis.3. Results and Discussions
3.1. Result
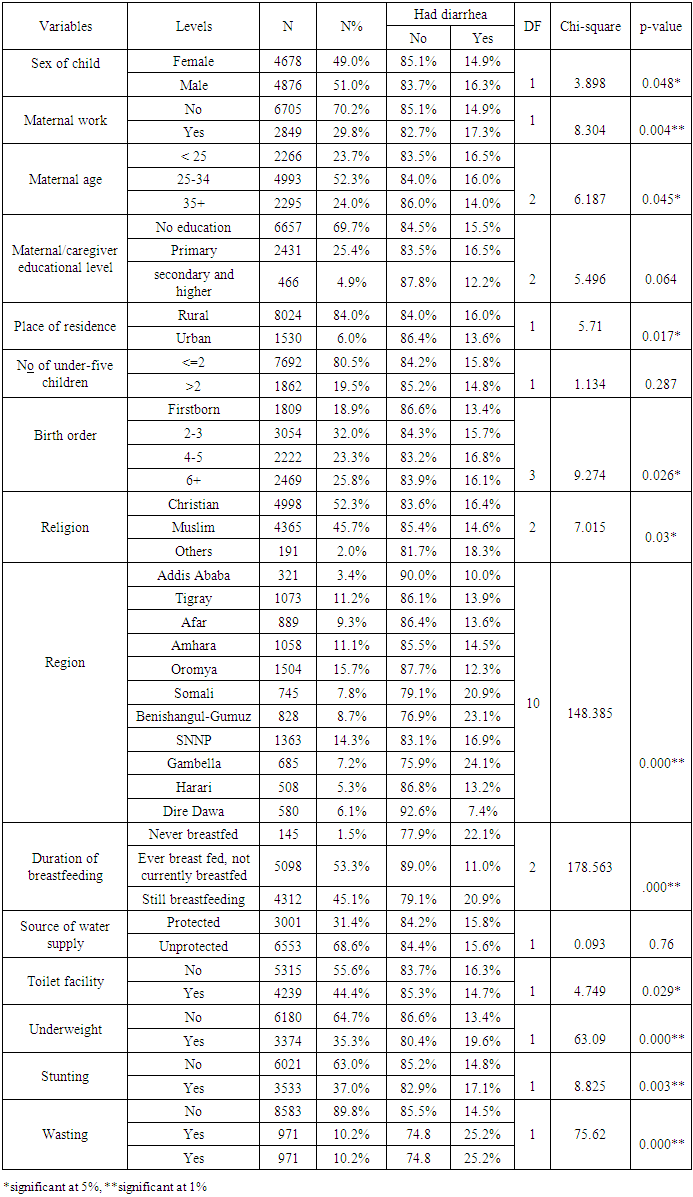
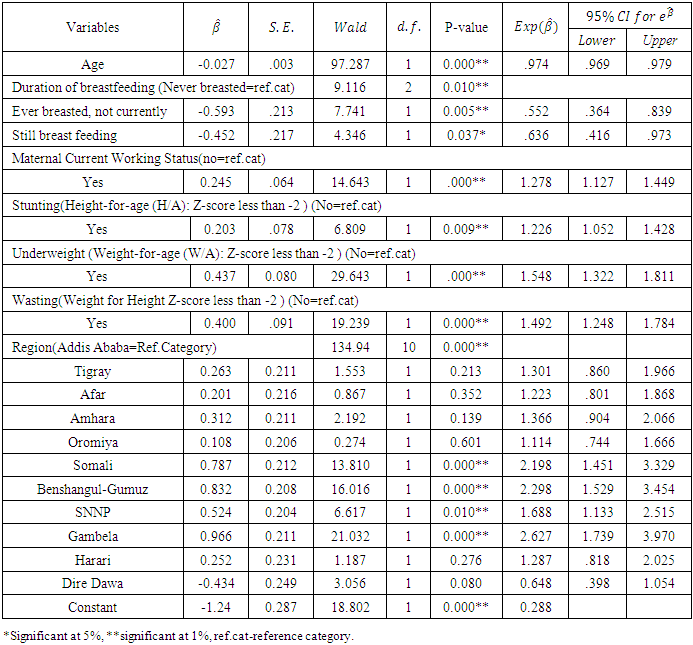
- From sampled children, the two weeks prevalence of diarrhea among under-five children was about 15.6% in Ethiopia. Table 1 show that religion, place of residence, sex of child, birth order, geographical region, duration of breastfeeding, stunting, wasting, and underweight were significantly associated with incidence of diarrhea among under-five children (P<0.05).
|
|
|
|
|
3.2. Discussions of Results
- This study has been an attempt to identify socio-economic, demographic, environmental, and nutrition related determinants of childhood diarrheal morbidity based on Ethiopian Demographic and Health Survey conducted in 2011.This study revealed that the two weeks prevalence of diarrhea among under-five children were about 15.6% in Ethiopia which is consistent with various research [11, 15-17]. Although the significance disappeared in the multivariate analysis, maternal age; sex of child; place of residence; birth order; religion, and toilet facility were significantly associated with the occurrence of diarrhea in the bivariate analysis. This might be due to methodological differences, and time gap between the current and earlier surveys. But further studies are required to confirm these findings.The prevalence of diarrhea in Tigray, Affar, Amhara, Oromya, and Harari were not significantly differing from that in Addis Ababa. Under-five children who live in, Somali, SNNPR, Gambella and Benishangul-Gumuz were more likely to experience diarrhea than children who live in Addis Ababa. This study found that experiencing of diarrhea was significantly associated with age of children. For a unit change in age, the odds of having diarrhea in children were decreased by 2.6%. This finding is in agreement with a study done in Banten Province Indonesia where older children were less likely had chance of having diarrhea than younger children (p-value=0.001) [18]. Children are more vulnerable to diarrhea than adults, because their immune systems are less able to respond to these infections [19].Under-five children whose mothers had work were 12.7% more likely to experience diarrhea than under-five children whose mothers had not work. These findings contradict those found in Egypt where diarrhea was significantly higher among children having mothers with lower education or not working. This might have mothers working status affect length of breastfeeding [20].The study revealed that incidence of diarrhea was significantly associated with durations of breastfeeding. Under-five children who had ever been breast fed but not currently had 44.8% less likely to experience diarrhea as compared to under-five children who had never breasted. Under-five children who still breastfeeding were 36.4% less likely to experience diarrhea as compared to under-five children who never breast fed. This present findings is in agreement with a study done in Ghana, found that infants that were either fully breastfed or mixed-fed (fed both breast milk and other foods or liquids) had a lower incidence of diarrhea than non-breastfed infants [21]. This finding had also conformity with a study done in Bangladesh which showed than infants who were partially or not breastfed had a high risk of diarrhea death than exclusively breastfed infants [22]. Not breastfeeding resulted in high exposure of diarrhea morbidity in comparison to exclusive breastfeeding among infants 0-5 months of age (RR: 10.52) [23]. This might be breastfeeding provides vitamins and nutrients that help children develop important antibodies that reduce diarrheal disease.This study found that incidence of diarrhea was significantly associated with nutritional status of under-five children. The prevalence of diarrhea was higher in stunting under-five children. The odds of having diarrhea in malnourished under-five children were 22.6% higher as compared to under-five children who had no chronic malnutrition. This finding is supported by a study done in Zimbabwe and Bangladesh that showed severely stunted children were more likely to had diarrhea than children of normal height and which had not severe malnutrition [24, 25].Under-five children who were wasting (acute malnutrition) were 49.2% (1.492-1) more likely to experience diarrhea than under-five children who were not wasted. This present findings is in agreement with a study done in Uganda, which showed that Being wasted increases the probability of occurrence of diarrhea as compared to well-nourished counterparts [26]. The study revealed that incidence of diarrhea was significantly associated with underweight. Under-five children who were underweight (have low weight-for age) were 54.8% (1.548-1) more likely to experience diarrhea than children who were not underweighted.
4. Conclusions and Recommendations
4.1. Conclusions
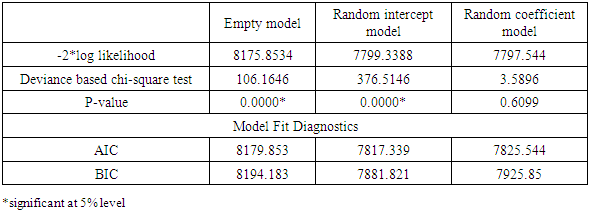
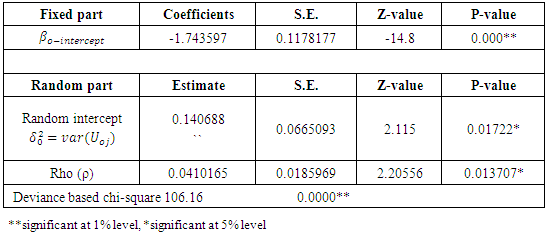
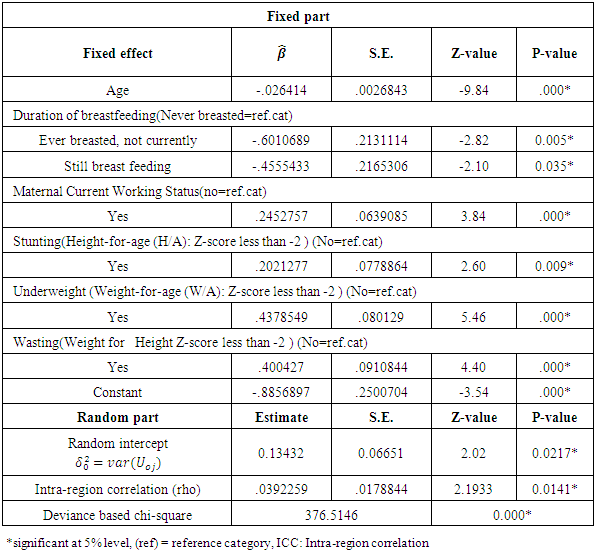
- The purpose of this study has been to identify demographic, socio-economic, environmental and nutrition related determinants and to assess regional variation of incidence of childhood diarrhea in Ethiopia. The descriptive results showed that 15.6% of under-five children have experienced diarrhea in the two weeks prior to the time of survey (EDHS 2011). In this study single level and multilevel logistic regression were used. In the single level logistic regression analysis, age of child, maternal working status, duration of breast feeding, stunting, wasting, and underweight were the most important determinant factors associated with incidence of diarrhea. The incidence of diarrhea was increased with the age of children i.e. the odds of having diarrhea decreased by 2.6% per unit month increment in age of child.In multilevel logistic regression analysis, under-five children are considered as nested within the various regions in Ethiopia. As a first step in the multilevel approach, non-parametric statistical methods were applied to see if there were differences in the prevalence of diarrhea in under-five children among the regions. The non-parametric approach based on the chi-square test suggests that prevalence of diarrhea in under-five children varies among regions. Among the three multilevel logistic regressions models, the random intercept and fixed coefficients model provided the best fit for the data under consideration. It found that the prevalence of childhood diarrhea was varying through regions. The significant determinants for the variations of prevalence of diarrhea among regions were age of child, maternal working status, duration of breast fed, stunting, wasting, and underweight.
4.2. Recommendations
- Based on the findings of this study we forward the following recommendations:× Efforts should be invested to educate parents about the importance of breastfeeding and initiate to adopt the culture of breastfeeding their children to reduce the exposure children to diarrhea.× Efforts should be made to communicate through different programs, such as health and nutritional education, the importance of feeding breast milk and introducing other supplementary nutrient rich foods.× It is useful to develop a policy for mothers to have sufficient time after giving birth and provide formal and qualified job.× Further studies should be conducted to identify other correlates of diarrhea that are not analysed in this study such as hygiene practice and sanitation facilities.