-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2016; 6(3): 91-98
doi:10.5923/j.phr.20160603.03

Factors Associated with Exclusive Breastfeeding Practices among Women in the West Mamprusi District in Northern Ghana: A Cross-Sectional Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkwasi Boakye-Yiadom1, Adadow Yidana2, Napoleon Bellua Sam3, Benjamin Kolog4, Anthony Abotsi4
1School of Allied Health Sciences, Department of Community Health, University for Development Studies, Tamale, Ghana
2School of Medicine and Health Sciences, Department of Community Health and Family Medicine, University for Development Studies, Tamale, Ghana
3Students’ Information System Unit, University for Development Studies, Tamale, Ghana
4School of Allied Health Sciences, Department of Nursing, University for Development Studies, Tamale, Ghana
Correspondence to: Akwasi Boakye-Yiadom, School of Allied Health Sciences, Department of Community Health, University for Development Studies, Tamale, Ghana.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Exclusive breastfeeding promotion is one of the most important health initiatives today. The World Health Organization recommends that all babies and young children are breastfed exclusively for their first six months of life and then given nutritious complementary food with continued breastfeeding up to two years of age. The benefits of exclusive breastfeeding have been espoused by several studies. Despite the education and promotion of exclusive breastfeeding by the Ghana Health Service and other agencies some mothers do not exclusively breastfeed their children for the first six months of life. This study, therefore, sought to investigate the factors that are associated with the practice of exclusive breastfeeding among women in the West Mamprusi district of Ghana. A 15x20 community-based cross sectional study was conducted in the district using simple random sampling in selecting 300 breastfeeding mothers with infants 0-6 months of age. Multistage cluster sampling procedure was used in selecting the study communities. Bivariate and multivariate analyses were done to find the determinants of exclusive breastfeeding in the study sample. Results indicated the prevalence of exclusive breastfeeding was 84.3%. Factors that were associated with exclusive breastfeeding were household wealth index (P<0.001, OR=12.3, 95%, CI: 35.43-36.7), antenatal care attendance (P<0.001, OR=10.44, 95%, CI: 32.42-37.21), knowledge of exclusive breastfeeding (P<0.002, OR=7.43, 95%, CI: 0.69-4.54) and place of delivery (P<0.006, OR=12.52, 95%, CI: 12.52-13.56). It emerged thatmajority of the women practised exclusive breastfeeding. Educational level of mothers did not have any influence on the practice of exclusive breastfeeding and was not significantly associated with the practice of exclusive breastfeeding. Antenatal care attendance on the other hand had a significant influence on the practice of exclusive feeding. The study recommends that information and education on exclusive breastfeeding among women not attending ANC and those who do not deliver in a facility be intensified in the entire district.
Keywords: Breastfeeding, Exclusive breastfeeding and infant feeding, Colostrum, Walewale
Cite this paper: Akwasi Boakye-Yiadom, Adadow Yidana, Napoleon Bellua Sam, Benjamin Kolog, Anthony Abotsi, Factors Associated with Exclusive Breastfeeding Practices among Women in the West Mamprusi District in Northern Ghana: A Cross-Sectional Study, Public Health Research, Vol. 6 No. 3, 2016, pp. 91-98. doi: 10.5923/j.phr.20160603.03.
Article Outline
1. Background
- It has been estimated that 1.3 million deaths could be prevented each year if babies were exclusively breastfed from birth to six months [2]. Since 1979, the World Health Organization (WHO) recommended that children should be exclusively breastfed between “4-6 months” after birth. This was changed to 6 months in 2001, following a review and evaluation of more than 3,000 references by its Secretariat, which supported the recommendation [1]. The reason for the review was that World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) recommended that all mothers should breastfeed their children exclusively for the first 6months and thereafter they should continue to breastfeed for as long as the mother and child wish, and both appropriate and sufficient weaning food should be added after six months of life [1, 2]. WHO estimates that worldwide only 35% of children between birth and their fifth month are breastfed exclusively [1, 31].Exclusive breastfeeding (EBF) has been defined by WHO as the situation where ‘the infant has received only breast milk from his or her mother or a wet nurse, or expressed breast milk and no other liquids or solids, with the exception of drops or syrups consisting of vitamins, minerals supplements, or medicines [8]. Several studies conducted in other countries have shown that exclusive breastfeeding for the first half year plays a significant role in preventing morbidity and mortality among infants. In a study by [13], the predictors of exclusive breastfeeding that were considered were socio-economic factors such as maternal years of education, total household income and place of residence and demographic factors.In another study in exclusive breastfeeding in Kenya by [14] they asserted that among lactating mothers with infants zero to six months, exclusive breastfeeding practice (33%) was considered low and this posed a great concern. The authors also established that marital status, employment, maternal education, place of delivery and both infant and mothers' age were closely associated with knowledge and practice of exclusive breastfeeding. According to [15], in a study in Nigeria to determine the knowledge of mothers about exclusive breastfeeding it was reported that 33% of mothers believed that giving baby water once in a while meant exclusive breastfeeding and recommended intensive health education campaign aimed at educating lactating mothers on the need to practice exclusive breastfeeding.A study by [16] in Ethiopia, on factors associated with exclusive breastfeeding practices, they reported that prevalence of exclusive breastfeeding among respondents was 73 percent, however, the study did not assess individual factors such as knowledge and other variables such as wealth index and these are some of the variables that this study in West Mamprusi looked at.The 2008 Ghana Demographic Health Survey (GDHS) reported that overall, 98 percent of children born in the past five years in Ghana (preceding the survey) had been breastfed at some time. For last-born children ever breastfed, 52 percent started breastfeeding within one hour of birth and 82 percent started breastfeeding within the first 24 hours after delivery. While there was a high percentage of early initiation of breastfeeding, and an extended length of breastfeeding time in Ghana, some mothers failed to carry the practice through the recommended six months; for instance, 84 percent of children under two months of age were exclusively breastfed; by age 4-5 months, only 49 percent were still being exclusively breastfed.Despite the numerous benefits of exclusive breastfeeding, to both mothers and their infants, some women in the West Mamprusi district continued to use animal milk and formula feeds to feed their infants because of inadequate milk supply which eventually affected the health and nutritional needs of the children. The effect of these inappropriate infant feeding practices was evident in the rising level of infectious diseases (such as pneumonia, diarrhoea), anaemia and child morbidity and mortality [4].The percentage of women who breastfed their children exclusively in 2013 decreased from (3231; 82.6%) to (2469; 64.8%) in 2014 [5]. In that same period the incidence of diarrheal cases among infants below six months rose from (476) in 2013 to (1601) in 2014. This was blamed largely on the shortages of drugs used for the Integrated Management of Childhood Illness (IMCI) and inappropriate infant feeding practices among mothers in the district. Meanwhile, exclusive breastfeeding in the Northern region was reported to be 63.6 percent according to the Multiple Indicator Cluster Survey conducted by UNICEF in 2011. West Mamprusi is a district in the Northern region of Ghana and no study has been conducted to document the magnitude and other related factors on exclusive breastfeeding. This study therefore sought to find the factors that were associated with the practice of exclusive breastfeeding among lactating mothers in the West Mamprusi district of Northern Ghana.
2. Methods
2.1. Study Area and Study Population
- The West Mamprusi district is one of the 26 administrative districts of the Northern region of Ghana. The district health directorate is administratively divided into five (5) sub-districts; Walewale, Janga, Kpasenkpe, Kubori and Yikpabongo sub-districts. The district has one hospital, one polyclinic, three health centres, six clinics and four Community Based Health Planning and Services (CHPS compounds). As at the time of the study, there were 212 communities with a total population of one hundred and fifty nine thousand, one hundred and eighty two people (159,182) [5].A 15x20, thus, (15 respondents each from 20 communities) community based cross-sectional study was conducted in the West Mamprusi district. The communities or clusters were selected from the sampling frame with probability proportional to size (PPS). Quantitative methods were used in the data collection. A sample size of 300 breastfeeding mothers was used based on the standard formula for one point sample estimation. The primary outcome variable used to estimate the sample size was the population proportion of exclusive breastfeeding in the district which was 27.6% in 2011 a 95% confidence level and 5% margin of error were used in the analysis. Structured questionnaire on exclusive breastfeeding was used to interview 300 mothers whilst 10 women leaders of the mother-to-mother support groups in the communities referred to as “Magazias” served as key informants. The Ghana Health Service encourages all communities to form mother-to- mother groups in order to meet and discuss maternal health issues. These support groups are also used by the service for advocacy on new interventions.
2.2. Inclusion Criteria
- The inclusion criteria were women in their seventh month after delivery residing in the West Mamprusi district. Any woman who delivered in less than seven months or more than seven months was not included in the study. This was to help reduce recall bias and to help measure the prevalence rate of practice of EBF for 6 months. Participation rate was 100%. All the respondents who were targeted participated in the study. Data collection was done from February, 2014 to June, 2014.
2.3. Variables and Measurements
- Structured closed-ended questionnaires were used to collect quantitative data which were administered in the local language of the respondents. Data were collected on the socio-demographic characteristics of the women, household wealth index, infant feeding practices, cultural practices and beliefs, and knowledge and practice of exclusive breastfeeding. The prevalence of exclusive breastfeeding in this study was calculated based on the proportion of women in the study sample who breastfed their children with breast milk for the first 6 months of life. A household wealth index based on household assets and housing quality was used as a proxy indicator for socio-economic status (SES) of households. An absolute measure of household wealth (wealth index) used in this study was based on an earlier concept developed by [6], whereby the sum of dummy variables created from information collected on housing quality (floor, walls, and roof material), availability of electricity, water and type of toilet facility, and ownership of household durable goods and livestock (e.g. bicycle, television, radio, motorcycle, sewing machine, telephone, cars, refrigerator, mattress and bed) were used to determine the household wealth index. These facilities or durable goods were regarded as modern goods that had been shown to reflect household wealth in the study area. A household of zero index score for example, means that household had not a single modern good. The scores were thus added up to give the proxy household wealth index. The index varied from 0-18. Households that had a wealth index score of 13 and below were classified as having a low wealth index score and those that had a wealth index score of 14 and above were classified as having a high wealth index score. These were arbitrarily established for the purpose of the study. The main aim of creating the index was to categorize households into SES groupings in order to establish its effect on the practice of exclusive breastfeeding. Knowledge of exclusive breastfeeding was also assessed using proxies such as respondents’ knowledge of the benefits of exclusive breastfeeding, period of exclusive breastfeeding, dangers of not breastfeeding exclusively and composition of breastmilk.
2.4. Data Analysis
- Quantitative data were coded and entered into SPSS version 18.0. Bivariate and multivariate analyses were done to find the factors associated with exclusive breastfeeding. P-values and Chi square values were used to test associations. P-values less than 0.05 were considered statistically significant. Qualitative data were transcribed into English before thematic analysis was done. There was informed consent from all the respondents before they were interviewed.
3. Results
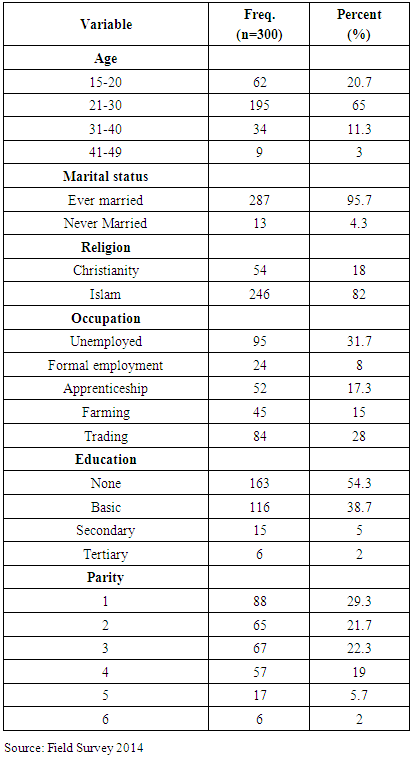
- The mean age of the respondents was 24±3.6 with majority, thus 195 (65%) of them within the age group of 21-30. Moslems were in the majority 246 (82%) whilst Christians formed the minority group 54 (18%). Only 6(2%) of the women were educated to the tertiary level with majority of them representing 163 (54.3%) having no formal education. The majority of the respondents were within the age group of 21-30 representing 195 (65%) as shown in Table 1.The study revealed that one out of every three respondents was unemployed whilst nearly, one out of thirteen respondents was having formal employment. Table 1
|
|
|
|
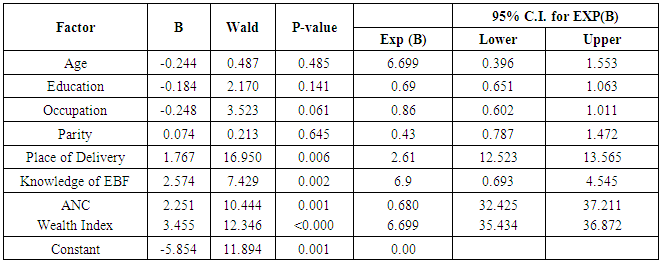
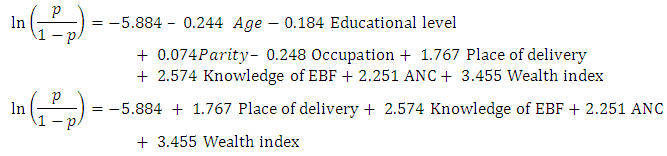 Probability PredictionUsing a respondent with High Knowledge of EBF=1, Gave birth at Government facility =1, Attending ANC=1 and High wealth index=1. The probability of exclusive breastfeeding among women in West Mamprusi District given the above characteristics.
Probability PredictionUsing a respondent with High Knowledge of EBF=1, Gave birth at Government facility =1, Attending ANC=1 and High wealth index=1. The probability of exclusive breastfeeding among women in West Mamprusi District given the above characteristics.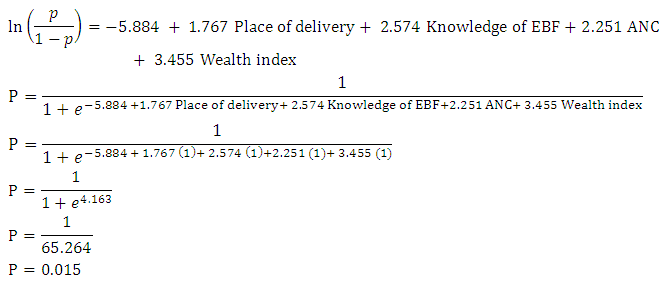 This indicates that there is probability that 1.5% of women, with the given characteristics are likely to be practicing exclusive breastfeeding.
This indicates that there is probability that 1.5% of women, with the given characteristics are likely to be practicing exclusive breastfeeding.4. Discussion
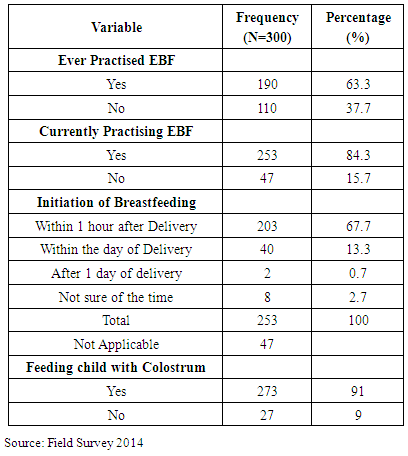
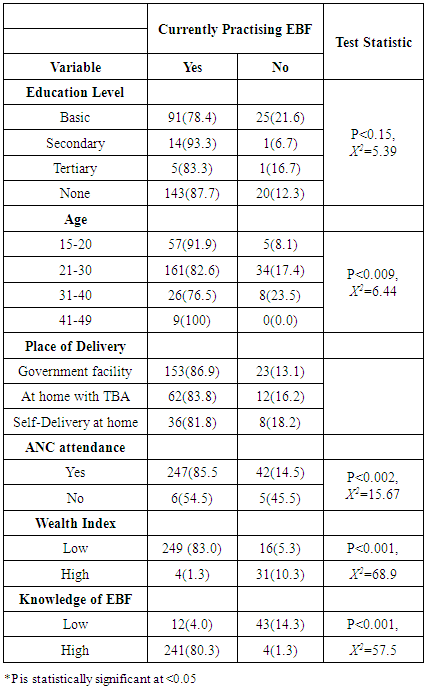
- The general objective of this study was to find the factors that were associated with the practice of exclusive breastfeeding among women in the West Mamprusi district of Ghana. Women without any formal education in the study sample formed the majority, thus, 54.3% of the study sample which is in consonance with the findings of the Ghana Statistical Service [17] that formal education among females is only 38% whilst 62% of females in the West Mamprusi district do not any level of formal education. Also the 2% of women in the study sample who were educated to the tertiary level was lower than the 4% reported by the 2008 Demographic and Health Survey. Female education has been associated to the use of maternal and child health services. A study by [18, 19] and [20] reported that women with higher level of formal education are more likely to use maternal health services. In this present study, infant feeding practices such as exclusive breastfeeding had no significant relationship with the educational level of the mother. This corroborates the findings of [23] that maternal educational attainment was unrelated to good neonatal feeding and infant feeding practices.However, the findings contradict or disagree with the findings of [7-9], in Nigeria, [22] in India, [23] [in Brazil and [1] in Ghana and Nigeria [32] who reported that the level of educational attainment of mothers was positively correlated to the practice of exclusive breastfeeding because educated women followed the antenatal instructions to the letter, thereby changing their attitudes towards utilization of exclusive breastfeeding. The finding of this current study could be attributed to the fact that exclusive breastfeeding is now universally known due to the education provided during ANC visits and it is, therefore, not the preserve of only educated women. In this study area, the presence and activities of the mother-to- mother support groups could have influenced the practice of EBF. The groups are made of mothers with different levels of formal education and they receive the same messages. The fact that educational attainment was not a determinant of the practice of EBF does not preclude the fact that education still remains the most viable means of reaching everybody with the benefits of exclusive breastfeeding. About 67.7% of the women in the study sample initiated breastfeeding within the first hour after delivery which is higher than the findings of the 2008 GDHS and the Multiple Indicator Cluster Survey (MICS) (2011) which found that mothers who breastfed their children within the first hour of delivery in Ghana were 46% in both surveys. This could be attributed to the smaller sample size involved in this study compared to the two surveys. The finding was, however, lower than the 73.5% of women who were reported to have initiated breastfeeding within the first hour after delivery in the Kumbungu district in northern Ghana [21].The prevalence of exclusive breastfeeding in the study population was 84.3% which was higher than the 63% reported by the Ghana Health Service and Ghana Statistical Service [4] prevalence of exclusive breastfeeding in the study area was also found to be higher than the 46% established [1] Compared to the practice of EBF in some rural communities in the Osun State of Nigeria which was found to be 20% as reported by [24], the current study showed that majority of mothers of West Mamprusi district practiced exclusive breastfeeding for the first 6 months after delivery. The high rate of EBF practice could be attributed to the mother-to-mother support groups that have been funded by non-governmental organizations and also the education from nurses at the Reproductive and Child Health Centers of the Ghana Health Service where pregnant women receive antenatal care services. Bivariate and multiple logistic regression analyses showed that household wealth index was a significant factor associated with the practice of exclusive breastfeeding which is similar to the earlier findings by [3] and [1]. The finding that household wealth index was positively associated with the practice of EBF also corroborates that of [24] in Osun State in Nigeria and [25] of South-Western Nigeria who established that mothers from households with lower income least practiced EBF than mothers from households with high wealth index. The association is attributable to abject poverty because of their low level of income. This finding corroborates the work of [25] in Nigeria.Knowledge of exclusive breastfeeding was also found to be positively associated with the practice of exclusive breastfeeding which confirmed the importance of mother's breast-feeding knowledge and the practice of exclusive breastfeeding [26, 27].The positive correlation between maternal exclusive breastfeeding knowledge and their practice of exclusive breastfeeding was also established by [28] in Canada where it was discovered that mother’s knowledge about EBF is as good as having the practice done. Similar findings were made by [29] on the knowledge of mothers on EBF which highlighted mother’s good knowledge on EBF as the major ingredient in the successful practice of EBF.The study also found that seeking antenatal or prenatal care is significantly associated with the practice of exclusive breastfeeding. This confirms the findings of [12] in Tanzania that women who made at least 4 ANC visits were more likely to practice exclusive breastfeeding compared to their counterparts who made less than 4 ANC visits during their pregnancy. This finding also supports that of [21] who reported that 64% of women who initiated ANC in the first trimester and also made the minimum of 4 ANC visits practiced EBF in rural communities of northern Ghana. This finding could be attributed to the education on breastfeeding that is given to pregnant women who seek antenatal care in health facilities.It was also very intriguing to find that the place of delivery is positively associated with the practice of exclusive breastfeeding in the study sample. Women who sought skilled delivery services were found to practice exclusive breastfeeding compared to those who delivered at home.
5. Conclusions
- Majority of the women practiced exclusive breastfeeding. Education level of women was found not have any influence on the practice of exclusive breastfeeding. However, antenatal care attendance and place of delivery had significant influence on the practice of exclusive feeding. It is, therefore, recommended that information and education on exclusive breastfeeding among women not attending ANC and those who do not deliver in a facility be intensified in the entire district. The mother-to-mother support groups should also be adequately supported to intensify their activities in order to bring in more mothers to help educate them on the need for exclusive breastfeeding.
ACKNOWLEDGEMENTS
- We acknowledge the cooperation of the West Mamprusi District Health Directorate and health facilities in the district and also thank the respondents for their participation in the study.