-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2016; 6(2): 69-75
doi:10.5923/j.phr.20160602.07

Socio-Demographic Factors Influencing Nutritional Status of Children (6-59 Months) in Obunga Slums, Kisumu City, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML1Department of Nutrition and Health, Maseno University, Maseno Township, Kenya
2Institute of Health Public Health and Management, International Health Sciences University, Kampala, Uganda
Correspondence to: Omondi D. O., Department of Nutrition and Health, Maseno University, Maseno Township, Kenya.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Poor nutrition remains a direct critical factor in child mortality in Africa. A lot of focus has been given to the rural population as poverty setting. However, urban slums display more serious poverty conditions which manifest in poor stunting rates, yet this has been ignored in the realm of scientific writing. This study explored the socio-demographic factors in relation to nutritional status indices mainly stunting, wasting and underweight. Materials and Methods: The study was conducted within Urban Slums using cross-sectional analytical design using a sample of 400 eligible households from total eligible households within the slum. Data was collected using structured questions and analysis done using descriptive and inferential statistics mainly odds ratio. Results: The results show strong association between income and stunting (OR=0.47; CI=0.24-0.91) and underweight (OR=0.44; CI=0.22-0.92). Wasting was strongly associated with Age of the mother (OR=1.07; CI=1.01-1.33) and mother’s education (OR=0.34; CI=0.14-0.83). Religion and sex of the child were ruled out based on the analysis outcome. Conclusions: These results may explain social perspective of nutritional status and suggest two critical factors that interventions should give much attention in order to ensure well being. Income, mother’s age and mother’s education are very critical in child health interventions. However, there is need to continue establishing new perspective of social components within similar settings beyond the boundary of Obunga.
Keywords: Socio-Demographic, Nutritional status, Children, Slums
Cite this paper: Omondi D. O., Kirabira P., Socio-Demographic Factors Influencing Nutritional Status of Children (6-59 Months) in Obunga Slums, Kisumu City, Kenya, Public Health Research, Vol. 6 No. 2, 2016, pp. 69-75. doi: 10.5923/j.phr.20160602.07.
1. Introduction
- Malnutrition characterized by stunting, wasting and underweight is a major burden associated with children under five years worldwide and about one-third of the world children population seems to be malnourished [1]. Half of the 200 million deaths among children less than five years in developing countries were attributed to malnutrition a decade ago making it an immediate predictor of child mortality [2]. However this condition continues to be an important Public Health problem in sub-Saharan Africa and a concern in urban slum dwellings. Some socio-demographic factors such as Age of the mother/surrogate mother, Income level, Religion Literacy level, Maternal Level of education, Sex of the child could influence nutritional status of a child but may display different scenarios in urban setting due to unique and unpredictable urban slum environment. A study conducted by Islam et al. [3] revealed significant relationship between socio-economic status and literacy of parents on prevalence of height-for-age (HAZ), weight-for-height (WHZ) and weight-for-age (WAZ). In this cycle socio-economic status focused on income levels while literacy was focused on whether parents could read and write. Low income and maternal literacy was also recently identified as key factors determining HAZ, WHZ and WAZ [5]. However, this study covered a wide geographical area raising a gap as to whether a similar pattern would be displayed in more specific closed urban slum settings.There seems to be a strong linkage between maternal level of education and nutritional status. Maternal level of education has been found to be associated with nutritional status of children in Kenya [6] [7]. Direct knowledge transfer to mother’s literacy and numeracy skills acquired from formal education enhance ability of caregiver to recognize illness and take appropriate action [8] in relation to child well being. It appears that there is demonstration on how maternal education may influence nutritional status of children even though gaps exist on the direct linkage within malnutrition pattern. Upon this background literature it was interesting to determine the linkage that level of education had with nutritional status of children (6-59 moths) within an urban slum setting. Religious affiliation of a household and level of education of the mother has strong linkage with nutritional status of children under five years [9]. Religious attribution has strong influence on food consumption pattern and indirect to influence nutritional status as some religious doctrines restricts consumption of certain foods. Gender/sex inequalities have received research focus with regard to effect on nutritional status [10] [11]. There seems to be conflicting information as to whether girls and boys would show differences in nutritional status within a similar setting [12-14]. It is expected that an ideal situation would show similarities on nutritional status indictors between boys and girls in a similar setting if many factors in the etiology were held constant. In this case external influence would focus on both sexes. However, this is a strong assumption that required some significant empirical proof. In poverty stricken urban setting, it would be apparent that differences attributed to value attached to gender of a child would be noticed in a study. This paper focuses on influence of level of income, sex of the child, religious affiliation, age of the mother or surrogate mother, maternal level of education and literacy level on nutritional status within a fast growing urban slum setting in Kisumu City, Kenya. Many studies seem to focus on general rural population with a few urban studies in exploration of the etiological complexities of nutritional status. This indicates limited focus on unique settings of public health concern where urban informal settlements become an ignored risk settings. This was a major gap that this study intended to fix and made clear for the purpose of scholarly comparisons. Based on this background this paper explored the selected social-demographic determinants of nutritional status of children under five within Obunga Informal settlement in Kisumu County.
2. Materials and Methods
- The study adopted a cross-sectional analytical design. Data was collected within a period of one and analyzed once for the period. This study design was chosen because it does not allow for any manipulation of factors and provides population characteristics as they at one point in time. The study unit consisted of 4000 eligible households listed in Obunga Informal settlement. An eligible household was made up on all children between 6-59 months with their maternal caregiver in Obunga informal settlement. The children were studied by assessing their nutritional status. This was followed by interviewing a biological mother or surrogate mother during the study. The sampling unit therefore included an eligible mother plus child within 6-59 months in a household. A household listing (sampling frame) based on the specified inclusion and exclusion criteria was developed and a representative sample size determined. Any household with a mother or child who did not consent to participate in the study was excluded.Sample size was determined according to Fisher et al (1991), using the formula;
 Where: n = minimum sample size (for population >10,000) required.Z = the standard normal deviate at the required confidence level, (set at 1.96 corresponding to 95%, Confidence level adopted for this study).p = population proportion estimated to be stunted in Obunga, which now stands at 41% (Kisumu Medical Education Training, 2011). q = 1-pd = the degree of accuracy required (was be set at 0.05 if prevalence of malnutrition is not known otherwise the actual prevalence will be used).Therefore, on substitution:
Where: n = minimum sample size (for population >10,000) required.Z = the standard normal deviate at the required confidence level, (set at 1.96 corresponding to 95%, Confidence level adopted for this study).p = population proportion estimated to be stunted in Obunga, which now stands at 41% (Kisumu Medical Education Training, 2011). q = 1-pd = the degree of accuracy required (was be set at 0.05 if prevalence of malnutrition is not known otherwise the actual prevalence will be used).Therefore, on substitution:  However, since the targeted population was 4000 eligible households the final sample size (nf) was adjusted as follows:
However, since the targeted population was 4000 eligible households the final sample size (nf) was adjusted as follows: Where; n f = desired sample size (when target population is less than 10,000) n = desired sample size (when target population is greater than 10,000) N = the desired sample size (target population) nf = 4000 ÷ {1+ (4000/372)}=340.42≈ 341 (plus 20% expected non-response) Sampling procedure followed a systematic random technique where the first household was chosen by simple random methods than every 10th Household in the listing was selected to participate. Out of 409 HHs only 400HH finally participated in the study after every HH was given equal chance of participating in the study. Dependent variable was child nutritional status. This was operationalized as Anthropometric indices categorized as Height for age z-score (HAZ), Weight for Age z-score (WHZ) and Weight for Height z-score (WAZ). Independent underlying variables focused on socio-demographic characteristics and were considered as potential moderators in the relationship. This category of variables included socio- age of the mother, education level of the mother, income level, literacy level of the mother and religion.Anthropometric Measurement of child’s height and weight were taken. Calibrated Short height-length measuring boards were used to take measurements of children’s height. Each child’s height was measured twice to the nearest 0.1 cm and measurements were repeated if there was a deviation of >±0.5 cm. Weight was measured to the nearest 0.1g using digital Seca Model 881 Scale. Z scores for height for age, weight for age, and weight for height were generated using Ena for SMART software based on WHO’s standard. Children wore light clothes and weights were adjusted for this to avoid errors created by the extra weight of the clothes. Other measurements of indicators of socio-demographic factors were done based on literature and previous measurement principles and criteria. Analysis adopted use of descriptive and inferential statistics. Inferential statistics adopted linear regression to establish the relationship between nutritional status and the independent variables which were measures of social demographic factors. Use of linear regression was to determine the predictive model nutritional status and effective isolation of predictive factors within socio-demographic domain. Logistic regression with crude and adjusted odds ratios were used to test for the strength and direction of the association. The association between socio-demographic factors and nutritional status indices were coded into dichotomous binary where 2-score >-1 was coded as “0” and 2-score <1 was coded as “1’ code “0” was “normal” while code “1” was stunting, wasted or underweight in pattern.
Where; n f = desired sample size (when target population is less than 10,000) n = desired sample size (when target population is greater than 10,000) N = the desired sample size (target population) nf = 4000 ÷ {1+ (4000/372)}=340.42≈ 341 (plus 20% expected non-response) Sampling procedure followed a systematic random technique where the first household was chosen by simple random methods than every 10th Household in the listing was selected to participate. Out of 409 HHs only 400HH finally participated in the study after every HH was given equal chance of participating in the study. Dependent variable was child nutritional status. This was operationalized as Anthropometric indices categorized as Height for age z-score (HAZ), Weight for Age z-score (WHZ) and Weight for Height z-score (WAZ). Independent underlying variables focused on socio-demographic characteristics and were considered as potential moderators in the relationship. This category of variables included socio- age of the mother, education level of the mother, income level, literacy level of the mother and religion.Anthropometric Measurement of child’s height and weight were taken. Calibrated Short height-length measuring boards were used to take measurements of children’s height. Each child’s height was measured twice to the nearest 0.1 cm and measurements were repeated if there was a deviation of >±0.5 cm. Weight was measured to the nearest 0.1g using digital Seca Model 881 Scale. Z scores for height for age, weight for age, and weight for height were generated using Ena for SMART software based on WHO’s standard. Children wore light clothes and weights were adjusted for this to avoid errors created by the extra weight of the clothes. Other measurements of indicators of socio-demographic factors were done based on literature and previous measurement principles and criteria. Analysis adopted use of descriptive and inferential statistics. Inferential statistics adopted linear regression to establish the relationship between nutritional status and the independent variables which were measures of social demographic factors. Use of linear regression was to determine the predictive model nutritional status and effective isolation of predictive factors within socio-demographic domain. Logistic regression with crude and adjusted odds ratios were used to test for the strength and direction of the association. The association between socio-demographic factors and nutritional status indices were coded into dichotomous binary where 2-score >-1 was coded as “0” and 2-score <1 was coded as “1’ code “0” was “normal” while code “1” was stunting, wasted or underweight in pattern.3. Results
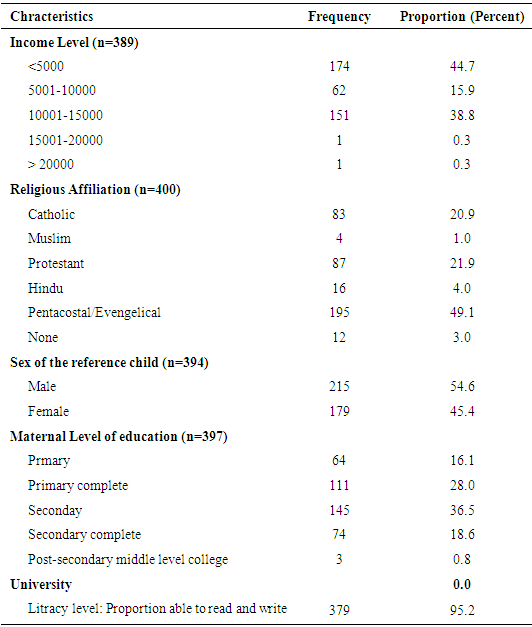
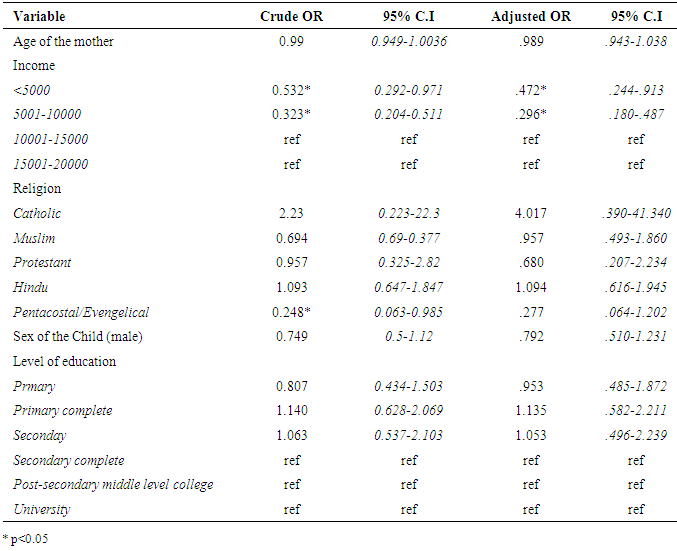
- The study focused on socio-demographic factors of eligible households. Among the factors considered for consideration were; income level, religious affiliation, sex of reference child, level of education of caregivers, and literacy level. Income pattern revealed that majority of households earned less than Ksh 5000 (44.7%) followed by those who earned between Ksh 10001–15000 (38.8%). Some reasonable proportions earned between Ksh 5000 – 10000 (15.9%). Generally, household level of earning was less than Ksh 15000. The findings further revealed that majority of households were Pentecostals origin (49.1%), followed by protestant (21.9%) and catholic (20.9%). Muslims (1.0%) and Hindu (4%) scored the least. Within sex of reference child, 54.6% of children were males while 45.4% were females. There was no significant difference recorded between male child participant and female child participants (z=1.818, p=0.069, Confidence Interval (CI) = -0.0071: 0.1912). Majority of the caregivers reached secondary school level of education (36.5%) and primary level (28.0%) in that order. Only 18.6% completed secondary level of education. Literacy level was high among the caregivers (95.2%).Table 2 shows the relationships that emerged between socio-demographic factors with stunting based on binary logistic regression analysis. Both bivariate and multivariate logistic regressions were conducted establishing the crude and adjusted odds ratio at 95% C.I.
|
|
|
|
4. Discussion
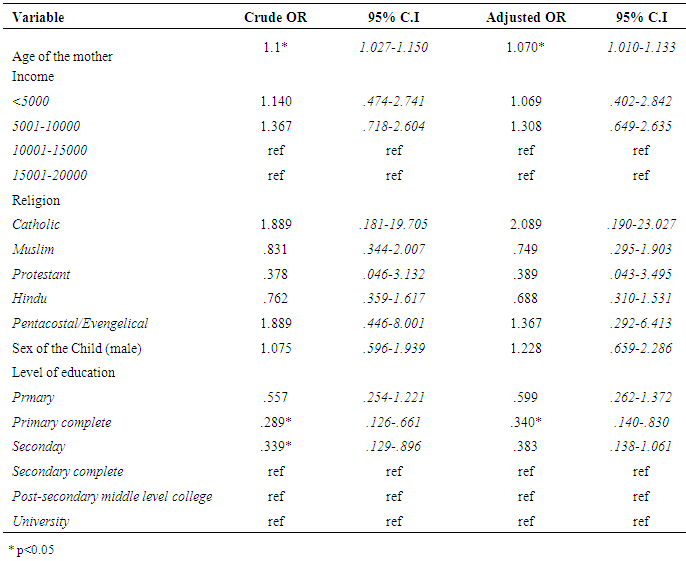
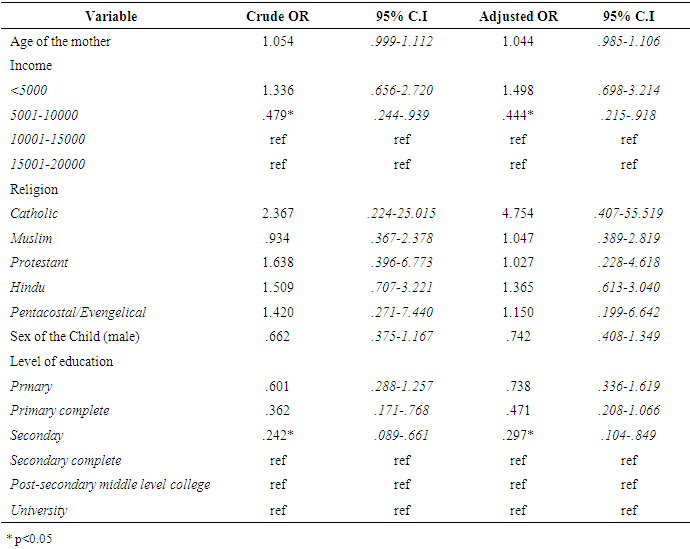
- These results revealed significant association of income with HAZ, WHZ and WAZ of children under five years. In this context income could significantly influenced household purchasing, food production power and household food accesses which are direct predictors of nutritional status. Low income has been identified as a key factor determining HAZ, WHZ and WAZ [5]. It is associated with growth retardation leading to achievements in growth below the potential [15] Household income stands out a key proxy predictor of nutritional status which means it has underlying mediators. Establishing causal association between nutritional status and income may not be possible based on cross sectional analysis approach. A study with some similarities examined the relative effect of fathers’ and mothers’ income of children’s nutritional status and revealed that household income component associated with the mothers had strong benefit to the child’s nutritional status within a peri-urban environment [16] Even though this relationship was examined over a decade ago, it appears that pooled income would improve nutritional status even in the current urban situation. It emerged that level of education may have no effect on stunting but significant partial effect on wasting and underweight. This finding seems to contradict the findings of other where there seems to be a strong linkage between maternal education and nutritional status of children in Kenya [6] [7]. While direct knowledge transfer to mother’s literacy and numeracy skills acquired from formal education enhance ability of caregiver to recognize illness and take appropriate action for example seeking appropriate treatment [8] this appears to be the opposite among households within Obunga slums. However, the study somehow revealed some associations between level of education, wasting and underweight which confirms the linkage previously alluded to by a number of authors. In an interactive linear regression model, mothers attaining higher levels of education exhibited an unexpected negative association with nutritional status indices [17]. This outcome demonstrates mixed results and somehow suggests that education could lead to mother engaging in other activities hence offering little attention to child care. Critically examined, it appears that the relationship between maternal education and nutritional status could be rather situational based and very unpredictable. The findings of this study further revealed that the concept of religion has no significant association with WAZ and WHZ except for WAZ which had some mild association with Pentecostal church where membership to this denomination would decrease chances of stunting. This would imply that being in any kind of religious groups may not have any direct implication of nutritional status of children under five. However, religious affiliation of a household has previously had a strong influence on food consumption pattern which may indirectly influence nutritional status [9]. This concept therefore may not be ignored in the etiological pattern of determinants of nutritional status. Sex of a child had no association with nutritional status indices. The study revealed that whether a child is male or female nutritional status would remain the same when other factors are held constant. The outcome of this study joins the debate of many authors where gender/sex as possible direct or proxy determinant of nutritional status receives conflicting information. In some situations gender is ruled out completely while in other situation it has proved as a key factor in nutritional status etiology [10-14]. Somehow this study attest to the fact that real social determinants would focus on external factors within rather than intrinsic factors linked to sex differences. In conclusion, this study has made an attempt to explore socio-demographic factors that may influence nutritional status within urban slum setting typical of Obunga informal settlement in Kisumu Kenya. Factors in the mix which have been ruled out as associates’ variables to stunting, wasting and underweight include religion and sex of the child. Household income was significantly associated with stunting and underweight. Age of the mother and mother’s education level was associated with wasting. These results may explain social perspective of nutritional status and suggest three critical factors that interventions should give much attention in order to ensure well being. Income, mother’s age and mother’s education are very critical in child health interventions. However, there is need to continue establishing new perspective of social components within similar settings beyond the boundary of Obunga.