Adadow Yidana1, Akwasi Boakye-Yiadom2, Millicent Osei3
1School of Medicine and Health Sciences, Department of Community Health and Family Medicine, University for Development Studies, Tamale, Ghana
2School of Allied Health Science, Department of Community Health, University for Development studies, Tamale, Ghana
3School of Allied Health Sciences, Department of Nursing, University for Development Studies, Tamale, Ghana
Correspondence to: Adadow Yidana, School of Medicine and Health Sciences, Department of Community Health and Family Medicine, University for Development Studies, Tamale, Ghana.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
A recent development on the use of tobacco shows that its usage is on the ascendancy in developing nations with its associated socio-economic and health implication. Using both qualitative and quantitative methods, a purposive sampling technique, a total of 384 respondents were selected to elicit their views on factors that influence tobacco use and how it impacts the health and social wellbeing of men in northern Ghana. The data was analyzed using statistical package for social sciences for the quantitative data and content analysis for the qualitative data. The findings showed that most of the respondents were still actively smoking. More so, a number of respondents were introduced into the act of smoking by friends. The average number of sticks smoked was 18 per week. It also emerged that while some smoke to reduce shyness, others smoke to reduce stress. It was also revealed that though many are aware of the health hazards associated with smoking, they seem not to know the health hazards associated with passive smoking. The paper thus recommends that proper education should be given to children as well as adults who are currently smoking about the potential health risk associated with smoking.
Keywords:
Tobacco, Legislation, Male Adults, Smoking Habit, Socio-Economic
Cite this paper: Adadow Yidana, Akwasi Boakye-Yiadom, Millicent Osei, Tobacco Use and Its Socio-Cultural Dimension among Male Adults in Northern Ghana, Public Health Research, Vol. 6 No. 2, 2016, pp. 64-68. doi: 10.5923/j.phr.20160602.06.
1. Background
The use of tobacco in low and middle income countries is on the ascendency [1]. Whereas tobacco use appears to be declining in many developed countries, it is increasing in the developing world [2]. Research show that the use of tobacco is associated with ill health, yet many Africans are not aware of the negative health effects associated with smoking [3]. This limited knowledge has serious implications in view of the fact that tobacco’s future victims are today’s children. This argument is premised on the fact that tobacco use is initiated at childhood and continues through adolescence to adulthood. High smoking prevalence among men is often linked to high level of second-hand smoke exposure among non-smoking persons living in the same dwelling with smokers [4]. In the opinion of [5], manufactured cigarettes are the most commonly used form of tobacco, though others grow what they use. The different use to which tobacco is put often determines the socio-economic and health risk they may be exposed to.In whatever form tobacco is used, it has been observed that socio-cultural factors have a role in the smoking habit of older people. A greater part of behaviour associated with smoking are often ritualized socio-culturally [6]. This ritualization forms part of many ceremonies especially in parts of the developing world [7]. Realizing their predicaments, some of the addicted persons often strive to stop smoking. However, these struggles are often not successful because they do not seek smoking cessation support from experts [8]. To minimize the socio-economic and health effects of tobacco use, many countries have promulgated laws against tobacco use in public places [3]. In a developing country like Ghana, frantic efforts are made by the Ghana Health Service in the fight against tobacco smoking [4]. These efforts notwithstanding, tobacco use is still contributing substantially to mortality and morbidity, and surprisingly, there is an increase in the use of tobacco in Ghanaian schools. This has raised concerns among stake holders on ways and means of halting the consumption of tobacco to prevent people from dying from tobacco related illness. This study thus examines factors influencing the use of tobacco and how it impacts the social wellbeing of men in the Yendi municipality in Northern Ghana.
2. Methodology
Between August and September 2014, 384 tobacco smokers were purposively selected and interviewed in relation to the social and health impact of smoking. Only those who agreed to be interviewed were interviewed. The aim of the study was clearly explained to the participants and they were aware that their participation in the study was voluntary. Four focus group discussions were also organized for additional information. The study was cross sectional design carried out in Yendi Municipality in the Northern Region of Ghana. The tools used for the data collection were structured questionnaire and focused group discussion guide. The questionnaire was pretested and validated in a community that did not form part of the study area. Additional tools were a tape recorder and a jotter to record the proceedings of the discussions. Since majority of people in Yendi could speak both English language and Dagbani, all of which are languages the researchers speak, the research was conducted using these languages. Two research assistants were recruited to help in recording the discussions while the lead investigators were facilitating the discussion sessions. The focus group discussions were transcribed for analysis. This study was approved by the Research Ethics Committee of the University for Development Studies, Tamale Ghana and all participants were assured of anonymity and confidentiality.
3. Results and Discussion
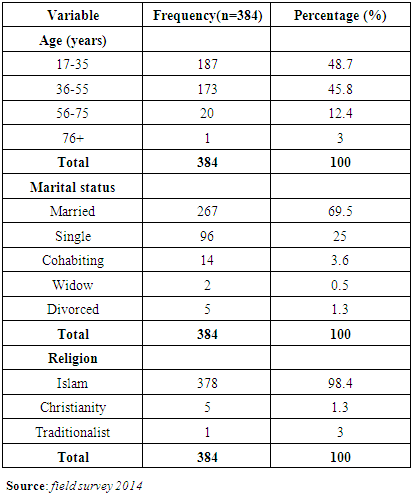
Socio Demographic CharacteristicsTable 1. Socio Demographic Characteristics of respondents
 |
| |
|
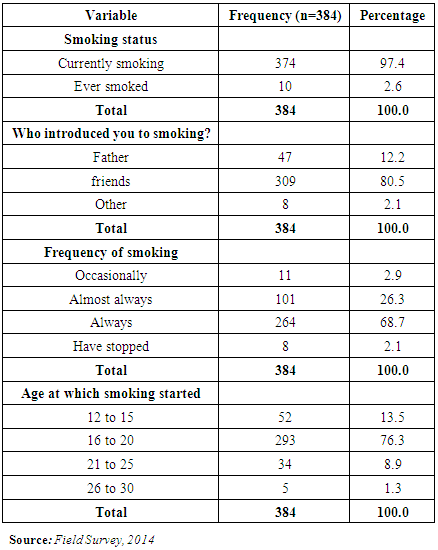
The minimum age of respondents was 15 years with the maximum age of 79 years. The mean age of the study sample was 37.8 ± 10.3 years (Mean ± Standard deviation). This showed that majority of the respondents were above 30 years. An assessment of the marital status of the respondents showed that 69.5% were married while 25% were single. The proportion of respondents who were co-habiting was 3.6% while 0.5% was widowed. Additionally, an overwhelming majority of the respondents who represented 98.4% were Muslims while Christians were 1.3%. There was only one person who was a traditionalist. Smoking Habits of RespondentsResults from respondents’ history of smoking revealed that 97.4% of them were still actively smoking. This means that only 2.6% were able to quit smoking after realizing that it was not good for their health. It is therefore not surprising that over 90% of people in Ghana who start smoking are not able to stop it but continues until death [5]. On the issue of how they started smoking, 80.5% were of the view that they were introduced to smoking by their friends, with 12.2% alleging that their fathers introduced them to the act. It also showed that 76.3% of them started smoking at ages between 16-20 years. This is also consistent with [9] who found that peer influence is one of the major causes of smoking and often victims initiated smoking at very early age in life. There was however variations in the number of cigarette sticks smoked in a week. Findings from the study revealed that 58.6% of the respondents smoked 26 to 45 cigarette sticks per week. Interestingly, only 1.3% smoked around 66 sticks per week. The number of sticks an individual smokes in a week is determined by his financial standing in some instances. The mean number of cigarette sticks smoked was 18.2 sticks per week. In the issue of the frequency with which they smoke, 68.7% of the respondents indicated that they smoked always or frequently whilst 26.3% were of the view that they smoked almost always.Smoking Practices of RespondentsThe results of the study revealed that 96.9% of the respondents buy the cigarettes they smoke with only 3% relying on the benevolence of their friends. It was observed that those relying on others were very old and were not earning any form of income, thus the reliance on others. It is also worth noting that many of the respondents rely on the locally produced tobacco when they have no money to purchase the manufactured ones or rely on the goodwill of their friends. In a report by [1], majority of smokers in India were of the view that they bought the cigarette they smoked with their own money. Similar studies conducted by [9] and [10] revealed that majority of smokers spend a lot of money on cigarettes at the expense of household food. It also came up that 77.6% of the respondents tried quitting smoking but to no avail, whilst 19.3% said that they have not thought of quitting because it is a difficult task. As [11] in their theory of behavior change stated, ‘a habit regarding the health of an individual when cultivated needs a committed action or effort to change.’ This goes to suggest that many of them are not happy with their own smoking habits. In response to venues where the smoking takes place, 41.7% indicated they smoked in the bush whilst 38% smoked in uncompleted buildings. This is an indication that they hide to smoke because the people around them detest the habit or they themselves feel shy about their own act. Those who smoked at home were 10.4% of the study sample whilst 8.3% smoked at the work place. These findings are consistent with that of [12] which found that most smokers have the desire to quit smoking but finds it difficult because of the addictions.Table 2. Smoking habits of respondents
 |
| |
|
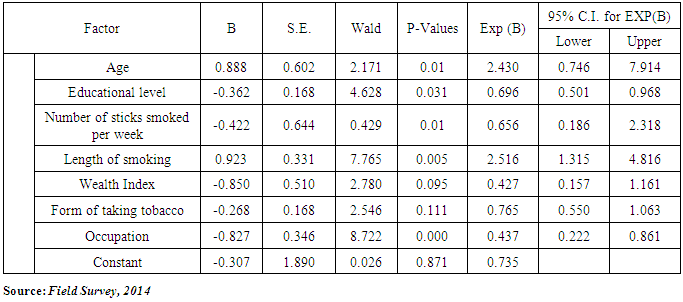
Factors that Influence smoking HabitsResults from the study revealed that smoking habit is influenced by a number of factors. It was revealed that peer influence was a cause of many people getting initiated into smoking. Though under different conditions, most of them expressed how they were influenced by their friends. As one participant put it: ….”I was introduced to smoking by my friends when we were in secondary school. We used to go into the our school forest to smoke. It was just a fun but has now become part of us. Most of the people who smoke started it in schools with their friends”…. (A discussant from Zakoli)This seems to suggest that it is very easy for people to influence each other when they are out of the sight of their parents or care takers. The reason for going to the forest, as the narrative above indicates, was to keep it off the knowledge of the school authorities. A study by [13], [14], and [15] revealed that many people are likely to smoke tobacco with their peer if their parents are not with them. Some of the respondent in this study revealed that they were made to believe that smoking was good and it could make one confident to approach issues. This probably is an expression of a group think. They all had the feeling that when you smoke, you no longer feel shy. This further implies it aids them to do things they would ordinarily not have done. It has also been observed that male whose friends, siblings, or parents smoke are more likely to smoke at an earlier age than are other male [16-18]. When growing as a child, parent-child relationship factors such as limited or poor quality familial attachments; low levels of parental supervision and strictness; inadequate parental monitoring; and lack of parental affection, concern, and involvement can lead people into smoking [9, 19, 20, 18]. Others have the conviction that it was just a source of entertainment and never thought they could get addicted. Some of the discussants said that they were given cigarettes as gifts during funerals and weddings. This culminated into a habit after smoking those pieces from the wedding and funeral grounds. Some of the statements are;..”I was given cigarettes as gifts during wedding and funeral ceremonies. These are the places where I learnt how to smoke”…. (A discussant from Kpatuya)It is vivid from the above that the more there are ritualized occasions taking place, the more people are exposed to smoking either directly or indirectly. During these occasions, it is the organizers who procure these cigarettes. Cigarette as antidepressant There were others who indicated that they were smoking because of some social problems they face in life. Some of the challenges include marital problems, employment issues, death of a beloved one etc. They indicated that they took to smoking because they wanted to suppress the painful memories:….”When I quarrel with my wife and I am so furious about the situation, I leave the house to join my colleagues to smoke. As we smoke and discuss other issues I tend to forget about it”…… (A discussant from Kuga)In a similar vein, another discussant intimated:…”I started smoking and drinking alcohol from the day I lost my wife. It was a very sad day for me so I started drinking alcohol and later added smoking to it to help me forget about the painful situation”….. (A discussant from Gbrimani)These revelations as indicated by these respondents’ points out how they use cigarette as antidepressants. This view was expressed by many other respondents to explain why they continue to smoke. With this mindset, people will continue to smoke as long as they believe that smoking takes their stress off them. Knowledge of Health Hazards of SmokingThe knowledge of respondents was assessed on health hazards associated with tobacco use. The results show that 51.3% of the respondents were aware of health risk associated with smoking. 48.2% however indicated that they did not know of any health risk associated with smoking. The study findings are consistent with that of [21] that smokers are aware of the dangers of cigarette smoking but they were not able to stop it because it is a habit developed over time. Interestingly, 74.2% of the respondents were of the view that they were not aware of health hazards associated with passive smoking. With regard to the health status of smokers, 77.6% of the respondents indicated they had illness with dry cough whilst 22.4% said that they have never had illness with dry cough. This appears to be consistent with [22] report that suggests that the use of tobacco causes cancer and some cardiovascular diseases.The respondents had different sources of information about the use of tobacco; 6.8% said they had information on tobacco use from health facilities whilst 10.4% said that they heard messages on tobacco use from radio and television. An assessment of the preferred place or source for information on the health risk of tobacco use showed that 66.9% said that they prefer to hear messages on tobacco. Even though it has been stated on the cigarettes pack that tobacco use is dangerous to the health of individuals who use it, it appears a greater majority of smokers cannot read and write and more so, quite a number smoke tobacco they produce themselves. Determinants of Health Status of SmokersIn logistic regression, determinants of health related complications among respondents were assessed based on those who have ever recorded diseases associated with smoking. Age was found to be significantly associated with the health complications of respondents (P<0.01, OR=2.171, 95%, CI: 0.746-7.914). This suggests that respondents who were younger were less likely to have health complications associated with smoking as compared to older respondents. Additionally, the length or years of smoking was also found to be statistically significant as respondents who had smoked for long had experienced some diseases associated with smoking (P<0.005, OR=7.765, 95%, CI: 1.31-4.81). It also emerged that the number of cigarette sticks smoked per week was also found to be a determinant of the health status of smokers in that respondents who smoked high number of cigarette sticks per week were found to have health complications compared to those who smoked fewer sticks (P<0.001, OR=8.722, 95%, CI: 0.22-0.86). Other factors that were found to be statistically significant were education level of respondents (P<0.0034, OR=4.494, 95%, CI: 1.023-1.782) and wealth index of respondents. See table 3 below.Table 3. Determinants of health status of smokers
 |
| |
|
4. Conclusions
The information reviewed in this article on the socio-cultural influences on tobacco use reveals multiplicity of factors contributing to the continued use of tobacco. The multifaceted nature of the problem demands policy makers and especially public health practitioners and other health care providers to device strategies that could be employed to discourage tobacco use. Halting the use of tobacco is one of the most important issue a person can do to improve his health and people who are able to quit smoking before age 30 have a normal life expectancy. Additionally, those who quit smoking in their sixties and seventies may also reduce the risk of developing lung cancer, cardiovascular disease, and chronic obstructive pulmonary disease. Though people significantly do not spend much money in purchasing tobacco, those who purchase spends much money on tobacco. It has been observed that most of the smokers are sick more often, adding to their already significant financial costs of tobacco. It came up that many of the smokers did not know the effects the smoke has on those who do not smoke; the impact is not only on the persons who smoke, but on those who inhale the smoke. The public ought to be educated on the looming dangers associated with inhaling tobacco smoke from other smokers. In relation to the use of tobacco as part of ritualized ceremonies, education should target this phenomenon to educate them on the need to get alternatives. The time and resources needed to take care of people who are ill, the physically challenged, and people dying from tobacco-related illness, affects the physical and mental health of caregivers and their ability to care for children and other members. It can also reduce the care givers personal and economic development.Improving the health of tobacco users demands enforcement of legislations that seek to ban smoking in public vehicles and public places. Since many of the people smoking leant that act of smoking from their peer, ban on cigarette sale to young people should be strictly enforced. More effort also needs to be put into understanding and counteracting marketing through the internet and movies, and related events. Given the high proportion of young people in the population, such action would be of special benefit to the smokers. New media campaigns to educate the general public on the additional dangers of smoking would also be appropriate. Dedicating some public health research funds to the development of smoking cessation programs tailored to the needs and interests of recovering addicts would also be useful. Other innovative strategies could be considered as well. State legislatures could be urged to pass laws prohibiting smoking and tobacco purchases in bars. The entertainment and advertising industries could be encouraged to avoid images of people smoking cigarettes in scenes.
References
| [1] | World Health Organization (2011) WHO report on the global tobacco epidemic, retrieved fromhttp://whqlibdoc.who.int/publications/2011/9789240687813_eng. |
| [2] | Mathers CD, & Loncar D (2006) Projections of Global Mortality and Burden of Disease from 2002 to 2030, PloS Medicine 3(11):e442. |
| [3] | Kurtz ME, Azikiwe U, & Kurtz JC (1993) Nigerian urban married women’s perceptions of exposure to secondary tobacco smoke, Health Care Women Int; 14(3):239–48. |
| [4] | Ivey SL, & Faust S (2001) Immigrant women’s health: initial clinical assessment, West J Med; 174(6): 433–7. |
| [5] | Shafey O, Eriksen M, Ross H, & Mackay J (2009) Types of Tobacco Use: The Tobacco Atlas. A. C. Society." Atlanta, GA, USA: Bookhouse Group, Inc. |
| [6] | Gryczynski J, Feldman R, Carter-Pokras O, Kanamori M, Chen L, & Roth S (2010) Contexts of tobacco use and perspectives on smoking cessation among a sample of urban American Indians. J. Health Care for the Poor and Underserved, 21: 544–558. |
| [7] | Webb MS, Francis J, Hines BC, Quarles FB (2007) Health disparities and culturally specific treatment: Perspectives and expectancies of African American smokers. J. Clin. Psychol, 63: 1247–1263. |
| [8] | Fu SS, Burgess D, van Ryn M, Hatsukami DK, Solomon J, Joseph AM (2007) Views on smoking cessation methods in ethnic minority communities: A qualitative investigation. Prev. Med, 44: 235–240. |
| [9] | Conrad KM, Flay BR, & Hill D (1992) Why children start smoking cigarettes: Predictors of onset. British Journal of Addiction 87(12):1711– 1724. |
| [10] | Edwards VJ, Anda RF, Gu D, Dube SR, & Felliti VJ (2007) Adverse Childhood Experiences and Smoking Persistence in Adults with Smoking-Related Symptoms and Illness; The Permanente Journal, 11(2): 5-13. |
| [11] | James OP, Carlo CD, JC, & John CN (1992) In Search of How People Change Applications to Addictive Behaviors, American Psychologist, Vol. 47(9): 1102-1114. |
| [12] | Warren CW, Jones NR, Peruga A, Chauvin J, Baptiste JP, Costa de Silva V, El Awa F, Tsouros A, Rahman K, Fishburn B, & Bettcher DW (2008) Centre for Disease Control and Prevention (CDC): Global Youth Tobacco Surveillance, 2000-2007. MMWR Surveill, 57(1): 1-28. |
| [13] | Gritz ER, Prokhorov AV, Hudmon KS (1998) Cigarette smoking in a multiethnic population of youth: Methods and baseline findings. Preventive Medicine 27(3):365–384. |
| [14] | Flay BR, Hu, FB, & Richardson J (1987) psychosocial predictors of different stages of cigarette smoking among high school students. Preventive Medicine 27:A9–A18. |
| [15] | Mittelmark MB, Murray DM, & Luepker RV (1987) Predicting experimentation with cigarettes: The childhood antecedents of smoking study (CASS). American Journal of Public Health 77(2):206–208. |
| [16] | Unger JB, & Chen X (1999) The role of social networks and media receptivity in predicting age of smoking initiation: A proportional hazards model of risk and protective factors. Addictive Behaviors 24(3):371–381. |
| [17] | Botvin GJ, Malgady RG, Griffin KW, Scheier LM, & Epstein, JA (1998) Alcohol and marijuana use among rural youth: Interaction of social and intrapersonal influences. Addictive Behaviors 23(3):379–387. |
| [18] | Brook JS, Whiteman M, Gordon AS, Nomura C, & Brook DW (1986) Onset of adolescent drinking: A longitudinal study of intrapersonal and interpersonal antecedents; Advances in Alcohol and Substance Abuse 5(3): 91–110. |
| [19] | Biglan A. Duncan TE. Ary DV, & Smolkowski K (1995) Peer and parental influences on adolescent tobacco use, Journal of Behavioral Medicine 18(4):315–330. |
| [20] | Hundleby JD, & Mercer GW (1987) Family and friends as social environments and their relationship to young adolescents’ use of alcohol, tobacco, and marijuana; Journal of Marriage and the Family 49(1):151–164. |
| [21] | Audrain-Mcgovern J, Rodriguez D, Epstein LH, Rodgers K, Cuevas J, & Wileyeto EP (2009) Young Adult Smoking: What factors differentiate ex-smokers, smoking cessation treatment seekers and non-treatment seekers? Addicts behaviour, 34(12): 1036-1041. |
| [22] | Ahmed R, Rizwan UR, McDonald PW, & Ahmed SW (2008) Prevalence of cigarette smoking among young adults in Pakistan; JPMA, 58(11): 597-601. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML