-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2016; 6(2): 38-44
doi:10.5923/j.phr.20160602.02

The Inextricable Effect of Health Worker’s Attitude on Primary Health Care Implementation in South-South Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. P. Inyang, Walker Doubrapade
Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Nigeria
Correspondence to: Walker Doubrapade, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study was designed to investigate the negative effect of health workers attitude on primary health care implementation in south-south Nigeria. The descriptive cross sectional survey design was utilized for the study. Three research questions and three hypotheses guided the study. A sample size of one thousand one hundred and twenty (1,120) primary health care workers, which is 10% of the total population, was used for the study. Multi-stage sampling procedure was adopted to pick the desired number of respondents for the study. A self-structured questionnaire with a modified 4-point Likert type scale of strongly agree (SA)-4points, Agree (A)-3points, strongly disagree (SD)-2points, Disagree (D)-1point was used for data collection. The reliability of the instrument was determined through the test-retest method with the use of Pearson product moment correlation and a reliability coefficient of 0.81 was established. The data generated from the study were coded, analyzed using the Statistical Package for Social Sciences (SPSS) batch system and hypotheses tested using Z-test and ANOVA statistical tools. Descriptive statistics of mean was used to answer the research questions and a criterion mean of 2.50 was established in taking decision concerning the research questions. However, the result of the analyzed data from the opinions of respondents pointed to the fact that majority of them agreed that, the three variables under consideration pose challenge to primary health care implementation in south-south Nigeria and it was recommended that health workers should be retrained on the basic principles of interpersonal communication while delivering health services to the people.
Keywords: Primary Health care, Maternal mortality, Infant mortality, Health center, Disease prevention, Community participation
Cite this paper: M. P. Inyang, Walker Doubrapade, The Inextricable Effect of Health Worker’s Attitude on Primary Health Care Implementation in South-South Nigeria, Public Health Research, Vol. 6 No. 2, 2016, pp. 38-44. doi: 10.5923/j.phr.20160602.02.
Article Outline
1. Introduction
- Primary health care is a grass-root approach aimed at achieving universal and equitable distribution of health care services for all. Primary health care, as conceptualized at the Alma Ata declaration, is meant to address the main health problems in the community, providing promotive, preventive, curative and rehabilitative services to all individuals and families in the community (Alenoghena, Aigbiremolen, Abejegah & Eboreime, 2014). The Declaration of Alma-Ata defines Primary Health Care as essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community can afford to maintain at every state of their development in the spirit of self-reliance and determination (Litsios, 2002). As affirmed by Olise (2007), it is the first level of contact of individuals, families with the national health system, bringing health care as close as possible to where people live and work. It constitutes the first element of the continuing health care process. According to Egwu (2006), the eight basic components, that will guide the progammes of primary health care in any countryas established at the Alma-Ata conference include; education concerning preventing health problems and methods of preventing them; promotion of food supply and proper nutrition; adequate supply of safe water and basic sanitation; maternal and child health care including family planning; immunization against the major infectious diseases; prevention and control of locally endemic diseases; appropriate treatment of common diseases and injuries and provision of essential drugs. However, in Nigeria, two additional components have also been added to extend the scope of coverage of Primary Health Care based on the health needs of the population. According to Adeyemo (2005), the two additional components of Primary Health Care in Nigeria are provision of community mental health care and community dental health care.Alenoghena et al (2014), contributed that, Primary Health care should be supported and sustained by integrated, functional, and mutual supportive referral systems that will lead to a progressive improvement of comprehensive health care for all, and giving priority attention to those communal needs that are most pressing. Above all, Primary Health Care Programmes should rely on health workers trained specifically to work at the local, and referral levels. They include physicians, nurses, midwives, auxiliary and primary health workers as applicable, as well as traditional practitioners as needed, suitably trained, socially and technically to work as a health team and respond to meet the health needs of the community (Magawa, 2012).The performance of primary health care system has traditionally been assessed in terms of coverage and quality of services provided at the various levels primary health care implementation. The coverage level and quality of services rendered in the primary health care system are directly tied to the competence, versatility, commitment and dedication of the various cadres of primary health care staff that are readily available to implement the various programmes of primary health care at all levels of care. The health worker play a basic and significant role in the implementation of primary health care at all levels (Adulraheem, Oladipo & Amodu, 2011). They carry out the actual implementation of primary health care at the rural areas in the local government areas. However the attitude, mindset, knowledge and behavior are important factors that determine the professional output of the health workers at any level of care in the primary health care system. As affirmed by Obioha and Molale (2011), poor attitude and behavior of health staff and low staff motivation and morale are some major indicators of poor quality of primary health care services.The policy may be excellent and result-oriented, but if the work force (staff) exhibit a counterproductive attitude in the course of implementation, the desired result may not be achieved. For primary health care policies and objectives to be translated to meeting the health needs of individuals and members of the community, the work force must be motivated and their morale highly boasted to a large extent with good working environment, regular and sustainable pay package and adequate provision and supply of drugs and equipment, infrastructure and other material resources that are required for effective implementation of primary health care at every level (Abimbola, 2012). The attitude and behavior exhibited by staff while delivering health services at the health centers and other outreach settings will significantly determine the level of utilization of health services and patient patronage to health centers in the community. The average patient/client visiting the health facility expects empathy and responsiveness from the staff. The reverse insensitivity and harshness displayed by most primary health care staff possess the potential to drive patients away from the health center (Gupta, Guari & Khemani, 2004). According to Sule, Ijadunola, Fatusi and Connell (2008) other attitudinal deficiencies reported among primary health care staff include discrimination of patients/clients based on their status and influence, lack of respect and compassion towards patients, careless and frivolous comments on patients by staff, unfriendliness and insensitivity to patients problems, laxity in dealing with patients waiting for attention, abandonment of place of work for personal gains, mismanagement of fund, drugs and other health care materials, drug leakage and illegal drug selling. As emphasized by Obembe et al (2014), the poor attitude exhibited by the availableprimary health care staff on daily basis at the health center may have contributed greatly to the unimaginable record of performance of the primary health care system of Nigeria.
2. Statement of the Problem
- The concept of primary health care was designed and initiated globally to address the main health problems of individuals and families in the community. This is achieved by the provisions of promotive, preventive, curative and rehabilitative services to every member of the population especially those at the rural areas where more than 65% of the population live. The implementation of primary health care is primarily through health services rendered at the health centers. These services are carried out by several cadres of primary health care staff professionally trained and working directly at the health centers. According to Bangdiwala, Fonn, Okoye and Tollman (2010), there are several challenges that continue tobedevil the implementation of primary health care which could be traced to the attitude of health staff. Supporting Bangdiwala et al (2012), Omoleke (2005) averred that, there is a wide spread dissatisfaction expressed by patients and clients about health services rendered at the health centers despite the fact that almost all health centers established under the primary health care system have a minimum number of staff who are supposed to carry out integrated primary health care services to meet the health needs of the community. There is also the steady rise in disease outbreaks that have consistently challenged the primary healthcare system, patients not utilizing health services, health centers empty without staff and increase patronage of secondary level of care by members of rural communities. More worrisome is the fact that pregnant mothers and other cure seeking individuals prefer the Traditional Birth Attendant and local patent medicine stores to the primary health centers (Center for Population and Environmental Development, 2014). All these variables coupled with the current rate of maternal and child mortality rates prompted the researcher to investigate if the attitude of primary health care staff can pose a great challenge to primary health care implementation in south-south Nigeria.
3. Purpose of the Study
- The purpose of the study is to investigate the effect of primary health care workers attitude on the implementation of primary health care in south-south Nigeria. Specifically the study tends to establish if • Mismanagement of available fund will affect primary health care implementation• Absenteeism of health workers will affect primary health care implementation• Unfriendliness of health workers will affect primary health care implementation.
4. Research Questions
- The following research questions guided the study1. To what extent does absenteeism of health workers pose a challenge to primary health care implementation in south-south Nigeria.2. To what extent does mismanagement of fund pose a challenge to primary health implementation in south-south Nigeria.3. To what extent does unfriendliness of health workers pose a challenge to primary health care implementation in south-south Nigeria.
5. Hypotheses
- The following hypothesis were postulated to guide the and were test at 0.05 level of significance.1. There is no significant difference between the opinion of male and female PHC staff on mismanagement of fund as challenge of Primary Health Care implementation in south-south Nigeria.2. There is no significant difference between the opinions of urban and rural PHC staff on staff absenteeism as a challenge of Primary Health Care implementation in south-south Nigeria.3. There is no significant difference between the opinions of different cadres of PHC on unfriendliness of staff as a challenge of Primary Health Care implementation in south-south Nigeria.
6. Methodology
- The descriptive cross sectional survey design was utilized for the study. All the primary health care workers serving at various health centers and LGA in the south-south geopolitical zone formed the study population. A sample size of one thousand one hundred and twenty (1,120) primary health care workers, which is 10% of the total population, participated in the survey. Multi-stage sampling procedure was adopted to pick the desired number of respondents for the study. The instrument used for the collection of data for the study was a self-structured questionnaire with a modified 4-pointLikert type scale with response options of Strongly agree (SA)-4points, Agree (A)-3points, strongly disagree (SD)-2points, Disagree (D)-1point, and it was titled Questionnaire on Effect of Health Worker’s Attitude on Primary Health Care Implementation (QEHWAPHCI). The instrument was in two sections with section-A having 3 question items on Personal data, while section-B had 7 question items covering the variables under study. The content and face validity of the instrument was ascertained by 3 experts in the field of health education. The reliability of the instrument was determined through the test-retest method with the use of Pearson product moment correlation. A reliability coefficient of 0.81 was established after the correlation of the two sets of data using Pearson product moment. The data generated from the study were coded, analyzed using the Statistical Package for Social Sciences (SPSS) batch system and hypotheses tested using Z-test and ANOVA statistical tools at 0.05 level of significance. Descriptive statistics of mean was used to answer the research questions and a criterion mean of 2.50 was established to take decision concerning the research questions. However any item or grand mean that equals or greater than the criterion mean of 2.50 was adjudged to as ‘accepted’ means that respondents accepted that item as a possible effect of health workers’ attitude on primary health care implementation, while any item or grand mean that falls below the criterion mean of 2.50 was considered as ‘rejected’ means that respondents did not accept that item to be a possible effect on primary health care implementation in south-south Nigeria.
7. Results
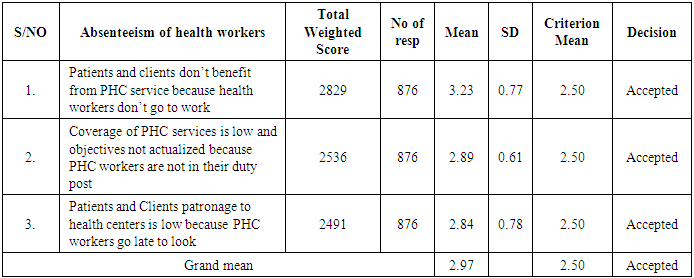
- Table 1 shows that, the mean score of respondents on patients and clients don’t benefit from PHC service because health workers don’t go work was (3.23). Mean scores, 2.89 and 2.84 respectively were for coverage of PHC services is low and objectives not actualized because PHC workers are not in their duty post and patients and clients patronage to health center is low because health workers go late to work. With a grand mean of 2.97 which is greater than the criterion mean of 2.5, the researcher concluded that, absenteeism of Health Workers is a challenge facing primary Health care implementation to a high extent in south-south Nigeria.
|
|

|

|

|

|

8. Discussion
- One significant area covered and investigated in this study was absenteeism of staff as a challenge of Primary Health Care Implementation. The result revealed that, respondents recorded a grand mean score of 2.97, which was greater than the criterion means of 2.50. This implies that, absenteeism of staff is a challenge facing primary health care implementation in South-South Nigeria. However, this result is not surprising, considering the present unstable political system that does not encourage the welfare and well-being of staff. The present state of delay in payment of salary and allowances running to months that is observable in the Primary Health Care System may also be a reason that had led respondents in this direction. Government insincerity and failure to place more emphasis on providing modern primary health centers with staff residential quarters with basic social amenities also determined the respondents’ opinion, who are also part of primary health care implementation at the local government level. The result is in agreement with the findings of Emeka and Masemote (2011), who carried out a study on function and challenges of primary Health Care Implementation in Roma province of Lesotho and found out that absenteeism of staff was a major factor impeding smooth implementation of primary health care. Similar results were also observed in related studies by Makau, Paul, Banda, Mbere, Charles and Adamson (2012), and World Bank (2013). The result of the studies carried out by Abimbola (2013) and ozochukwu, Akpala and onuwujekwe (2004) were inconsistent with this present study. The divergent of their findings may be attributed to the fact that, these studies were carried out at a time, when there was a prevailing health challenge that had a great public health importance and as such the government provided incentives that attracted the health staff to be present at work and there was a committed supervision that could not create the room for absenteeism.From the result it is also clear that mismanagement of fund is a challenge of primary health care implementation in South-South Nigeria, with a grand mean score of 2.84 which is greater than the criterion mean of 2.50. This result was not surprising considering the high level of corruption that have bedeviled the various sectors of our national economy, which has also crept in to the primary health care delivering system. The result can also be attributed to the fact that, outcomes and indices from the primary health sector are not commensurate with the available scare resources expended on the sector by both government and other partner agencies. However, the findings validates the views of Brown and Bernleth (2000), Dedalike (2002) and Hallfors, Pankratz and Hartman, (2007). The findings from these studies convincingly revealed that, mismanagement of available funds designated for primary health care implementation will truncate the achievement of set objectives and goals. This finding is also in consonance with Adeyemo (2005), whose findings revealed that, shortage of man-power, misappropriate of fund, insufficient fund, lack of political will and community involvement are some major challenges primary health care implementation was facing. Moreover the findings of studies carried out by Ozochukwu et al. (2004), Makaula et al. (2012), and Olatunde (2012) were inconsistent with the present study. Their results showed that, there is a challenge of funding in the primary health care sector but the available little funds are appropriately managed by the coordinators of the various programmes in the primary Health care departments in the local government councils. This divergent of results might be attributed to the fact that, these studies were aimed at investigating the level of implementation and achievements of some specific programmes implemented under the umbrella of primary health care, which were monitored and supervised strictly by several donor agencies. The study also revealed that unfriendly attitude of health worker posed a challenge to primary health care implementation to a high extent in south-south Nigeria. This finding is not surprising considering the significant role played by health workers. They are the actual implementers of primary Health care at the grass root level hence whatever behavioural inconsistency and insensitivity to patients and clients’ needs exhibited by them may indirectly affect primary health care implementation. Another factor that may have contributed to this result was the fact that the study was carried out at a time when there is a high level of community patronage to village patent medicine stores and TBAs. This finding is in consonant with the findings of studies carried out by Mihalic and Iriwin (2003) Elliott and Mihalic (2004), Adeyemo (2005), and Obembe, Osungbade, Olumide, Ibrahim and Fawale (2014). The results of their studied at various times pointed to the fact that the unfriendly attitude of health workers has direct implication on the smooth implementation of primary health care. Furthermore this result contradicts the views of Akaniyere et al (2014), who in a study investigating the perception and attitude of community and health care providers about health policy and services, concluded that several factors in the primary health care delivery system can influence the attitude of health workers negatively in the discharge of their duties.
9. Conclusions
- The result of the analyzed data from the opinions of respondents pointed to the fact that majority of them agreed that, the entire three variable under consideration pose challenge to primary health care implementation in south-south Nigeria. The results also revealed some variations in the responses of respondents based on gender, staff cadre, and location. Moreover these variations do not significantly contradict the fact that, absenteeism, unfriendly attitude of workers, mismanagement of fund are challenges facing primary health care implementation in south-south Nigeria. In tandem with the above and the prevailing high maternal and child mortality rates in Nigeria especially south-south, it could be concluded that primary health care implementation in the south-south region of Nigeria might be negatively affected by some challenges.
10. Recommendations
- Based on the findings of the study and the conclusion thereof, the following recommendations were made. 1. The wide spread negative attitude of primary health care workers towards their duties has significantly impeded the successful achievement of primary health goals and objectives. Although this negative attitude of health workers may be attributed to the low level of professional competence and lack of knowledge of profession ethics, but it is Marjory behavioural. Hence the need for effective supervision and reorientation of health workers on the ethical provisions of the profession in continual basis is strongly recommended 2. Health workers should be retrained on the basic principles of interpersonal communication while delivering health services to the people. 3. From the findings, it was also revealed that, the primary health care implementation is relatively under funded with the available fund mismanaged to the detriment of set goal and objectives. In view of this, adequate and sustained funding from government, partner and door agencies and other well-meaning individuals from the private sector is highly recommended. 4. There is also the urgent need to institute a viable and uncompromising machinery to strictly supervise and monitor the way and manner in which available funds are managed and utilized to achieve set goals and objectives of primary health care. Co-coordinators of Primary Health Care programme should be exposed to effective financial management and budgeting principles through seminars and workshops in a sustained manner.