-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2016; 6(1): 1-17
doi:10.5923/j.phr.20160601.01

The Efficacy of HIV and Sex Education Interventions among Youths in Developing Countries: A Review
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLLaud Alfred Dei Jnr
Monitoring and Evaluation, World Education Inc, Ghana
Correspondence to: Laud Alfred Dei Jnr , Monitoring and Evaluation, World Education Inc, Ghana.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Human Immunodeficiency Virus (HIV) and Sexually Transmitted Infections (STIs) among youths represent an important public health challenge in developing countries. The incidence of HIV peaked in the 1990’s and saw a decline from 2005. What was done to prompt the decline? To answer this question selecting studies between 1990 and 2005 was appropriate to assess whether the drop in HIV incidence in developing countries was as a result of education interventions. School based interventions are widely used to change young people’s attitudes towards early sexual activity and to prevent the transmission of HIV/STIs, and have been implemented by countries across the world. Methods: Electronic databases were searched to identify studies in HIV/STI education interventions conducted in schools in developing countries published from 1990 to 2005. Studies from 1990 effectively gave a clearer explanation of whether education interventions contributed to the genesis of the decline. In addition to assessing HIV incidence, the reviewer also included studies performed on sexually transmitted infections (STIs) as knowledge on STI prevention could lead to preventing HIV transmission. Studies were eligible if they had an appropriate comparison group; published in English and full text retrieved. Twenty-eight full text articles were assessed for eligibility, 17 articles met the inclusion criteria and 11 articles were rejected due to, not addressing HIV or sex education programmes in schools or were abstracts only. The Cochrane Effective Practice and Organization of Care tool for randomized controlled trials (RCTs), non-randomized controlled trials (NRCTs) and controlled before and after (CBA) studies was used to critically appraise studies. Results: All 17 studies reviewed established positive effects on knowledge. Programmes have similar characteristics and were more effective if they were conducted by adults. Conclusions: The overall conclusion of evidence gathered was that curriculum based programmes on HIV and sex education could be effective in changing the behavior of young people in developing countries if conducted properly. They were also effective in increasing knowledge on problems associated with risky sexual activity among young people. Further research is needed to assess the long-term positive effects of such programmes in schools in developing countries.
Keywords: HIV and Sex Education, Youths, Developing Countries
Cite this paper: Laud Alfred Dei Jnr , The Efficacy of HIV and Sex Education Interventions among Youths in Developing Countries: A Review, Public Health Research, Vol. 6 No. 1, 2016, pp. 1-17. doi: 10.5923/j.phr.20160601.01.
Article Outline
1. Introduction
- The human immunodeficiency virus (HIV) is recognized as one of the major public health concerns for many years (WHO 2006). This problem still remains high notably in developing countries. In 2012 the World Health Organization (WHO) and the Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated that globally 2.3 million people were newly infected with HIV, 35.3 million people were already living with the virus, and 1.6 million people died from AIDS-related causes (USAID 2013); youths aged 15-24 years account for more than 10 million. In the same year 2.5 million people were newly infected with HIV and 1.7 million people died from acquired immunodeficiency syndrome (AIDS)-related causes (UNAID 2012). Sub-Saharan Africa is the region most severely affected; with young people living with HIV accounting for 3.9 million (UNAIDS 2011). Although young people are generally seen as the healthiest phase of life, it is also a period of experimentation and exploration, with developmental changes in major areas such as sexual identity, sexual practices and behaviors. The unique biopsychosocial changes linked with this age group leads to an unequal risk of HIV infection. According to Boonstra (2011) a large number of young men engage in sex before marriage; however, females have also become known recently to engage in premarital sex, which may probably be because of the marriage age being delayed.
1.1. Why Young People are Vulnerable
- The time between childhood and adulthood involves a variety of different variations between and within individuals in terms of their physical, psychological and social development that take place. There are other factors apart from their age that influences their behavior, these factors include, marital status and economic dependence which are associated with how the society views young people and how they see themselves. The period when puberty takes place is known as adolescence, this is when majority initiate sex and form their sexual preferences and identity. Worldwide, young people account for almost half of all new HIV infections among individuals aged 15 and older in 2010 (UNAIDS 2012). According to the USAID/FHI (2010), people responsible for HIV/STI programmes need to understand the changes that take place during adolescence. This is because these changes in adolescents affect the following;Ÿ How the people translate and understand the information.Ÿ The type of information and how it influences their behavior.Ÿ How adolescents look at the future and their present decisions.Ÿ Whether they are conscious of the risks involved when experimenting.Ÿ How they get involved in relationships, respond to social values and norms that surround them, and are influenced by the attitudes of their peers and others around them. Young people’s needs for health and development have been grouped in four major areas by the World Health Organization (WHO), the United Nations Population Fund (UNFPA) and United Nations Children’s Fund (UNICEF) which include; comprehensive information and life skills; safe and supportive environments and opportunity for participation. In order to meet these needs for young people, several people have to be involved; these are namely, parents, peers, teachers, service providers, community and religious leaders and policymakers. According to studies conducted in 50 countries, there are common determinants associated with early sexual activities that undermine young peoples’ health (WHO 2001). These determinants could either expose the individual to risk factors or a protective factor. They include, how the young person relates to his or her parents, other adults within their communities, the school environment, the attitude of peers and spiritual beliefs. Protective factors promote the prevention of early sexual activity, these include, positive relationship with parents, positive school environment and spiritual beliefs. On the other hand, risk factors associated with early sexual activity include negative friends and engaging in risky behaviors (Blum & Mmari 2004).Studies indicate that sexual practices among youths is a reality, women in Latin America account for more than 40% and the Caribbean report engaging in sexual activity by age 18, and close to 60% in Sub-Saharan Africa (Boonstra 2011). Sexual activity is commenced in most developing countries in early adolescence, before age 15 years (UNAIDS 2012). Young people are generally known to be at the center of the AIDS pandemic irrespective of whether they live in concentrated or generalized epidemic countries. There are a number of factors that expose young people to HIV; these factors include inadequacy of life skills training, inadequate knowledge of the disease, lack of parental protection and role models, lack of financial security, early sexual encounter, sex under duress, partner violence, and inadequate accessibility to health facilities (UNAIDS 2008).Health promotion interventions educating young people on HIV prevention is highly necessary. It is important that action is taken to give young people the training, skills and knowledge to make important choices regarding HIV gender equality and their sexual and reproductive health, as well as dealing with gender-based violence (UNAIDS 2012). Although the incidence of HIV among youth globally is decreasing, notably, due to behavioral changes, people who have already been infected with HIV need to live healthy and productive lives through support (UNAIDS 2009). Efforts to reduce the HIV transmission among youths does not often get to those who are highly at risk (UNAIDS 2010) and a lot of programs do not address intergenerational sexual partnerships (UNAIDS 2009). On all counts, schools-based HIV interventions would be a better position method than non-school based HIV interventions, to reach the ultimate aim of reducing the HIV incidence among young people. Even though school-based interventions may not be relevant where a lot or most of the youths have completed school or dropped out of school, it is the only institution which is constantly attended by youth within most communities. Most of these young people start school before they begin engaging in sexual activities and others would have begun intimate sex when they enrolled. Accordingly, the school provides the chance for interventions to capture young people before or just before the time they are sexually active.
1.2. Current Global HIV Situation
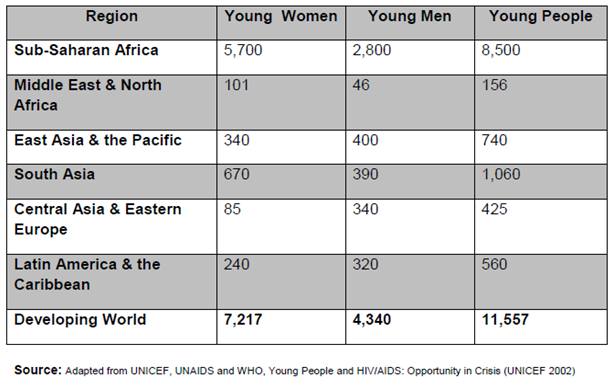
- Youths (aged 15-24 years) make up about 18% (1.2 billion) of the world’s population of about 6.7 billion people (United Nations, 2007). The behaviors of youths are influenced by a number of factors which include knowledge and attitudes; relationships with teachers, parents, and peers; performance in school; environmental and socioeconomic contexts; and accessibility to health services. It is understood generally that a large number of youths who are sexually active, do not practice monogamy in their sexual relationships, and do not like using condoms regularly, as it shows in the high incidence of HIV among youths globally (United Nations 2007). Youth risk taken behaviors are usually seen in terms of risk clustering, as various risk behaviors take place at the same time, such as drug use and engaging in unprotected sex and sometimes delinquency. The determinants for these behaviors seem to be common; meaning that they are affected by the same risk and protective factors (UNAIDS 2004). A number of countries have embarked been involved in an intensive communitywide, group-level and mass media interventions and the antiretroviral treatment programmes being widely introduced to address HIV prevention worldwide (UNAIDS 2007). Even though the progress has been made over the last ten years in scaling up the response, the HIV pandemic still remain a very serious communicable disease and a challenge to global public health (WHO 2006). Out of eight main areas covered by the Millennium Development Goals (MDGs), six namely, increased access to education, reduced poverty and child mortality, gender equality, improved maternal health and efforts to combat major infectious diseases, are not progressing as expected due to the continues spread of HIV and its development to AIDS (UNAIDS 2000). In 2006, governments of the world committed “to ensure an HIV-free future generation through the implementation of comprehensive, evidence based prevention strategies, responsible sexual behavior, including the use of condoms, evidence and skills-based youth specific HIV education, mass media interventions, and the provision of youth friendly health services” at the United Nations High Level Meeting on AIDS (UNGASS, 2006. p. 26). They recognized the need to give young people more attention by identifying the appropriate goals for interventions aiming at youths. To achieve these goals will demand that government and organizations to work with youths and donor agencies make sure that the youth (aged 15-24) years have the relevant information on HIV and health services including programmes that will encourage them to build skills to avoid them from being infected with HIV and other Sexually Transmitted Diseases (STIs); the results leading to a decrease in young peoples’ prevalence of and vulnerability to the HIV infection. Table 1 below shows the estimated number of young men and women aged 15-24 years who were living with HIV as at 2001. As shown in this table, the estimated proportion of women living with HIV (5,700) is twice that of men (2,800) in Sub-Saharan Africa, adding up to 8,500 young people living with HIV in 2001. This is followed by South Asia (1,060), then East Asia and the Pacific, then Latin America and the Caribbean. These figures may have increased since 2001 due to the availability of the antiretroviral drug. The Middle East and North Africa, even though are part of the developing world, some economic, cultural and religious factors prevents young people from.
|
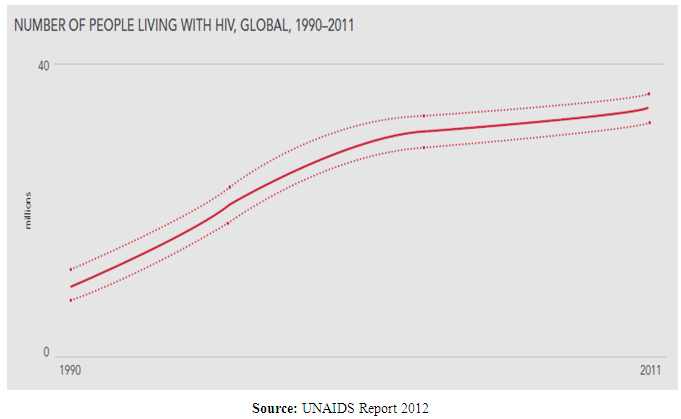 | Figure 1. Global HIV Trends 1990-2011 |
1.3. Trends of HIV among Young People in Developing Countries
- Globally, the number of newly infected (adults and children) fell from 2.8 million in 2001 to 2.2 million in 2011 20% lower than in 2001 (UNAIDS, 2012). Figure 2 below show a graphical representation of global trends of newly infected from 1990 to 2011 (UNAIDS 2012). It shows how the rate of infection has gradually falling since the mid to latter part of the 1990’s and still continues to fall. In Sub-Saharan, recent estimates show that there has been 25% fall in HIV infections since 2001 (UNAIDS 2012).
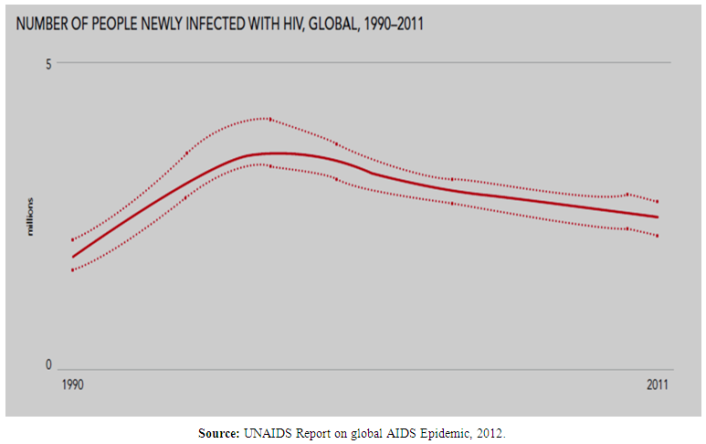 | Figure 2. Newly infected-Global Trends |
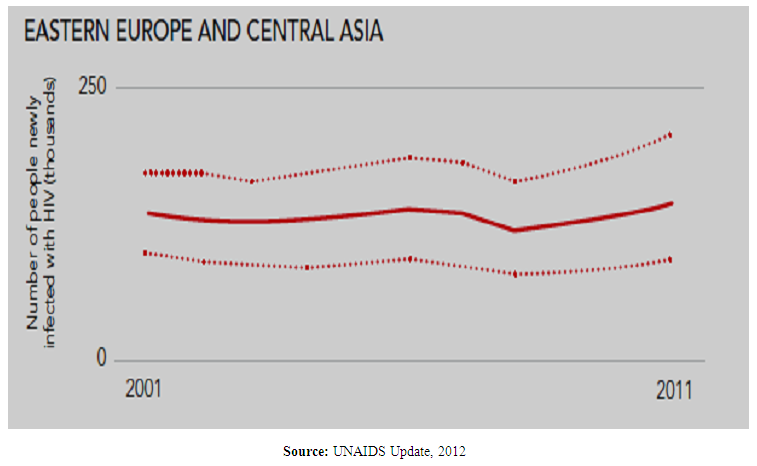 | Figure 3. Eastern Europe and Central Asia |
1.4. Definition of Youth
- Youth refers to the period between childhood and adulthood. In many countries, the terms "young person", "teenager", "adolescent", and "young adult" are used to describe this period. The United Nations General Assembly defines youth as "all persons falling between the ages of fifteen and twenty four inclusive" (United Nations 2010), even though it recognizes the nuances that may exist with this definition in various countries. They also acknowledge other subgroups like adolescents (ten to nineteen years of age) and young people (ten to twenty four years of age; FHI 2010). Additionally young people may be categorized as teenagers (thirteen to nineteen years of age) or young adults (twenty to twenty four years of age). Individuals in these different age groups may face different psychological, social and health problems. But for the purposes of this paper, the term "youth" and “young people” will be used interchangeably and will refer to persons aged from fifteen to twenty four years.
2. Justification for Systematic Review
- Young people have been acknowledged as a special risk population by both the Millennium Development Goals1 and the global goals which have explicitly addressed their unique vulnerability. These goals have been endorsed by the UN General Assembly Special Session on HIV/AIDS (2001).Many HIV control programs have failed to respond to the needs of young people because the data used to develop these programs are not disaggregated by age (FHI 2010). Studies suggest that the fall in the incidence of HIV in some countries could be associated with behaviour interventions (UNAIDS 2001). There are a number of theories and models on how behavioural change comes about. Some common models and theories on which behavioural interventions were built include the Information-Motivation-Behavioural Skills Model (Fisher 2003), the Social Cognitive Theory (Banbura 2001) and Theory of Reasoned Action (Ajzeu 1985). All three theories have different details but produce similar ideas. They all aim to change factors believed to be predictors of behaviour, such as health beliefs, cognitions, attitudes, social skills. This involves the transfer of information to target populations through education, training and counselling which could be done on individual bases or groups. This review is an attempt to examine the efficacy of school-based interventions in developing countries using the global goals of the United Nations General Assembly Special Session on HIV/AIDS for young people (UNGASS 2001) as a reference point. These UNGASS goals are namely;Ÿ To provide young people with access to informationŸ To teach young people skills to avoid them becoming infected with HIVŸ To provide access to servicesŸ To decrease young people’s vulnerability to infectionŸ To decrease the prevalence of HIV among young peopleVarious studies have been conducted on the effectiveness of school-based interventions in knowledge improvements on HIV infection prevention in developing countries (Gallant & Maticka-Tyndale 2004). However, the evidence is unclear as to the effectiveness of school-based HIV interventions meeting these goals. This may be due the difficulty in formulating and measuring outcomes such as skills, vulnerability and HIV incidence (Mufune 2015). Additionally, it may probably be because skills required teaching refusal, negotiation and condom-use are unfamiliar in the school setting in developing countries (WHO 2004). However, in order to notice changes in HIV incidence, schools in developing countries should look at not only making an impact on knowledge alone to demonstrate significance and sustained improvements in sexual risk behaviors but address the more complex affective factors, such as the values, attitudes and perceived norms about sex and condom use, that influence them (Smith et al 2003).Limited reviews of studies have been performed to examined school-based programmes in developing countries and have examined their impact on behavior. Reviews were limited focusing on a particular geographical area or by the strengths of their evaluation and have not examined the characteristics of these programmes in developing countries (Kirby, Laris & Rolleri 2005). A review performed by Kirby, Laris & Rolleri (2005), showed that some characteristics of curriculum-based programmes within the school setting proved to be effective changing young peoples’ behaviors toward sexual activity in both developed and developing countries. However, similar analysis is required for all school-based HIV/STI prevention programmes in developing countries if schools are to fulfill their potential for fighting HIV among youths.
2.1. Description of School Based Programmes
- For the purposes of this review, interventions to improve HIV/STI prevention amongst youths will be referred to as interventions performed in a school setting, which are aimed at educating youths on HIV/STI prevention, and interventions intended to change behaviors, attitudes and practices towards sex among youths within a school setting through single or multiple sessions. Studies, which looked at HIV/STI prevention among a population other than the population selected for this review were not considered. Studies that were school based performed on HIV/STI prevention on a single or mixed gender within the target population for this review were included. Any study which was conducted within a setting other than the school on HIV/STI prevention and focusing on young people were excluded.
2.2. Aim(s)
- This review is to produce synthesis of research evidence on the effectiveness of HIV/STI interventions in schools in developing countries.
2.2.1. Objectives
- The objective of this review is to;Ÿ Identify various school-based interventions aimed at improving youths HIV and STI knowledge. Ÿ Examine school-based interventions that impact on sexual behavior.Ÿ Assess the strength of evaluation design of different study strategies.Ÿ Assess the characteristics of effective interventions
3. Methods
3.1. Criteria for Inclusion and Exclusion
3.1.1. Types of Studies Considered for Inclusion
- The type of studies considered were studies aimed at assessing school-based programmes which were focused on reducing HIV/STI incidence among youths in developing countries. As it is already known to produce a quality review with fewer biases when evaluating the efficacy of an intervention, studies performed with randomised controlled trial (RCT) are known to produce the most reliable results (Sackett et al. 1997). Explicit judgments were made about whether studies were at high risk of bias, according to the criteria given in the Cochrane handbook for systematic reviews of interventions (Higgins 2009). Every effort was made to capture studies performed using randomized control trial (RCT). With this in mind, studies considered for this review were;Ÿ Randomized Controlled Trials and studies performed using cluster-randomized controlled trials comparing either two or more different behavioral interventional strategies were included in this review.Ÿ Controlled Before and After (CBA) Studies where the intervention is compared with no other intervention or alternate interventions were considered.
3.1.2. Type of Participants
- For the purposes of this review, participants selected for inclusion were individuals from age fifteen to twenty-four and actively enrolled in school. There was no restriction on the gender of the participants; studies performed looking at only male, females or mixed gender were considered for inclusion. Studies which compared interventions to prevent the transmission of HIV within an older or younger population were excluded from this review. If studies compared school-based interventions within a population made up of youths and the older population, where possible, only data for the youths were retrieved and included in the review.
3.2. Type of School-Based Interventions
- The types of studies that were included in this review were studies which assessed school-based interventions. For the purposes of this review, schools will be defined as any formal educational establishment, which offer training or education to youths younger than age 25 years. School based interventions can be categorized into three different dimensions which are namely; adult-led versus peer-led interventions, curriculum-based versus non-curriculum-based and interventions with and without characteristics of effective curriculum-based intervention.
3.2.1. Curriculum-Based Verses Non-Curriculum-Based
- Curriculum-based interventions more structured and are often more rigorous than the non-curriculum interventions. Additionally, curriculum-based interventions are mostly based on theories and research which were previously conducted and may have been systematically tested through pilot studies and have been accepted by an authority or the appropriate body. Curriculum is defined in Wikipedia, an online encyclopedia, as “planned interaction of pupils with instructional content, materials, resources, and processes for evaluating the attainment of educational objectives”. It is used as a guide by the educator for effective teaching. It could be said that the curriculum helps the educator to overcome some limitations they may envisage in teaching. This description of a curriculum could improve the efficacy of these interventions. A variety of studies have reported a rise in youth’s knowledge on HIV, STI and condom use in schools where sex education interventions have been introduced (James et al. 2006). Non-curriculum interventions on the other hand, are a range of activities such as individual unstructured counseling on sexual activity and HIV within the school premises plays on HIV/STI stories during school entertainment sessions and the use of posters or leaflets or a blend of both. A number of these activities may be less complicated to implement in educational settings because there is no cost involved and they do not need any training for the teacher. Kirby et al (2005a) recommend that unstructured individual communication between youths and teachers could be more efficient considering the private nature of the discussing sexual behavior. These types of interventions need some level of empathy, skill and sensitivity outside the range of many implementers.
3.2.2. Interventions with and without Characteristics of Effective Curriculum-Based Intervention
- Different characteristics of interventions can affect their effectiveness, especially the curriculum-based interventions. Examples are the focus of activities, the provision of information and the teaching methods used in curriculum-based interventions. In developing countries, at least 65 evaluations of curriculum-based education HIV education interventions have been conducted, this includes some studies of non-curriculum-based interventions. Studies reviewed have identified that some of the characteristics of interventions are believed to be important in producing behavioral change (Kirby 2005). Even though these characteristics of effective interventions have not been taken from interventions used originally in developing countries, they still present a potential strategy which can be used to measure these interventions in developing countries. In their review, Kirby et al (2005) identified some of these characteristics which were based on greater number of studies and includes some studies from developing countries. The review identified 17 characteristics that appeared to differentiate efficient programmes which described programme development, the curriculum and the implementation of the programme.
3.2.3. Adult-Led Versus Peer-Led Interventions
- Adults are mainly the implementers of curriculum-based interventions, mainly because they have more experience, knowledge and skills needed. Adults who implement any specific curriculum may involve school teachers and health workers. Interventions lead by teachers are the said to be logistically the easiest to implement in educational settings once a teacher has been sufficiently trained, such interventions are most of the time replicable (Ross, Dick & Ferguson 2006). However there are some limitations to these teacher-led interventions, that is, their discomfort in using interactive teaching methods and discussing sensitive topics such as adolescents’ sexual behavior.Due to these limitations most communities favor using community health workers or other local experts to teach these subjects. These experts may know more about the subject area and more confident discussing these topics. However, due to the inadequacy of infrastructure, transportation, time and other resources may hinder health workers from providing effective teaching to many students in many schools. The use of peer educators as alternative to teachers or other adults have been advocated widely have (UNAIDS 1999). There is the belief that peer educators are able to communicate better with other young adults than older adults. However, peers are likely to be unfamiliar with these topics and unlikely to possess the requisite skills required to teach curriculum activities (Irvin 2000). Additionally, the expected yearly student turnover and subsequent requirements for frequent training and supervision raise doubts about whether it is sustainable and cost-effective to use peer educators (James-Traore et al 2004).
3.3. Study Setting
- Due to the age of the participants for this review, only studies performed in primary, secondary and vocational schools settings were considered in this review. All other studies focused on youth HIV/STI prevention in developing countries performed outside the school setting were excluded. According to the World Bank classification (2004), developing countries are countries with low or middle levels of gross national product per capita.
3.4. Types of Outcome Measures
- The reviewer considered both primary and secondary outcomes measures in selecting studies for inclusion.
3.4.1. Primary Outcome Measure
- Studies reported outcome measures;Ÿ Increase/Decrease of HIV KnowledgeŸ Increase/Decrease in sexual activityŸ Changes in behavior and attitudes
3.4.2. Secondary Outcome Measure
- Ÿ Increase/Decrease in condom useŸ Increase/Decrease in Abstinence
3.5. Methods Used to Identify Studies for Inclusion
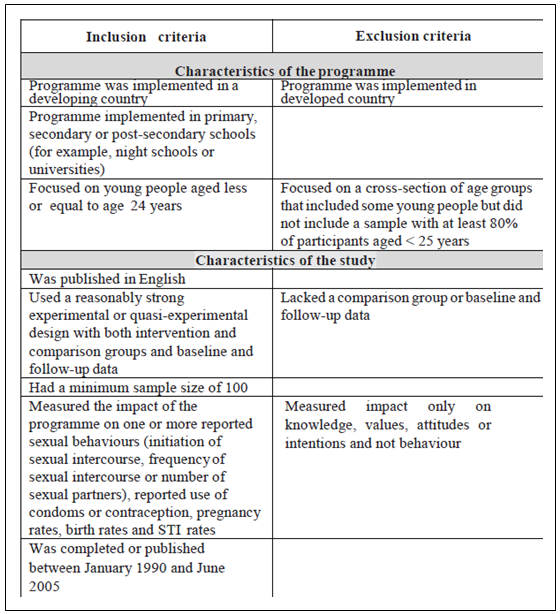
- Studies identified that sought to meet the criteria for inclusion and exclusion as shown in Table 2 were retrieved. The review was restricted to studies which evaluated an intervention’s effects on behavior. The reasons for this restriction are firstly, it is well-known that school-based HIV interventions can enhance knowledge, all studies that evaluated impact on knowledge found a positive impact. The secondly, changes in knowledge, skills and other mediating aspects will not contribute to a decline in HIV/STI prevalence if behavior also changes.
|
3.6. Search Strategy
- The incidence of HIV peaked in the 1990’s and saw a decline from 2005. What was done to prompt the decline? To answer this question selecting studies between 1990 and 2005 were appropriate to assess whether the drop in HIV incidence in developing countries was as a result of education interventions. Studies from 1990 effectively gave a clearer explanation of whether education interventions contributed to the decline in 2005. In addition to assessing HIV incidence, the reviewer also included studies performed on sexually transmitted infections (STIs) as knowledge on STI prevention could lead to preventing HIV transmission.To identify and retrieve relevant studies that met the criteria for inclusion the search terms used were based on Medical Subject Headings (Mesh) to capture articles relating to HIV/STIs and their prevention among youths or young people published from 1990 to 2005.To prevent a publication bias, a broad search strategy was employed to identify all the related studies irrespective of their publication status. In addition, reference lists, academic studies and publications from government and non-governmental departments were targeted. Finfgeld-Connett (2008) explains publication bias as a situation where studies selected to be included in a review may not be representative of the true intervention effect.
3.6.1. Electronic Searches
- Studies were selected using various databases namely; Medline, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), POPLINE and CINAHL.
3.6.2. Searches from Other Sources
- In addition the following sources were also searched;Ÿ Reference lists of relevant papers for additional citationsŸ A Family Health International (FHI) 360 Library catalogue for relevant project reports.
4. Data Collection and Analysis
4.1. Selection of Studies
- Assessments of studies for inclusion were performed by reading through all titles and abstracts identified during the initial search. Due to the purposes of this study, search results were examined for potential eligibility for inclusion solely by the reviewer. This made it difficult for the reviewer to make decisions when there were discrepancies in study selection which could lead to a selection bias. Studies which were identified and selected in the first screening were further assessed to establish relevance and whether the full article should be retrieved. To reduce the amount of a selection bias, when there was difficulty in making a decision on the eligibility of a study, the full text was retrieved and read thoroughly before a final decision was made. Studies were screened for eligibility based on the following; study design, the intervention, participants and the outcome measures. Studies which were found to assess school-based interventions on HIV or STI prevention among youths were included. Studies which examined HIV transmission in an older population than the study population were also excluded. The reviewer screened references provided in studies included for eligibility.The data abstraction form used for extracting data for this review was adapted from the Cochrane Effective Practice and Organization of Care. The information extracted from the studies included were country of study, intervention focus, description of participants, description of intervention, quality of delivery and statistical methods, study outcome measure. Data collected from the studies that met the criteria for this review were managed on an excel spreadsheet which was prepared by the review.
4.2. Methodological Quality
- The assessment of the methodological quality for this review was performed using an up-to-date risk of bias criteria tool for randomized controlled trials (RCTs), non-randomized controlled trials (NRCTs) and controlled before and after (CBA) studies prepared by Cochrane Effective Practice and Organization of Care (EPOC, 2009). Yes, No and Unclear were used as scores to indicate whether studies included had clearly indicated the following; study design, sequence generation, allocation concealment, baseline outcome measurement similar, baseline characteristics similar, incomplete outcome data, knowledge allocated intervention, adequate protection against contamination, free from selective outcome reporting and other sources of bias. Eleven CBAs and six RCTs were scored “No” and “Yes respectively in “sequence generation”. The score for “adequate allocation concealment” for six CBAs in the review were scored “No” and five scored “Yes”, five out of the six RCTs included in the study were scored “Yes” and the remaining one scored “No”. Six RCT studies scored “Yes” for “baseline measurement similarities” and CBAs scores were 9 and 2 for “Yes” and “Unclear” respectively. The number of studies scored “Yes” for “similarities of baseline characteristics” was fourteen and the remaining three were scored “No”. Out of the seventeen included studies, thirteen adequately dealt with “incomplete outcome data” and thus were scored “Yes”, one was scored “No” and the rest were scored “unclear” as this was not clearly addressed. “Knowledge allocated interventions” was scored “Yes” for fourteen studies, “No” for one study and two studies were scored “unclear”. Efforts were made to avoid contamination in fifteen studies which were scored “Yes”; One study scored “No”, because the possibility of the control receiving the intervention was high and the other was scored “Unclear” as it wasn’t clearly stated how contamination was controlled. All the studies selected for inclusion had no selective outcome reporting.
4.3. Review of Studies Selected for Inclusion
- All studies included for this review were summarized in a table created by the reviewer. Reported outcomes in studies included, for example, effects on behavior were measured significant if they were statistically significant at the p< 0.05 level. This significance was based either on the entire sample or a sub-sample that was approximately one third of the overall sample or larger (for example, sexually inexperienced youths or youths younger or older than a certain age or sexually experienced or males or females). Some studies establish a significant effect for important sub-groups but not for the total sample. Some studies reported results for several measures of behavior at different time periods, for different sub-groups. To provide a more balanced overview and avoid presenting only the positive results, rules were adopted for summarizing the results. First, all measures of similar outcome behavior: every measure across all the studies was rank-ordered according to their likely impact on incidence and prevalence. For example, the condom use over an extensive period of time was scored higher than condom use at first sexual intercourse. The reviewer included in the study only results which reported the highest ranked measures in the tables. Second, because short-term effects on behavior would have a slight impact on HIV prevalence, only those results reported for periods of 3 months or longer were included in the tables. In addition, since studies were not likely to have enough statistical power to assess the impact on those behaviors or outcomes that change gradually, that is, initiation of sex, pregnancy rates or rates of sexually transmitted infections, only those results assessing impact on these outcomes for at least 6 months were included.
5. Results
5.1. Characteristics of Interventions Included
- Searches identified a total of 17 studies which met the inclusion criteria. Studies performed in foreign languages were excluded due to time constrains in translating them into English. No additional information was requested from authors of studies included due to the time constrains. Among the interventions that were identified in the 17 studies selected for inclusion, 12 were curriculum-based and 5 were non-curriculum based.Mainly adults taught another 11 of the 12, and only 1 was taught exclusively by peers. Among the 11 interventions taught by adults, school teachers taught 9 and other adults, such as health workers, qualified counselors and facilitators, and young adult volunteers, taught the remaining 3. However, among the 12 interventions taught by adults, 1 also included peer educators significantly. The remaining five non-curriculum-based interventions were mainly facilitated by teachers or other adults. A total of 11 of the interventions assessed had been performed in secondary schools; four had been performed in primary schools; and two had been performed in night schools or teacher training colleges.
5.2. Characteristics of Studies Included in Review
- A total number of 6 studies used an experimental design and the remaining 11 used a quasi-experimental design. To be included in this review, quasi-experimental designs had to have both an intervention and comparison group and both pre-test and post-test. The analyses of statistics in studies selected for this review varied from moderately acceptable to rigorous. For example, a small number of studies assessed whether the intervention and control group were statistically dissimilar at baseline and then at follow up used a different test to assess whether there was a significant difference over a period of time between the intervention and the control group. Others did not statistically have power over the background characteristics that may have been associated with outcome behaviors. An entire school was assigned to intervention group by others but did not control for clustering. It was difficult to access the overall effects of limitations in the statistical analyses. Fortunately, a small number of studies which were part of the studies selected for this review used very thorough statistical analyses.
5.3. Impact on Prevalence and Sexual Behavior
5.3.1. HIV/STI Prevalence
- Preferably, studies selected would have evaluated the intervention’s impact on the incidence or prevalence of HIV/STI. But, just one study with the largest sample size, assessed the impact of STIs/HIV prevalence. This study was a randomised controlled trial conducted in Mwanza, Tanzania (Ross et al 2005), which established that the “MEMA kwa Vijana” (“Good things for young people”) interventions had no significant effect on the occurrence of STIs such as syphilis, genital herpes or Chlamydia among either boys or girls. Additionally, it did not show a significant result on the prevalence of trichomoniasis and gonorrhoea among girls, these were not measured among boys in the study. But there was a small but significant negative effect found on the prevalence of gonorrhoea among girls.
5.3.2. Impact on Behavior
- Due to the process used in selecting the relevant studies for this review, all included studies assessed the effects on one or more reported sexual behaviors which could affect HIV/STI incidence in the long run. Patterns of reported outcomes presented were relatively similar, regardless of the type of intervention or evaluation design.
5.3.3. Sexual Behavior
- Studies used for this review presented strong evidence that HIV and STI education interventions will not result in increased sexual behavior but rather significantly reduced one or various types of sexual activity. Initiation of sex was measured in 12 of the included studies; only Brieger et al (2001) used a non-curriculum-based peer-led intervention which found in the intervention group a significant increase in the initiation of sex compared to the control group. The remaining 11 interventions did not report anything on the initiation of sex, but delayed initiation was significant 7 studies.Reported frequency of sexual engagement was the other common measure of sexual activity. This measure comprises both the total number of sexual activity performed by the participants during a particular number of months before the study and whether participants engaged in any sexual intercourse during this period: it thus assesses the likely return to secondary abstinence, defined as abstaining from further sex before marriage for those who already have sexual experience. This assessment is imperative for the prevention of unwanted pregnancy and STIs/HIV. Overall, only eight studies assessed the impact on the reported occurrence of sexual activity, none of these studies reported an increase in sexual activity but three studies reported a decrease in frequency of sexual activity. The reported number of sexual partners was the last measure of sexual activity. This measure is particularly important for avoiding the spread of HIV. There were no increases in the reported number of sexual partners, but 3 out of 8 interventions reported a reduction in the number of partners.
5.3.4. Impact on Use of Condoms and Contraceptives
- In total, fourteen studies assessed the impact on reported condom use, no studies found a decrease in the use of condoms, but six studies reported a significant rise in condom use. This may probably due to the large sample sizes of these studies compared to the other eight. Although other contraceptive methods apart from condoms do not evidently prevent the transmission of HIV, most of these interventions were on sex education which encouraged contraceptive use to prevent teenage pregnancy as well preventing STIs and HIV through the use of condom. Out of four studies that assessed on reported contraceptive use, three reported a significant increase in contraceptive use. Two studies looked at the impact on measures of unprotected sex which included frequency of sexual activity reported or number of partners and the frequency of condom use. A positive impact was found in one study.
5.3.5. Changes in One or More Behaviors
- Out of 17 interventions, 11 reported an encouraging impact on one or more of the behaviors and two or more positive impacts on behaviors were reported by 5 interventions. However, two had no significant effect on any reported behavior. In general, all 17 interventions established a significant positive change in 21 of 50 measures in reported sexual behavior in all studies.
5.3.6. Summary of Behavior Effects
- In summary, most studies presented enough evidence to suggest that school-based HIV/STI education interventions did not result to a rise in sexual activity, but rather some interventions had encouraging outcome on both reported sexual and protective behaviors measured. There is a possibility that some school-based interventions could delay reported sexual activity, reduce the number of sexual partners, reduce the number of reported of sexual activity or increased condom use or contraceptive use and thereby reducing the incidence of unprotected sex among youths.Additionally, about half of adult-led interventions in all three categories had a positive effect on at least one of the reported sexual or protective behaviors. Out of the three peer-led interventions two showed one or more behaviors that had a positive impact on participants. These results have established that there is no one type of intervention that is effective, but generally they have the possibility to be effective in some circumstances. Full discussions of these interventions are can be found below.
5.4. Impact on Psychosocial Factors Affecting Behavior
5.4.1. Knowledge
- Out of the 17 studies, ten assessed the intervention’s effects on knowledge. All 10 studies indicated that certain interventions could increase knowledge about one or more subjects which included STIs/HIV and their prevention. Knowledge on all items measured was not improved by the interventions; this may be probably because some curriculum did not focus on some specific details. However, all interventions identified in studies showed a positive change in knowledge on one or more details relating to HIV/STI prevention which resulted in a change in one or more outcome measured. This change among youths could suggest that knowledge of HIV/STI could have some positive impact on sexual activity. These findings were similar with the results from developed world that had continually indicated that there is a significant chance that HIV/STI education interventions and school-based sex education could improve knowledge about sexuality, just as classes in a particular subject could increase knowledge about that particular subject or topic. Topics on sex education and HIV/STIs are often of great interest and relevance to the lives of students, they are often very effective way in increasing students’ knowledge.
5.4.2. Reported Values, Attitudes, Peer Norms, Skills, Intentions and Other Risk and Protective Behaviors
- The skills identified in the United Nations General Assembly Special Session goal number 2, are one of many psychosocial factors required to successfully transform the behavior of youths. Fourteen studies assessed interventions effect on sexual and psychosocial factors, for example, individual values and awareness of peer norms or other behaviors, such as discussions about sex and condoms or alcohol use, that are recognized to be linked to protective behaviors and sexual risk. These results were not as reliable as they were for knowledge.These results indicated that interventions did not affect these factors negatively, and about half produced positive effects. Some studies found that their interventions positively changed reported values about sex, values on someone being given pressure to have sex, attitudes towards people living with AIDS, attitudes towards condoms, perceptions of peer norms regarding condoms, self-efficacy to obtain condoms and to use condoms, self-efficacy to say no to have sex and plans to talk about condom use or to use a condom. The intention to abstain from sex or reduce number of sexual partners that were measured in three of the studies suggests that the interventions could increase these intentions. A decrease in the use of alcohol and drugs was found in one intervention. One of the studies establish the intervention that encouraged youths avoid situations that could lead to sex; and a final study establish that its intervention raised the percentage of young people who reported having purchased condoms. Results from these 17 studies assessing effects on reported behavior were also backed by findings reported by other studies that assessed impact on attitudes, values and norms but did not assess effects on behavior. Six of such studies reported that school-based interventions enhanced a number of these reported attitudes, values, intentions or norms (Aplasca et al 1995; Caceres et al 1994; Kuhn, Steinberg & Mathews 1994; Singh 2003; Visser 1996 and Kim 2005).
5.5. Strength of Evidence for Curriculum-Based Adult-Led Interventions
- In total, six types of interventions on behavior were identified, out of the six interventions, five reported encouraging behavioral results, and a strong evidence of positive effect on behavioral change identified in one intervention.There was strong evidence for three reasons: firstly, the number of studies within that category was large; secondly, evidence of the strength for some individual studies were much stronger than some other studies in other categories; and finally, a positive impact on behavior was consistent among interventions. Significant behavioral changes were identified in 11 interventions; only 2 did not produce a significant change in behavior. However, in one those two interventions, the control group reported 17% on initiated sex compared the intervention group which reported only 7% (Klepp et al. 1997). Even though this could have been programmatically important, the results were not statistically significant. Eggleston et al. (2000), similarly report results that were not significant, contraceptive usage indicated an odd ratio of 2.25 (P = 0.08). These were the only two studies which did not report on the benefits on behavior being statistically significant. Although in some interventions the positive effect lasted only for a few months, other lasted for years. An example is the MEMA kwa Vijana intervention which identified, over a 36 month period, positive effects on reported behaviors (Hayes et al 2005). These positive effects produced by these interventions were highly significant in this study. Similar proportions of interventions were identified to be efficient irrespective of where they were implemented, either in a primary or secondary school or in a college setting.Generally, curriculum-based interventions identified to have been taught by teachers or other adults were seen to be more effective. The intervention was found to be effective for both male and female students. Interventions which resulted to an increase in reported use of condoms among females were encouraging, as women have little access to control their use. These interventions were effective irrespective of the type of design used in evaluating them, whether with experimental or quasi-experimental designs. The overall patterns of results of the interventions found in developing countries were similar to those from the United States and other developed countries (Kirby; Laris and Rolleri 2005). Interventions that were school based demonstrated that encouraging condom use and abstinence among youths did not result to an sexual behavior, but could result in reducing the occurrence of sexual relations among youths, delaying youths sexual activity, reducing the number of sexual partners and encourage them to use condoms or contraceptives. Additionally, the positive effects of such interventions were demonstrated in some studies as quite robust (Kirby, Laris and Rolleri 2005; Kirby D. 2001). This is encouraging and could mean that the level of economic development and the incidence of HIV could not have any adverse effect on the effectiveness of the interventions used.
5.5.1. Characteristics of Curriculum-Based Adult-Led Interventions that Changed Behavior
- As previously mentioned above, the reviewer coded each study using the characteristics of interventions (Kirby, Laris and Rolleri, 2006) which has been proven to be useful in any part of the world. So the question is: In developing countries what are the characteristics of an effective school-based programmes? After the coding, results indicated that interventions had very similar characteristics as successful curricula assessed in any part of the world. However, this may be partly because of the restrictions of studies, the reviewer was not able establish whether three particular characteristics were included. In particular, to decide whether the developer of the programme applied logic model to develop programmes was often complicated, whether a pilot study was performed on curriculum activities before implementation or whether a safe environment was created by educators for group discussions in the classrooms.
5.5.1.1. Health Services
- Schools may have a significant role in reaching the United Nations General Assembly Special Sessions goal for improving access to health services for youths in the developing countries. However, full evaluation of this issue is beyond the range of this review.
5.6. Discussion
- Given that all curriculum-based programmes in this review that assessed effects on knowledge established an increase in knowledge, knowing that various studies of curriculum-based programmes in developed countries have also established that knowledge can be increased by these programmes, school-based programmes have evidently demonstrated an impact of on knowledge levels among studies reviewed.As already mentioned in this review, curriculum-based interventions which incorporated a majority of the characteristics described by Kirby, Laris and Rolleri, (2006) were adult-led which had been assessed by a most of the studies and had produced strong evidence. They had reliable results representing a positive description of behavioral change. These outcomes are all based on behaviors that were reported, which included, the limitations of sexual behavior which were self-reported, it also includes the possibility for presentation bias that may take place, mainly within the framework of interventions promoting particular behaviors. As a result, a positive change on actual STI or HIV incidence among youths is more reliable. However, the reliability of the positive changes on reported sexual behaviors in studies reviewed is encouraging. The results also suggest that interventions have demonstrated some evidence of effectiveness in behavioral change.Studies reviewed suggested that curriculum-based programmes were effective when they had the following characteristics a) when participants’ needs were assessed before the intervention. b) Interventions were led by adults, and c) the intervention was conducted in the appropriate environment, such as the classroom. Among all these studies that assessed curriculum-based adult-led interventions, only one study with a quasi-experimental design indicated a positive change on sexual risk behavior and another study with the same design showing no change. The evidence in these interventions demonstrates some form of effectiveness, but the findings are weak. Interventions may require additional development, pilot testing and evaluation.Some of the interventions identified were called life-skills interventions. However, life-skills interventions not included in this study educated youths on only a wide-ranging of social skills or life-planning skills. They did not make sexual behavior the focus, the message on sexual behavior was not clearly stated and they did not included some of the other characteristics described in chapter 3 of this review. Very few of these interventions have been assessed. These interventions demonstrated some evidence of effectiveness but were not strong enough. Perhaps further development and testing could demonstrate effectiveness. Primarily, peers implemented only two curriculum-based interventions of which one indicated a rise in the use of condoms among youths, the second intervention failed to include these characteristics which may have resulted in the change behavior not being significant. These two interventions also demonstrated some evidence that the intervention could be effective, but needed some further assessment. Non curriculum-based interventions did not produce clear results. Out of five non curriculum-based interventions, four were adult-led. Two out of the four adult-led non curriculum-based interventions produced positive effects on various behaviors, whiles the other two did not. Out of the four adult-led interventions, only one was assessed in a randomized trial and could not find an impact on behavior. These studies did not demonstrate sufficient evidence of effectiveness probably due to the limited number of studies.The last non curriculum-based intervention, which is the fifth, was peers-led. This intervention’s results indicated very important positive behavioral changes, such as, increased condom use, having fewer sexual partners and increased use of contraception; the results also included one negative behavioral aspect, which is, speeding up of the initiation of sexual activity. These results provide convincing evidence that curriculum-based compared with non-curriculum based interventions on HIV and STI education do not lead to an increase in reported sexual activity, but rather, it is effective in increasing knowledge on preventative methods and condom use, reduces risky sexual behaviors and delays the initiation of sexual activity. This conclusion is mainly for adult-led interventions which were particularly strong and consistent. With these changes in sexual behavior, one could anticipate a decrease in both unwanted pregnancy and sexually transmitted infections (STIs), but, only one study assessed an intervention’s impact on the rate of STIs which produced no positive significant effects (Hayes et al, 2005). This may partly be because the participant sample sizes were not representative enough to identify programmatically significant effects on bacterial STIs and HIV. However, there was sufficient power to estimate the effects of the intervention on infection rates associated with pregnancy and herpes simplex virus–type 2. The intervention produced no impact on biomedical outcomes even though it had showed convincing evidence for effects on reported sexual behaviors. A better understanding of this displacement between reported effects on behavior and the lack of biomedical impact is clearly significant. More studies need to assess an intervention’s impact on STIs rates and pregnancy. None of the studies used for this review included any cost effectiveness analyses. If risky sexual behavior is reduced effectively by programmes then there is the potential of these programmes to be cost effective. To develop an effective curriculum based intervention, teachers have to be trained and this can be expensive. Once teachers are trained, they must implement the programmes in the classrooms; this time in the classroom carries a cost. On the other hand, once effective curricula designs have been established, training of all new teachers can be included so that they can effectively implement the programme. In addition, the duration of these curricula is short, the longest is usually 28 hours, and this makes the cost of the time spent in the classroom reasonably modest. Finally, to implement such programmes relatively few materials are required.Potentially, primary and secondary schools or colleges in developing countries do have a major role to play in dealing with youth’s vulnerability to early sexual activity in different ways; examples are, at the personal level, developing youth life skills during their education and at the community level, by dealing difficult gender norms leading to increasing changes in norms and morals. However, it is also known that the schools themselves could lead to youth vulnerability by exposing young girls to sexual abuse by their teachers (James-Traore et al 2004; Gachuhi 1999 and Schapink, Hema, Mujaya 1997) and by supporting unfavourable practices between both sexes. However, reviewing these effects is outside the parameters of this review.
5.7. Limitations to the Study
- There were a large number of studies on HIV prevention focusing on young people, but were excluded due to the type of design. This resulted in having only 17 studies to review, which may result in losing vital information which could have been beneficial to this review. Normally, systematic reviews are conducted by two or more people each playing a different role in selecting studies and making decisions on discrepancies; this review was conducted by one person due to its purposes which may have resulted to the review overlooking important information. This may exposed the review to a reporting bias and other biases which may affect the results. To reduce or avoid these biases uses two or more reviewers will be more appropriate. The review also identified many studies on school-based HIV/STI prevention programs in developing countries, but the problem is most of the studies identifies either had a small sample population which could not be representative of the true population and thus affect the results for this review or the study design used did not meet the criteria. This reduced the number of studies reviewed for this study. The reviewer did not have access to some studies due to accessibility. These were studies which demanded payment before downloading. This resulted in the reviewer missing information from studies which were relevant to the review. Finally, due to the language restrictions, studies conducted in other languages apart from English were excluded. This could result in a section bias and thus leading to a possible exclusion of vital information.
6. Conclusions and Recommendations
- The studies reviewed had showed some positive results with regards to the effectiveness of increased knowledge; this suggests that most HIV and sex education interventions incorporated into the school curriculum could be effective in developing countries considering its success in developed countries. With regards to changes in reported behavior, this review suggests studies have demonstrated sufficient evidence that curriculum-based interventions led by adults are highly effective. All other types of interventions identified produced weak evidence of effectiveness for reported behavioral change. Similar patterns of results were found across both developing and developed countries which is encouraging.Even though so far studies have not established that these interventions significantly reduced STIs and HIV rates in developing countries, various studies established that their intervention found encouraging changes in behavior that could lead to a decrease in STIs and HIV in the long term. Further research with more rigorous designs will be needed to examine the long-term positive effects of sex and HIV education interventions on stronger outcomes such as reducing STI incidence/prevalence and most importantly reducing HIV incidence/prevalence among youths in developing countries. Given that there is some evidence of efficacy on curriculum based interventions on HIV/STIs in developing countries and that there is no evidence that these interventions are harmful, it would be useful to introduce more of such interventions in developing countries. This will enable young people to have the knowledge and the behaviours to be more responsible and control of the lives. From the studies reviewed, there is enough evidence to suggest that effective Curriculum Based Education is the key to increasing knowledge and changing behaviours of young people. Educational institutions are key settings for educating children on HIV and STI prevention for halting the further spread of the infection. Success in carrying out this function depends upon reaching children and young adults on time to reinforce positive health behaviours and alter the behaviours that place young people at risk.2It is important that governments and other stakeholders aim at investing in training teachers in schools to train teachers to promote these sexual health interventions for young people in developing countries. Currently, medical researchers seem to focus more on cure than prevention. There is also the need to have a well design school based HIV/STI programmes in the developing countries, if possible they should be conducted using randomised controlled trials. Samples included in such studies should be very large to measure effectively the interventions impact on HIV/STIs among young people.
Notes
- 1. http://www.un.org/en/mdg/summit2010/pdf/ZeroDraftOutcomeDocument_31May2010rev2.pdf 2. http://www.ibe.unesco.org/AIDS/doc/prac09e.pdf
References
| [1] | Agha, S., Van Rossem R. (2004), Impact of a school-based peer sexual health intervention on normative beliefs, risk perceptions, and sexual behaviour of Zambian adolescents. Journal of Adolescent Health, 34:441-452. |
| [2] | Antunes, MC et al. (1997), Evaluating an AIDS sexual risk reduction program for young adults in public night schools in Sao Paulo, Brazil. AIDS, 11 Supplementary 1:S121-127. |
| [3] | Ajzen, I. (1985), From intentions to actions: A theory of planned behaviour. In J. Kuhl & J. Beckmann (Eds.), Action-control: From cognition to behaviour pp. 11–39. Heidelberg, Germany: Springer. |
| [4] | Bandura, A. (2001), Social cognitive theory: An agentic perspective. Annual Review of Psychology, 52, 1–26. |
| [5] | Baker, S et al. (2003), Evaluation of a HIV/AIDS program for college students in Thailand. Washington, DC, Population Council. |
| [6] | Blum RW, Mmari KN. (2004), Risk and Protective Factors Affecting Adolescent Health in Developing Countries. Geneva: World Health Organization, Broadening the Horizon. |
| [7] | Boonstra, H. D (2011), Advancing Sexuality Education in Developing Countries: Evidence and Implications. Guttmacher Policy Review; Vol. 14 Issue 3, p17. |
| [8] | Brieger, WR et al. (2001), West African Youth Initiative: outcome of a reproductive health education program. Journal of Adolescent Health, 29:436-446. |
| [9] | Cabezon, C et al. (2005), Adolescent pregnancy prevention: An abstinence-centred randomized controlled intervention in a Chilean public high school. Journal of Adolescent Health, 36:64-69. |
| [10] | Caceres, CF et al. (1994), Evaluating a school-based intervention for STD/AIDS prevention in Peru. Journal of Adolescent Health, 15:582-591. |
| [11] | EPOC, (2009), Cochrane Effective Practice and Organisation of Care Group. http://epoc.cochrane.org/epoc-resources Accessed 17.12.2015. |
| [12] | Eggleston, E et al. (2000), Evaluation of a sexuality education program for young adolescents in Jamaica. Revista Panamericana Salud Pública, 7:102-112. |
| [13] | Family Health International, (2010), Young People Most at Risk of HIV: A Meeting Report and Discussion Paper from the Interagency Youth Working Group, U.S. Agency for International Development, the Joint United Nations Programme on HIV/AIDS (UNAIDS) Inter-Agency Task Team on HIV and Young People, and FHI. |
| [14] | Fawole, IO et al. (1999), A school-based AIDS education programme for secondary school students in Nigeria: a review of effectiveness. Health Education Research, 14:675-683. |
| [15] | Fisher, W. A., Fisher, J. D., & Harman, J. J. (2003), The information, motivation, behavioural, skills model as a general model of health behaviour change: Theoretical approaches to individual-level change. In J. Suls, & K. Wallston (Eds.), Social psychological foundations of health (pp. 127_/153). London: Blackwell. |
| [16] | Gachuhi, D. (1999), The impact of HIV/AIDS on education systems in the eastern and southern african region and the response of education systems to HIV/AIDS: education/life skills programmes. Nairobi, UNICEF/East and Southern Africa Region. |
| [17] | Gallant M, Maticka-Tyndale E. (2004), School-based HIV prevention programmes for African youth. Social Science and Medicine, 58:1337-1351. |
| [18] | Grunseit, A et al. (1997), Sexuality education and young people’s sexual behaviour: a review of studies. Journal of Adolescent Research, 12:421-453. |
| [19] | Grunseit, A. (1997), Impact of HIV and sexual health education on the sexual behaviour of young people: a review update. Geneva, UNAIDS. |
| [20] | Harvey, B., Stuart J, Swan T. (2000), Evaluation of a drama-in-education programme to increase AIDS awareness in South African high schools: a randomized community intervention trial. International Journal of STD and AIDS, 11:105-111. |
| [21] | Hayes, et al. (2005), Community randomised trial of an innovative adolescent sexual health intervention programme in rural Tanzania: the MEMA kwa Vijana trial. Aug; 26(4):430-42. |
| [22] | Higgins, JPT, Green S. (2009), Cochrane handbook for systematic reviews of interventions version 5.0.0 (updated 2009). Wiley-Blackwell. |
| [23] | Irvin, A. (2000), Taking steps of courage: teaching adolescents about sexuality and gender in Nigeria and Cameroon. New York, International Women’s Health Coalition. |
| [24] | James-Traore, T et al. (2004), Teacher training: essential for school-based reproductive health and HIV/AIDS education: focus on sub-Saharan Africa. Arlington, VA, FHI, YouthNet Program. |
| [25] | James-Traore, T et al. (2002), Intervention strategies that work for youth: summary of FOCUS on young adult’s end of program report. Arlington, VA, Family Health International, Youth Net Program. |
| [26] | James, S., P. Reddy, R.A.C. Ruiter, A. McCauley, and B. van den Borne. (2006), The impact of an HIV and AIDS life skills program on secondary school students in KwaZulu-Natal, South Africa. AIDS Education and Prevention 18, no. 4: 281–94. |
| [27] | Kim, H. (2005), The effects of sex education programs on knowledge and attitude related to sex of elementary school high grade students. (Unpublished data presented at 16th World Congress of Sexology). |
| [28] | Kinsler, J et al. (2004), Evaluation of a school-based intervention for HIV/AIDS prevention among Belizean adolescents. Health Education Research, 19:730-738. |
| [29] | Kirby, D. (2001), Emerging answers: research findings on programs to reduce teen pregnancy. Washington, DC, National Campaign to Prevent Teen Pregnancy. |
| [30] | Kirby, D, Laris B, Rolleri L. (2005a), Impact of sex and HIV education programs on sexual behaviours of youth in developing and developed countries. Washington, DC, Family Health International, pp. 1-45. |
| [31] | Kirby, DL, Ryan G. (2005), Sexual risk and protective factors – factors affecting teen sexual behaviour, pregnancy, childbearing and sexually transmitted disease: Which are important? Which can you change? Washington, DC, National Campaign to Prevent Teen Pregnancy. |
| [32] | Klepp, KI et al. (1997), AIDS education in Tanzania: promoting risk reduction among primary school children. American Journal of Public Health, 87:1931-1936. |
| [33] | Kuhn, L., Steinberg M, Mathews C. (1994), Participation of the school community in AIDS education: an evaluation of a high school programme in South Africa. AIDS CARE, 6:161-171. |
| [34] | MacPhail, C and Campbell C. (1999), Evaluating HIV/STD interventions in developing countries: do current indicators do justice to advances in intervention approaches. South African Journal of Psychology, 29:149-165. |
| [35] | Mufune, P (2015) Poverty and HIV/AIDS in Africa: Specifying the connections. Social Theory & Health 13, 1-29 (February 2015) | doi:10.1057/sth.2014.14. |
| [36] | Martinez-Donate, AP et al. (2004), Evaluation of two school-based HIV preventions. |
| [37] | Interventions in the border city of Tijuana, Mexico. Journal of Sex Research, 41:267-278. |
| [38] | Maticka-Tyndale, E et al. (2004), Primary School Action for Better Health: 12-18 month evaluation. Final Report on PSABH Evaluation in Nyanza and Rift Valley. Windsor, Ontario, University of Windsor. |
| [39] | Mbizvo, MT et al. (1997), Effects of a randomized health education intervention on aspects of reproductive health knowledge and reported behaviour among adolescents in Zimbabwe. Social Science and Medicine, 44:573-577. |
| [40] | McCauley, AP. (2004), Programming for HIV prevention in Mexican schools. Washington, DC, Population Council. |
| [41] | Munodawafa, D., Marty PJ., Gwede C. (1995), Effectiveness of health instruction provided by student nurses in rural secondary schools of Zimbabwe: a feasibility study. International Journal of Nursing Studies, 32:27-38. |
| [42] | Murray, N et al. (2000), An evaluation of an integrated adolescent development program for urban teenagers in Santiago, Chile. Futures Group International, Centre for the Reproductive Health of Adolescents, Johns Hopkins University. |
| [43] | Okonofua, FE et al. (2003), Impact of an intervention to improve treatment-seeking behaviour and prevent sexually transmitted diseases among Nigerian youths. International Journal of Infectious Diseases, 7:61-73. |
| [44] | Oshi DC, Nakalema S, Oshi LL. (2005), Cultural and social aspects of HIV/AIDS sex education in secondary schools in Nigeria. Journal of Biosocial Science, 37:175-183. |
| [45] | Pedlow, CT, Carey MP. (2004), Develop mentally appropriate sexual risk reduction interventions for adolescents: rationale, review of interventions, and recommendations for research and practice. Annals of Behavioural Medicine, 27:172-184. |
| [46] | Perez, F, Dabis F. (2003), HIV prevention in Latin America: reaching youth in Colombia. AIDS CARE, 15:77-87. |
| [47] | Pick De Weiss, S. Givaudan M, Givaudan S. (1993), Planeando tu vida: sex and family life education. Fundamentals of development, implementation, and evaluation. International Journal of Adolescent Medicine and Health, 6:211-224. |
| [48] | Reddy, P., James S, McCauley AP. (2003), Programming for HIV prevention in South African schools: a report on program implementation. Cape Town, USAID and Population Council. |
| [49] | Reddy, P., James S, McCauley AP. (2003), Programming for HIV prevention in South African schools: horizons research summary. Washington, DC, Population Council. |
| [50] | Resnick, MD et al. (1997), Protecting adolescents from harm: findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278:823-832. |
| [51] | Robin, LD et al. (2004), Behaviour interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: a decade in review. Journal of Adolescent Health, 34:3-26. |
| [52] | Ross, DA et al. (2005), Community randomised trial of an innovative adolescent sexual health intervention programme in rural Tanzania: the MEMA kwa Vijana trial. |
| [53] | Rusakaniko, S et al., (1997), Trends in reproductive health knowledge following a health education intervention among adolescents in Zimbabwe. Central African Journal of Medicine, 43:1-6. |
| [54] | Samkaranarayan, S et al. (1996), Impact of school-based HIV and AIDS education for adolescents in Bombay, India. AIDS Education in India, 27:692-695. |
| [55] | Schapink, D, Hema J, Mujaya B. (1997), Youth and HIV/AIDS programmes. In: Ng’weshemi J et al, eds. HIV prevention and AIDS care in Africa: a district level approach. Amsterdam, Royal Tropical Institute, KIT Press, 163-184. |
| [56] | Seidman, M et al. (1995), Fertility awareness education in the schools: a pilot program in Santiago, Chile. San Diego, CA, American Public Health Association. |
| [57] | Secretary-General's Report (2012), Adolescents and Youth. February 2012. Accessed 20.05.13. |
| [58] | Shuey, DA et al. (1999), Increased sexual abstinence among in-school adolescents as a result of school health education in Soroti district, Uganda. Health Education Research, 14: 411-419. |
| [59] | Singh, S. (2003), Study of the effect of information, motivation and behavioural skills (IMB) intervention in changing AIDS risk behaviour in female university students. AIDS CARE, pp. 15:71-76. |
| [60] | Smith, G et al. (2003), HIV/AIDS school-based education in selected Asia-Pacific countries. Sex Education, pp. 3-21. |
| [61] | Speizer, IS, Magnani RJ, Colvin CE. (2003), The effectiveness of adolescent reproductive health interventions in developing countries: a review of the evidence. Journal of Adolescent Health, 33:324-348. |
| [62] | Stanton, BF et al. (1998), Increased protected sex and abstinence among Namibian youth following a HIV risk-reduction intervention: a randomized, longitudinal study. AIDS, 12:2473-2480. |
| [63] | Steinberg, LD. (2008), Adolescence. 8th ed. Boston: McGraw Hill, 2008. |
| [64] | United Nations, (2003), World Youth Report, The global situation of young people. South African Medical Journal. |
| [65] | UNAIDS, (1999), Peer education and HIV/AIDS: concepts, uses and challenges. Geneva, UNAIDS. |
| [66] | UNAIDS, (2013), Global Report on AIDS epidemic http://www.unaids.org/sites/default/files/en/media/ unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf accessed 17/12/2015. |
| [67] | UNAIDS, (2008), Report on the global AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS). |
| [68] | UNAIDS, (2012), Report on the global AIDS epidemic. brglobal_aids_report_en_pdf_red_en.pdf. Accessed 17.12.2015. |
| [69] | United Nations, (2007), Department of Economic and Social Affairs. World Youth Report 2007: Young people's transition to adulthood: progress and challenges. |
| [70] | United Nations, (2000), The Millennium Development Goals http://www.un.org/millenniumgoals/ Accessed 15.09.13. |
| [71] | United Nations, (2010), United Nations World Youth Report: Youth and climate change. 2010. http://social.un.org/index/WorldYouthReport.aspx Accessed May 2013. |
| [72] | UNICEF / UNAIDS, (2011), Opportunity in Crisis: Preventing HIV from early adolescence to young adulthood. |
| [73] | UNAIDS (2012) UNAIDS Report on the Global AIDS Epidemic. Geneva, Switzerland. |
| [74] | United Nations, (2001), Declaration of commitment on HIV/AIDS. Geneva, United Nations, 2001 (available at |
| [75] | http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html. Accessed March 2013. |
| [76] | UNGASS, (2001), http://www.un.org/ga/aids/pdf/aids.pdf Accessed 14.09.15. |
| [77] | UNGASS, (2006), Political Declaration on HIV/AIDS. http://www.unaids.org/en/aboutunaids/unitednationsdeclarationsandgoals/ 2006politicaldeclarationonhivaids Accessed 18/12/2015. |
| [78] | Visser, MJ., Schoeman, JB., Perold, JJ,. (2004), Evaluation of HIV/AIDS prevention in South African schools. Journal of Health Psychology, 9:263-280. |
| [79] | Visser, M. (1996), Evaluation of the First AIDS Kit: the AIDS lifestyle education programme for teenagers. South African Journal of Psychology, 26:103-113. |
| [80] | Wikipedia Encyclopaedia (2013), http://en.wikipedia.org/wiki/Curriculum Accessed 22.09.15. |
| [81] | World Health Organisation (2004), Sexually Transmitted Infections; Issues in Adolescent Health and Development. |
| [82] | World Health Organisation (2006), Department of Reproductive Health and Research. Global strategy for the prevention and control of sexually transmitted infections: 2006–2015. |
| [83] | World Bank (2009), Country Classification. Available at: http://go.worldbank.org/K2CKM78CC0 Accessed 16 12 2015. |
| [84] | WHO (2009), Women’s Health http://www.who.int/mediacentre/factsheets/fs334/en/ accessed 25.05.2013. |
| [85] | WHO, (2001), Balancing protection and risk for adolescents. |
| [86] | http://www.who.int/child_adolescent_health/documents/fch_cah_01_20/en/index.html assessed 15.12.2015 |
| [87] | WHO (2004), Key issues in the implementation of adolescent sexual and reproductive health programmes. Geneva, Department of Child and Adolescent Health and Development, WHO. |
| [88] | WHO (2010), PMTCT strategic vision 2010-2015. Preventing mother-to-child transmission of HIV to reach the UNGASS and Millennium Development Goals. |