-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(6): 198-205
doi:10.5923/j.phr.20150506.05

Tobacco Use in Rural Bangladesh: Socio-Demographic Characteristics, Self Rated Health and Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSamia Aziz, Tarzia Choudhury, Nafisa Huq
School of Public Health, Independent University, Bangladesh, Dhaka, Bangladesh
Correspondence to: Samia Aziz, School of Public Health, Independent University, Bangladesh, Dhaka, Bangladesh.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Tobacco smoking, a leading risk factor for non-communicable diseases (NCDs), has been recognized as the 2nd leading cause of death globally. Bangladesh has been ranked among the top tobacco consuming countries in the world where 68 percent of the total mortality reported in 2006 was due to non-communicable diseases NCDs. This paper explores the association of tobacco consumption with socio-demographic factors, self-rated health and non-communicable chronic diseases among the rural population in Bangladesh. Methods: A cross sectional data from “IUB Health and Socio Economic Survey” 2013 was used for this study. A sample of 1512 male and 1569 female aged 18 and above were randomly selected from four districts of Bangladesh. Binary logistic regression was used to explore the association of tobacco consumption with socio-demographic characteristics; self reported chronic diseases and general health. Results: The prevalence of current tobacco use in any form (smoking or chewing tobacco) among adults in rural Bangladesh was 47.4%. Poor self reported general health was found to be a significant predictor of tobacco consumption. Males were 2.13 times more likely to use tobacco than their female counterparts. Tobacco use was significantly associated with older age (OR=3.18, CI= 2.507-4.035), higher education (OR=0.426, CI=0.289-0.628) and Sylhet region (OR=3.707, CI=2.911-4.720). Conclusions: Strategies to reduce tobacco consumption can focus more on older adults as they are at higher risk of developing chronic morbidity, which may be exacerbated by tobacco use. Regional variation and the role of higher education need to be explored further using in-depth qualitative research. The impact of self-rated health on tobacco consumption should be studied as poor self-rated health is in itself an important predictor of mortality.
Keywords: Tobacco Use, Self Rated Health, Chronic Morbidity
Cite this paper: Samia Aziz, Tarzia Choudhury, Nafisa Huq, Tobacco Use in Rural Bangladesh: Socio-Demographic Characteristics, Self Rated Health and Diseases, Public Health Research, Vol. 5 No. 6, 2015, pp. 198-205. doi: 10.5923/j.phr.20150506.05.
Article Outline
1. Introduction
- Bangladesh, like many transitional nations in the world is straddling through the demographic and epidemiological transitions [1] [2]. The country is observing large decline in mortality due to acute, infectious, and parasitic diseases and increases in chronic diseases such as heart disease and diabetes (collectively known as non-communicable diseases or NCDs) over the last 20 years. Consistent with this shifting epidemiological profile, recent data suggests that tobacco consumption is one of the most important modifiable risk factors contribute to these emerging chronic diseases [3] and has also been identified as a major risk factor for mortality [4].Bangladesh is ranked among the top tobacco consuming countries in the world. [2] [5] Overall, the percentage of Bangladeshi people who use smoked tobacco, smokeless tobacco or both, increased from 36.8% in 2004-05 to 43.2% in 2009 [6]. This alarming rise poses severe impact on the country’s overall disease burden. A WHO study estimated that in 2004, 57 000 people lost their life prematurely as a result of tobacco use and 382,000 people became disabled in Bangladesh [7]. It is also evident from studies conducted in Bangladesh that lung cancer, cancers of the mouth and larynx, stroke and ischemic heart diseases (IHD), and chronic obstructive pulmonary disease (COPD) and obstetric problems such as stillbirth can be attributed to tobacco usage. [8] [9] studies have also found high levels of depressive symptoms increases smoking predispositions level. [10] Considering the fact of such detrimental association of tobacco, patterns and predictors of tobacco consumption has brought under the limelight in different researches. Several studies have found that tobacco consumption is inversely related with individuals’ socio-economic status [11], [12] and has addressed further. But the high uprising trend in Bangladesh needs further exploration. As a result this study focused on Self rated health that has been found to be a good predictor of morbidity and mortality [13], [14]. Individuals’ own assessment regarding their health may decide their health behavior, practices and lifestyle. Study conducted in African population found that satisfaction with life and daily living was much lower for those who use tobacco [15]. Smoking was associated with poor SRH among Chinese adolescents, especially girls [16]. In a study conducted on older Bangladeshis has concluded that older individuals are more likely to report poor SRH than their younger counterparts, and women report significantly worse SRH than their male peers at each age group [17]. From these studies it is evident that self rated health is an important predictor for livelihood, health and diseases. However, there has been no published analysis to explore the association of self reported general health on tobacco consumption in any form in Bangladesh. This study explores the relationship between tobacco consumption and self reported general health and morbidity among the rural Bangladeshi adults. This paper also examines socio-economic, regional and demographic factors that are associated with tobacco consumption.
2. Research Hypothesis
- The study explores the association between self-rated health and tobacco consumption. We hypothesize that people who report bad health are more likely to consume tobacco than those who report good or moderate health, controlling socio-demographic background and self reported chronic morbidity.
3. Methods
- This study uses cross-sectional data from “IUB Health and Socio Economic Survey”, a large-scale epidemiologic study which collected data on households in rural communities across four districts in Bangladesh (Manikganj, Sylhet, Bogra and Natore). The four districts were purposively selected because of the availability of non-governmental organizations that provided logistical support for data collection. In each district, the study randomly selected three villages. In each village, the study randomly selected around 325 households. Interviewers conducted face to face interviews with participants and collected data using a pre-tested online questionnaire set up on mobile phones. Data collection using mobile interface eliminates errors in manual data entry. Coordinated by Independent University, Bangladesh (IUB), the survey was conducted from 5-12 January, 2013 by 120 pairs of interviewers. Each pair of interviewer collected data on approximately 11 households during the survey period. In this way, the survey covered 1310 households which consisted of 3081 adults (aged 18 years and above).
3.1. Measures
- Tobacco Use: Current tobacco users were assessed with the question “are you currently using any tobacco products such as cigarette, bidi, hukka, gul, or betel leaf with tobacco (locally known as ‘paan’ with ‘jorda’)?” Ceased user and never users were also assessed using the question “do you still have the habit of using any tobacco?” and “have you ever used any tobacco?” and was categorized as non-current users of tobacco. Socio-demographic characteristics: The survey collected information on respondents’ age, sex, marital status, level of education and monthly income. Age of the respondents was broadly categorized into 3 categories- young age (18-33), middle age (34-49), and older age (50 and above). Respondents were asked “on average, how much you earn per month” to assess their level of income and then further categorized into four segments considering the rural economical settings of Bangladesh. Chronic Morbidity: The survey obtained information on several chronic and acute diseases which are prevalent among Bangladeshi adults. This study has only incorporated self-reported chronic diseases like heart disease, diabetes, gastric/ulcer, asthma, hypertension, stroke and depression that comprise a large proportion of disease burden caused by Non Communicable Diseases (NCDs) and have evidence of attribute from tobacco consumption. The question “has a health care professional ever diagnosed you with the following diseases?” was used to determine the health status of the respondents. Depressive Symptoms: Participants were asked whether they had experienced the following symptoms for a continuous period of at least two weeks in the last 12 months: tiredness, loss or gain in weight, trouble sleeping, trouble concentrating, thoughts about death, feelings of worthlessness, and loss of enthusiasm for important pastimes. In the absence of a specific validated scale to measure depression in our questionnaire, we operationalized ‘depression’ as having more than 3 depressive symptoms. Self-reported general health (SRH): Self-rated general health was assessed by asking “how is your current health condition?” Three probable options were given to the respondents to know how they define their own health: Good, Moderate and Bad.
3.2. Data Analysis
- In this study, we analyzed data using Stata 12 software. The primary outcome was a dichotomous variable which indicated whether participants currently consumed tobacco. This study examined associations of tobacco consumption and socio-economic factors, self reported morbidity and health variables using chi-square test. A p-value of less than .05 was considered significant. We used binary logistic regression with odds ratio and 95% confidence interval to determine the impact of socio-economic factors, self reported morbidity and health variables on tobacco consumption. Four logistic regression models were used in this study. The first model incorporated tobacco consumption and self rated health. In the second model, all predictive socio-economic variables (age, sex, marital status, education level, income and site) were included. The third model controlled for chronic diseases (such as heart disease, diabetes, gastric / ulcer, asthma, hypertension, stroke and depression) along with all socio-demographic variables. An interaction term between sylhet region and higher education was added in the final model of logistic regression.
4. Results
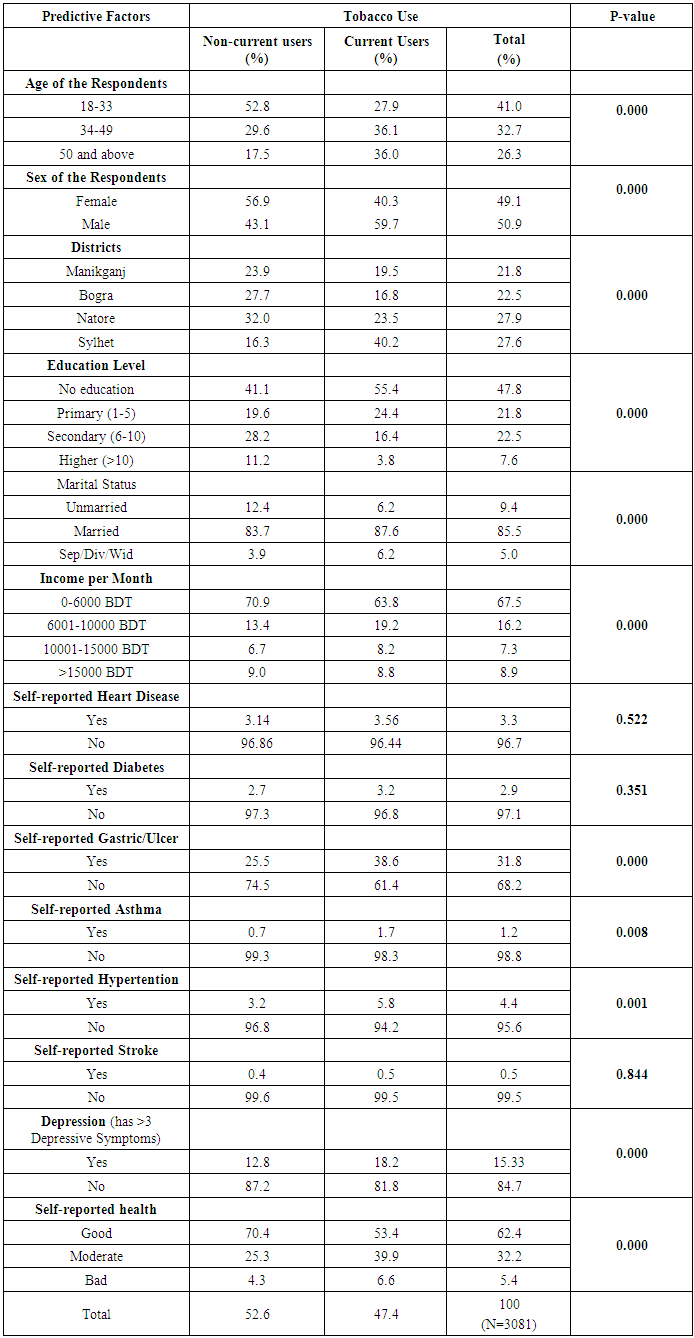
- Of the 3,081 respondents, 41% belonged to the young age group (18-33) whereas 32.7% were in the middle age group (34-49) and 26.3% were aged 50 and above, as shown in Table 1. Our sample consisted of an almost equal proportion of males and females (49.1 and 50.9 respectively). There were slightly more respondents from Natore and Sylhet (around 28 percent), compared to Manikganj and Bogra (around 22 percent). Around half of the respondents (47.8%) had no education. The majority (85.5%) of respondents were married. Most of the respondents (67.5%) earned between 0-6,000 BDT per month.
|
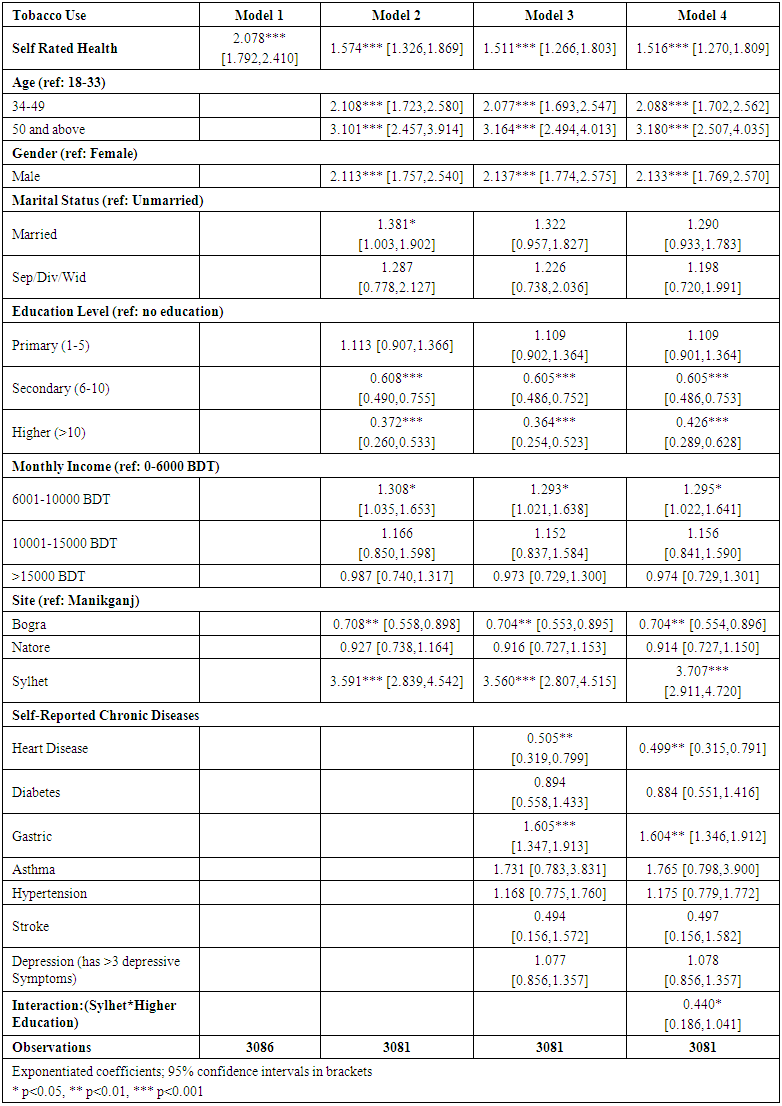 | Table 2. Multiple regression analysis with Tobacco Use as dependent variable and Self-reported Health, Socio-demographic Status and self rated chronic morbidity as independent variables |
5. Discussion
- This paper has explored the association of tobacco consumption with self rated health, chronic morbidity and other socio-demographic characteristics among rural residents of Bangladesh. After controlling for all the predictive variables of tobacco consumption, poor self-rated health (SRH) had a very strong and statistically significant association with tobacco consumption. Studies have found associations of poor SRH with smoking among adolescent population [18, 19]. In this study, we found a similar association for adults and for all forms of tobacco use (smoking or chewing) after controlling for disease and depression. As self-rated health is a strong predictor of mortality, future research should explore the behavioral changes which may result from one’s perception of health. In addition to self-rated health, it is important to explore the complex relationships between temperamental dimensions, depressive and anxiety symptoms with regard to nicotine dependence and cessation success, especially after pharmacological treatment [20]. Our findings on socio-demographic predictors of tobacco consumption are largely consistent with other national and international studies which found significant associations of tobacco use among males, older adults and people with lower education [11, 21, 22]. Several studies have also found that people with lower income or poor social class are more likely to consume tobacco [10, 23]. Similarly, our results indicate that respondents with higher monthly income were less likely to use tobacco. However, this association was not statistically significant. We found that people in the lower middle income group were more likely to consume tobacco compared to respondents in the lowest income group. This may indicate that tobacco consumption is a pastime that is most likely to be taken up by people who have only a small amount of income to spare after spending on basic life needs. It may also be noted that the effect of income may be offset by the low cost and easy accessibility of tobacco products in rural area of Bangladesh. In this paper, respondents with self-reported heart diseases were less likely to consume tobacco. A cross sectional study conducted in Bangladesh found that heavy and long duration use of gul was significantly associated with chronic heart disease [24]. As we account for current consumption of tobacco, our results may be impacted by previous diagnosis of heart disease. In such cases, people with heart disease may make a conscious decision to stop consuming tobacco in order to improve their health. A trend of lesser tobacco consumption has been found among respondents with higher education. Studies have shown that higher education creates more awareness of risk behaviors. Most of the educational campaigns in Bangladesh focus on primary education and not on higher education. A study conducted on 10 high schools in rural Bangladesh depicted a trend of dropout starting at a slower pace of about 9-10% at Class VI, rising slowly to Class IX and ending with a ‘bang’ of around 60-70% at Class X [25]. Factors responsible for this massive drop out should be identified and addressed to raise the number of people with a higher education which may help in reducing tobacco consumption. Regional variation of tobacco consumption in this study is also consistent with other international studies [15]. Respondents in Sylhet were 3.8 times more likely to consume tobacco compared to respondents in Manikganj. This may be due to the fact that Sylhet is considered to have an independent cultural identity resulting from traditional beliefs and practices despite being part of the larger Bengal [26]. However, we also found that respondents with higher education in Sylhet were 59% less likely to consume tobacco, confirming the positive role of education in reducing tobacco consumption.
6. Limitations
- The use of cross-sectional data limits our understanding of the factors which are causally linked with tobacco consumption. Longitudinal data on factors that influence tobacco initiation would be more beneficial in addressing ways to prevent tobacco consumption.Another limitation is the purposive selection of districts in which we conducted our study which may not be representative of Bangladesh. However, random selection of villages and households within these districts minimized possible selection bias. Self-report of diseases may have resulted in a biased representation of people with diagnosed diseases. However, it is important to note that our survey was conceptually designed to measure the prevalence of diseases and risk factors in the rural population. Information on sick participants were often collected or confirmed from family members. The questionnaire also specifies that only diseases which have been diagnosed by a medical professional should be reported.This study is also limited by the range of variables that were available for analysis. Accessibility, local price of tobacco products, information on social and individual networking and support system, and exposure to media may have provided additional insight.
7. Conclusions
- Bangladesh has a long history of tobacco use and a variety of ways in which tobacco is consumed [11]. In spite of the enactment of rigorous tobacco control law in Bangladesh in 2005, 43% adults in Bangladesh still consume tobacco [27]. Research conducted on tobacco consumption so far in Bangladesh has emphasized on socio-demographic characteristics only. This study found that poor self rated health is highly associated with tobacco consumption. As self-rated health is an important predictor of mortality, the causal relationships between tobacco use and self-rated health should be further explored.This study found that higher education has a strong positive association with tobacco consumption. As Bangladesh is already focusing on primary education, there should be more emphasis on secondary and higher education with an aim to reduce high school drop outs. Regional differences also account for variation in tobacco consumption. Further research is needed to explore the effect of location in mediating tobacco use. These results may enable policy planning and implementing further strategy to combat tobacco consumption in rural Bangladesh.
ACKNOWLEDGEMENTS
- We are grateful to Independent University Bangladesh, IUB for the permission of accessing “IUB Health and Socio Economic Survey-2013” data. We would like to thank all students and faculty members of Independent University, Bangladesh IUB who contributed for data collection.
Abbreviations
- SRH: Self Rated Health, NCDs: Non Communicable Diseases, IUB: Independent University, Bangladesh.