-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(5): 159-165
doi:10.5923/j.phr.20150505.06
Knowledge and Practice of Hand Washing among Caregivers of Under-Five Children in a Rural Nigerian Community
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAigbiremolen A. O.1, Abejegah C.1, Ike C. G.1, Momoh J. A.1, Lawal-Luka R. K.1, Abah S. O.2
1Department of Community Medicine, Irrua Specialist Teaching Hospital, Irrua, Nigeria
2Department of Community Health, Ambrose Alli University, Ekpoma, Nigeria
Correspondence to: Aigbiremolen A. O., Department of Community Medicine, Irrua Specialist Teaching Hospital, Irrua, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Hand washing is a very important public health tool in disease control. The control of some of the leading causes of under-five morbidity and mortality is greatly enhanced when mothers and other care-givers adopt appropriate hand washing practices. The study was done to assess the knowledge and practice of hand washing by mothers and caregivers of children less than five years with a view to recommending ways of enhancing the practice in rural communities. This was a cross-sectional survey using a cluster sampling technique. A sample of 513 mothers and care givers was drawn from selected quarters in Usugbenu-Irrua and studied with interviewer-administered questionnaires. A scoring system designed by the research team was used to assess the knowledge of respondents. The mean age of mothers interviewed was 31.6 (±9.2) years. Over two-third (70.6%) of them had good knowledge of hand washing. Fifty-six percent reported regular washing of hands at critical moments; hand washing was highest after defecation (79.6%). There was no statistically significant relationship between the knowledge and practice of hand washing (df=1, X2 = 2.796, p = 0.094). The commonest reasons given for not washing hands regularly were: being too busy (19%) and non-availability of soaps (17.7%) and water (13.5%).The findings showed that though there is a gap between knowledge and practice of hand washing, it is not statistically significant. The study indicates that other factors beyond knowledge may be responsible for poor hand washing behaviour.
Keywords: Knowledge, Practice, Hand washing, Infection control, Mothers
Cite this paper: Aigbiremolen A. O., Abejegah C., Ike C. G., Momoh J. A., Lawal-Luka R. K., Abah S. O., Knowledge and Practice of Hand Washing among Caregivers of Under-Five Children in a Rural Nigerian Community, Public Health Research, Vol. 5 No. 5, 2015, pp. 159-165. doi: 10.5923/j.phr.20150505.06.
Article Outline
1. Introduction
- Hand washing with soap and water is one of the most effective measures against infectious disease [1, 2]. The practice is safe, cheap and not time consuming. Hand washing could be effectively adopted by any socio economic class and by any community. The practice of hand washing is also culture-sensitive and is generally acceptable across many population groups. A consistent practice of proper hand washing with soap and water has the great potential of keeping a family, especially, mothers and children, away from germs and hence ill health. The hands are about the most important human anatomical structures that man uses to interact with his environment. This interaction transcends virtually all aspects of the environment: hands are used to lift objects; they are used to touch pet animals and plants in the biological environments; and also used for social actions like shaking of hands, petting and hugging. Mothers and other care givers are engaged in these interactions and more particularly with respect to catering for their under-five children. Inadvertently, their hands pick up micro-organisms and other materials that may be harmful to children. In general, ‘critical moments’ for hand washing include after using the toilet, cleaning a child up following defeacation, before preparing food and before eating [3]. Other times when hand washing is important are after changing diapers, attending to a sick person, handling raw meat, fish or poultry, after handling garbage, treating a wound or cut, contact with domestic animals, before preparation and eating of food.In caring for children, especially those less than 5 years old, there are some peculiar aspects such as handling diapers, disposing of faeces and urine, and extracting catarrh that introduce harmful organisms into mothers’ hands. A 2006 study in Idumebo, a rural community sharing similar socio-cultural characteristics and in geographical contiguity with the present study location found that up to 30% of mothers administer complimentary feeds to their infants using bare hands [5]. Thus, there is a high possibility of infecting the child and transmitting infections to other members of the household when hand hygiene is not maintained. In rural communities, there are other factors that determine the extent to which the practice of hand washing is promoted and adhered to. Such factors range from the availability of water to cultural perceptions of when and how often hands should be washed [6].In many places where the practice of hand washing is largely accepted as a cost-effective measure important in the control of communicable diseases, there are differences in the patterns of practice. These patterns have to do with knowledge, frequency and use of hand washing materials. Effective hand washing involves the vigorous, brief rubbing together of all surfaces of lathered hands, followed by rinsing under a stream of water. This action suspends microorganisms and mechanically removes them by rinsing with water thereby reducing the number of microbes on the hands in most situations [4]. This simple process is valuable in preventing the spread of infection from one person to the other. As several studies have shown, hand washing and basic hygiene behavior could minimize the spread of germs and as such prevent diarrhea, acute respiratory infections such as influenza and skin infections [7-9]. This simple act is thought to be capable of preventing about 47% of child diarrhoea [10] and 23% of respiratory infections [11].In Nigeria, the commonest causes of morbidity among children under five years of age are malaria, measles, malnutrition, acute respiratory infections (ARIs) and diarrhoeal disease. Diarrhoeal disease and ARIs are strongly linked with poor hand washing practices among other factors [10]. Furthermore, the National Demographic and Health Survey 2013 reveal that childhood morbidity and mortality are higher in rural than urban areas [12]. Diseases such as acute respiratory infections and helminthic infections have also been closely associated with unwashed hands. Globally, it is estimated that over 4-6 million deaths of children under-five are due to diarrhea and acute respiratory tract infections with diarrhea alone accounting for 47% of these deaths [13]. Diarrheal diseases and respiratory infections are amongst the leading contributors to the global burden of disease and poor water supply, sanitation and hygiene represent 7% of the risk factors [14]. Thus, there is an important link between poor hand washing practices of mothers and the morbidity of children less than 5 years of age especially those living in rural communities. The aim of this study is to create a better understanding of the level of knowledge and practice of hand washing among mothers of under-five children in the rural community of Usugbenu-Irrua in Esan Central LGA, Edo State of Nigeria.
2. Methodology
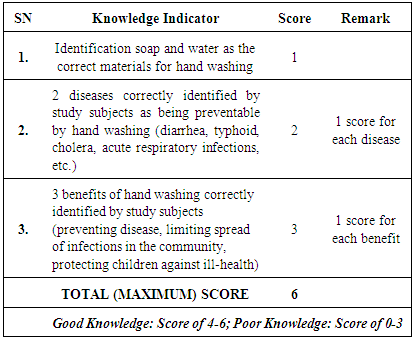
- This was a cross-sectional study done using the cluster sampling technique in which 4 of 8 quarters in the community were randomly selected for the study. The quarters in the village constituted the clusters. All consenting mothers and other caregivers (other family members and foster parents) who had children less than five years old directly under their care were interviewed in each cluster. Interviewer-administered semi-structured questions were administered to 513 mothers. The pre-tested questionnaires were administered by trained undergraduate medical students. The minimum sample size of 262 subjects was calculated using the Cochran formula [15, 16]: n = Z2pq/E2 where n = sample size; Z = standard normal deviate (1.96); p = a hand washing practice prevalence of 21.7% from a previous study [17]; q = 1-p = 0.783; E = tolerable error of margin (0.05).Knowledge of hand washing was assessed with a scoring system designed by the authors (Box 1) following the pretesting of questionnaires used for the study. Correct hand washing was defined as washing hands with soap and water. After data cleaning, 496 of the questionnaires were available for analysis using the SPSS software. Secondary data analysis was done with WINPEPI [18]. Chi-square test was used to test for significance at p< 0.05. The results are presented in tables.
|
3. Results
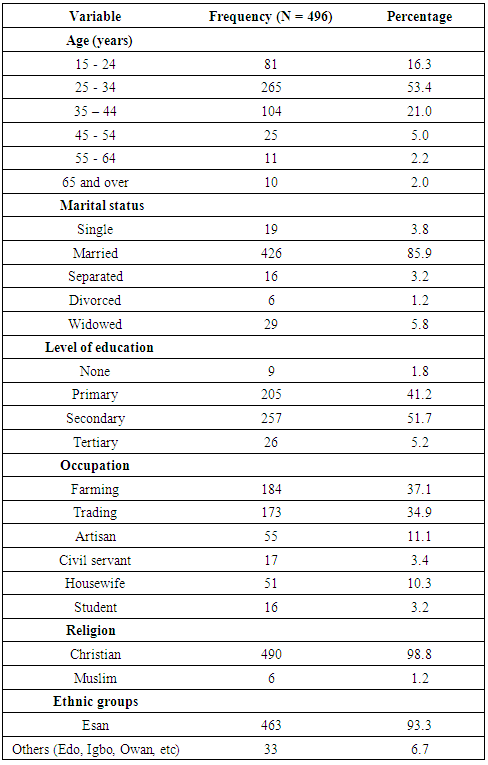
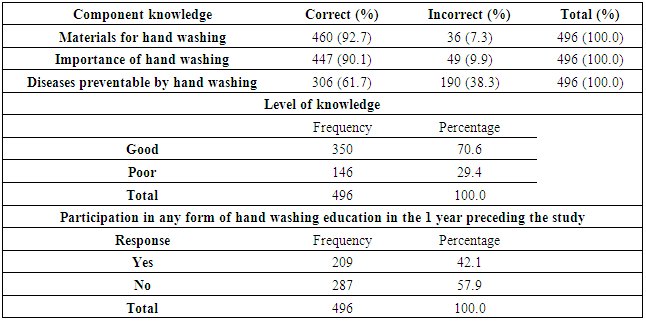
- The mean age of caregivers interviewed was 31.6 (±9.2) years and majority of them were married (85.9%). Most of the mothers/caregivers were either farmers (37.1%) or traders (34.9%) (Table 1). Over two-third (70.6%) of respondents had good knowledge of hand washing. Only 42.1% of the respondents had participated in any form of hand washing education program in the one year preceding this study (Table 2). Fifty-six percent reported regular washing of handsat critical moments (at least once immediately after critical activities); hand washing was highest (79.6%) after defecation (Figure 1).
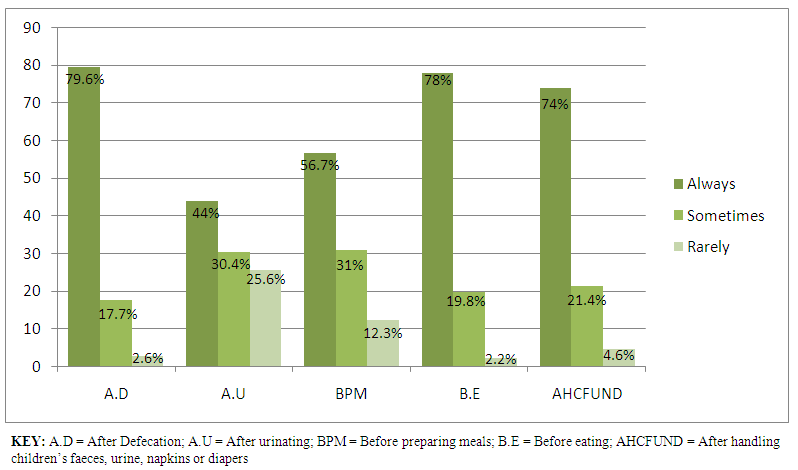 | Figure 1. Practice and pattern of hand washing among mothers/caregivers of under-five children in Usugbenu |
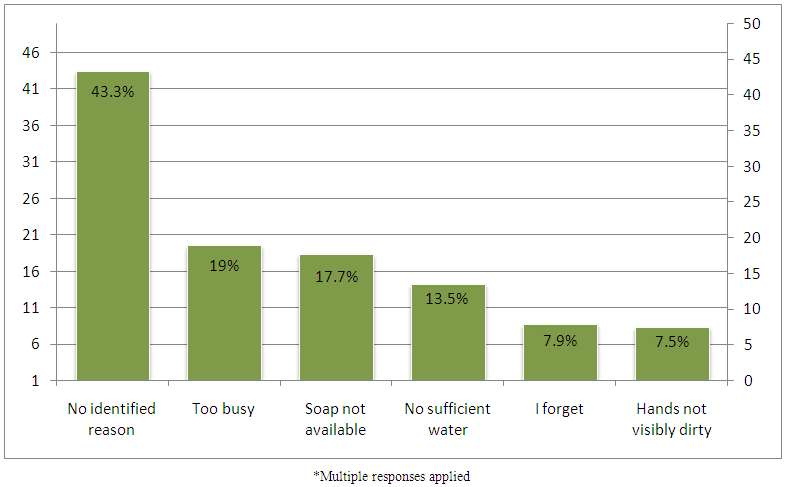 | Figure 2. Reasons for not washing hands regularly |
|
|
|
|
4. Discussion
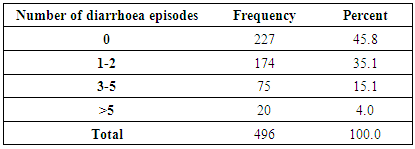
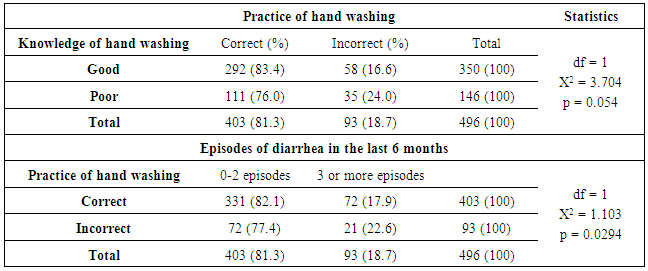
- Over half of the respondents in this study had at least a primary level of education which is not surprising given that a previous study in the area found a literacy rate of about 48% among the respondents [19]. This finding is also comparable to the finding in another study done in 50 rural communities in Bangladesh, with 48% of the mothers having more than a primary education [20]. Over two-third (70.6%) of respondents had good knowledge of hand washing (Table 2). Closely linked with this was the very high knowledge of materials used for hand washing, and importance of hand washing. These findings are similar to those found in Osogbo study where good knowledge of hand washing was 93% and knowledge of the importance was 99% [17]. Similarly, in an Indian study, majority of the respondent mothers had knowledge that washing hands was important in the prevention of communicable diseases but there were lower figures for knowledge of the specific disease condition: only 38.88% and 24.92% believed that this practice could prevent diarrhea and ARI, respectively, among children [21]. In contrast, the findings from a study done in two resource-poor settings in Kenya showed that new mothers in urban slums and rural areas have insufficient knowledge or do not practice correct hand washing habits that would reduce the burden of neonatal infections [22].Participation in a hand washing health education activity was low (Table 2). Health promotion activities on personal and environmental hygiene, including hand washing improve knowledge and ultimately the practice of hand washing [23]. Role plays, demonstrations and health talks are relevant in this respect as has been applied in the community previously [24]. Hand washing was highest after defecation, followed by before eating and after cleaning the child. This pattern is similar to the findings in a previous study on Environmental risk factors for diarrhea among breast feeding mothers carried out at Idumebo, a peri urban community in geographical contiguity with the present study location which found that 81% of respondents washed their hands after using the toilet and before preparing feeds [19]. Similarly, it closely replicates what was recorded in a study done in rural India where the figures were 73.18% washed hands after defaecation, 63.91% after cleaning the child who had defaecated and 29.98% before feeding the child respectively [21]. The observed pattern may be explained on the basis of the fact that faeces is commonly viewed as a highly detestable kind of waste capable of inducing resentment of the person who might be associated with its odour, whilehand washing before eating is more of a cultural practice than for hygiene purposes among many folks [6, 25].The non-significant relationship between knowledge and practice of hand washing among the study group suggests that other factors aside knowledge are more important in determining adherence to the practice of hand washing. Important among these factors as found in this study are being too busy, soaps and or water not being available at the time hand washing would have been done. Women in a Kenyan survey reported factors such as poor availability of water, not having been shown how to wash hands, and their busy schedules in that order [22]. The importance of regular and correct washing of the hands is depicted in the fact that hand washing with soap removes transient potentially pathogenic organisms from hands and it is not sufficient to wash hands with only water after critical events like defecation [21].Being too busy may be reflective of the individual’s attitude. When people appreciate the possible consequences of non-adherence to hand washing, they are more likely to create time for adherence. Non-availability of hand washing facilities and being busy with patients were reported as important factors for poor adherence to handwashing in another study in Karachi [26], which tends to support the view that hand washing is related to the value system of the individual. The statistically significant association between hand washing practice and diarrhea episodes in this study supports he importance of hand washing by others [19, 10].
5. Conclusions
- The findings showed that there is a gap between knowledge and practice of hand washing. The study suggests that other factors beyond knowledge may be responsible for poor hand washing behavior. These factors include non-availability of water and other hand washing materials in sufficient quantities. Therefore, efforts must be made to make water and other hand washing facilities readily available in rural communities in addition to enhancing health promotion for hand washing.
ACKNOWLEDGEMENTS
- We acknowledge the support given by other members of staff in the Department of Community Medicine, ISTH, Irrua during community mobilization activities for this work.
Annex: Questionnaire
- Knowledge, Practice and Pattern of Handwashing among Caregivers of Under-Five Children in a Rural Nigerian CommunityWe invite you to participate in this survey on the above subject. Answers provided to the questions will be treated in confidence and used only for the purpose of this research. Thank you.NB: Multiple responses are applicable to questions with asterisks (*).A. BIODATA1. Mother or caregiver’s age (in years) as at last birthday: ……………………………..2. Marital status: Single ( ) Married ( ) Divorced ( ) Separated ( ) Widow ( )3. Mother’s Level of education: Primary ( ) Secondary ( ) Tertiary ( ) none ( )4. Mother’s occupation: Subsistent farmer ( ) Commercial farmer ( ) Petty trader ( ) Trader/Business woman ( ) Civil servant ( ) Housewife ( ) Others…………………………..5. Husband’s Level of education: Primary ( ) Secondary ( ) Tertiary ( ) none ( )6. Husband’s occupation: Subsistent farmer ( ) Commercial farmer ( ) Petty trader ( ) Trader/Business man ( ) Civil servant ( ) Housewife ( ) Others…………………………..7. Religion: Christian ( ) Muslim ( ) Others (specify) …………………… 8. Ethnic group:…………………………………B. KNOWLEDGE1. Have you ever heard about hand washing? Yes ( ) No ( )2. *Where did you hear about it? School ( ) Church ( ) Television ( ) Radio ( ) Print Media ( ) Friend/Neighbour ( ) Others:……………………..3. *What is the importance of hand washing? Helps prevent diseases ( ) Helps protect your children from infections ( ) Helps limits spread of infections in the community ( ) Do not know ( ) Others:………4. *What diseases can be contracted by not washing hands? Malaria ( ) Typhoid ( ) Diarrhoea disease ( ) Airway infections ( ) Others …………5. What materials are needed for effective hand washing? Water only ( ) Water and soap ( ) Ash and water ( ) hand towel/Clean Piece of cloth ( ) Others:………………………………………….6. Have you had any health education on hand washing in the last one year? Yes ( ) No ( )C. PRACTICE1. How often do you wash your hands? Always ( ) Sometimes ( ) Rarely ( ) Never ( )2. How do you wash your hands? a. Soap and water: Always ( ) Most times ( ) Rarely ( )b. Water only: Always ( ) Most times ( ) Rarely ( )3. Do you wash your hands after the activities below?a. After defeacating? Always ( ) Most times ( ) Rarely ( ) Never ( )b. After urinating? Always ( ) Most times ( ) Rarely ( ) Never ( )c. Before preparing food or drink? Always ( ) Most times ( ) Rarely ( ) Never ( )d. When you return from the farm or market? Always ( ) Most times ( ) Rarely ( ) Never ( )e. Before eating? Always ( ) Most times ( ) Rarely ( ) Never ( )f. After handling your child’s faeces, urine, diapers or napkins? Always ( ) Most times ( ) Rarely ( ) Never ( )4. *What are the major sources of water in your household? Rain water ( ) Borehole ( ) Rivers/Stream ( ) Pipe-borne water ( ) Well ( ) Others:…………..D. OUTCOME1. Has any child been sick or admitted in the past 6 months? Yes ( ) No ( )2. *If yes, what were the symptoms? Fever ( ) Watery stool with mucus ( ) Watery stool with blood ( ) Cough ( ) Vomiting ( ) Others :……………………………………………..3. If your child has had watery stool, how many episodes? 0-2 ( ) 3-5 ( ) >5 ( )4. *What challenges do you sometime experience in regards to hand washing? a. Inadequate water supply ( )b. Soaps not available ( )c. No time (I am too busy) ( )d. No hand towel/clean cloth available ( )e. Others: …………………………………………..5. How do you think the problems mentioned above (7) can be helped:………………………………………