-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(5): 129-134
doi:10.5923/j.phr.20150505.01
Effect of Exposure to Cement Dust on Pulmonary Function among Cement Plants Workers in the Middle Governorate, Gaza, Palestine
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYousef Aljeesh1, Wesam Al Madhoun2, 3, Suliman El Jabaly4
1Associate Professor in Public Health, Islamic University, Gaza Strip, Palestine
2Assistant Professor of Environmental Engineering, Islamic University, Gaza Strip, Palestine
3MIT-UTM program on Sustainable cities, Universiti Teknologi Malaysia, Johor Bharu, Malaysia
4Clinical Instructor in Nursing, Al Quds Hospital, Gaza strip, Palestine
Correspondence to: Suliman El Jabaly, Clinical Instructor in Nursing, Al Quds Hospital, Gaza strip, Palestine.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This study was conducted to investigate the level of PM air pollution in cement plants, and their impacts on respiratory system health and pulmonary function for cement plants workers. Case-control study was conducted on all cement plants at Middle Gaza Governorates. 100 individuals participated, case (exposed) and control (non exposed) groups contain 50, 50 respectively. All participants were subjected to questionnaire, lung function measuring by electronic spirometery. The findings of this study showed that an average particulate matter from 106.3 to 143.3, which is about more than 4 times higher than the particulate matter (PM2.5) existing standard of 35 μg/m3 also an average particulate matter from 615 to 656, which is about more than 4 times higher than the particulate matter (PM10) existing standard of 150 μg/m3. As well as, it showed clear links between PM exposure and respiratory health and pulmonary function. Cough, dyspnea and sputum buildup were more common among the exposed group, Furthermore, the mean of FEV1/ FVC (%) for control group is significantly greater than that for FEV1/ FVC (%) for case group. Among other recommendations, this paper infers that Environmental and engineering control of cement dust emissions, protective techniques, procedures, measures and equipment and periodic medical examinations.
Keywords: PM2.5, Respiratory symptoms, Pulmonary function, Cement plants
Cite this paper: Yousef Aljeesh, Wesam Al Madhoun, Suliman El Jabaly, Effect of Exposure to Cement Dust on Pulmonary Function among Cement Plants Workers in the Middle Governorate, Gaza, Palestine, Public Health Research, Vol. 5 No. 5, 2015, pp. 129-134. doi: 10.5923/j.phr.20150505.01.
Article Outline
1. Introduction
- The worldwide community, especially the people in developing countries, are facing increasing risks of respiratory diseases due to production of smoke and dust in different occupational and industrial sectors [1].It is impossible to envisage a modern life without cement. Cement is an extremely important construction material used for housing and infrastructure development and a key to economic growth. Cement demand is directly associated to economic growth and many growing economies are striving for rapid infrastructure development which underlines the tremendous growth in cement production [2].The cement industry plays a major role in improving living standard all over the world by creating direct employment and providing multiple cascading economic benefits to associated industries. Despite its popularity and profitability, the cement industry faces many challenges due to environmental concerns and sustainability issues [3].Cement is one of the most important building materials in the world. A cement plant can be a significant source of air pollutants, and cement dust can affect respiratory symptoms and lung function. Previous studies indicate reduced lung function [4].Particulate matter (PM) has been found to be a major threat to human health. Health impact is caused by concentrations of PM in ambient air to PM standards, the size of the particles and spatial planning [5].The number of plants concrete operating in the Gaza Strip, 32 plants, according to the Ministry of National Economy, while the number of plants granted certification by the Ministry of Public Works and Housing 11 plants only after compliance with regulations quality control approved by the ministry, This means that there are a large number of plants pose a danger to the environment and the health of their workers.Cement industry in Palestine has a specific importance in this time in particular where the Palestinian society passes in construction stage and a populating of what increases the demand size on the cement, and this is what gives an extreme importance to establish local factory on the market compliance from the cement material by the specifications the competition price and to putting limit in front of the subjection of the Palestinian market to the Israeli economy in this side.In a previous study, occupational exposure to cement dust is known to be an important factor in the causation of the chronic respiratory health effects [6].In recent times. There were many problems affecting the respiratory system in the human body and there are many factors that cause various diseases and serious respiratory infections such as: crisis, lung fibrosis, acute and chronic infections, asthma ... Etc. May be a cement dust affecting on the pulmonary function by causing some of these disease [7].Therefore, there are many problems and lack of awareness as a result of wrongful conduct to work in the plants of concrete, where the impact of the non-use of protective supplies negatively on the respiratory health of workers in the plants and on the quality of the air in the around area [8].Pulmonary functional measurements reveal significantly increased lung resistance, transpulmonary pressures, and functional residual capacity with decreased dynamic lung compliance and arterial oxygen tension and accompanying chronic respiratory acidosis [9].These emissions are not only deteriorating air quality but also degrading human health. Emissions have local and global environment impact resulting in global warming, ozone depletion, acid rain, biodiversity loss, reduced crop productivity etc [10].Results of several studies showed that these emissions are adversely affecting human health in a variety of ways, like itchy eyes, respiratory diseases like tuberculosis, chest discomfort, chronic bronchitis, asthma attacks, cardio-vascular diseases and even premature death [11].Summary of Literature ReviewAir pollution has many negative effects on human health and it is recognized as a serious health hazard. There seems to be an association of air pollution with an increased risk of decrease pulmonary function and acute respiratory infections.Following this, cement dust air pollution and its specific clinical effects on the human body were examined and discussed. Health endpoints associated with both short and long term exposure to cement dust were analyzed thoroughly with findings from numerous studies presented. Further, the health impacts of cement dust in Palestine and history of particulate air pollution regulations were discussed. Finally, more than fifteen similar previous studies of short and long term exposure to cement dust and its findings was mentioned, its findings are with line and consistent with our results and findings. From the above comprehensive literature review, it can be concluded that there is a correlation between particulate matters and alterations in pulmonary function and Exacerbation of respiratory symptoms.
2. Materials and Methods
- Case-control study was conducted on all cement plants at Middle Gaza Governorates. 100 individuals participated, case (exposed) and control (non exposed) groups contain 50, 50 respectively.All cement plant workers in the Middle governorate included in the current study. There are (6) cement plants and the total number of workers in is (80) and excluded (30) people who do not work in the middle governorate, and who are under the age of 18 years or more than 40, and have past history. At the same time, The researcher used control group as a comparison consist of (50) participants, who are not working in cement plants, and the case to control group selected 1:1 described simply and matching with age, residence, gender and had not any past medical history.Data was collected in August till November 2014 using structured questionnaire in a face-to-face interview and measuring parameter of lung function by electronic spirometer from each individual and measuring PM in each cement plant. Detailed information about the study was given to the individuals, Both verbal and written consent was obtained from each individual included in the study. The reason for selecting the middle governorate is the location of the plants which are in very populated areas.In those with evidence of airway obstruction and an intermediate probability of asthma, arrange reversibility testing and/or a treatment trial for a defined period, NICE guidance suggests that reversibility testing should not be routine if clinical features and spirometry are strongly suggestive of COPD [12].NOTE A spirometer is a device that monitors the flow of air in and out of a person's lungs. The device can be used for diagnosis and monitoring of pulmonary diseases, particularly Asthma and COPD. Spirometers are divided into two classes (manual and electronic) which have different specifications
3. Results
3.1. PM Level in Cement Plants
- PM2.5 and PM10 emission monitoring was carried out in six cement plants.Figure 1 clarified the emission of PM2.5 by the cement plants varies widely from 82 to 196 μg/m3, with an average particulate matter from 106.3 to 143.3, which is about more than 4 times higher than the particulate matter (PM2.5) existing standard of 35 μg/m3.
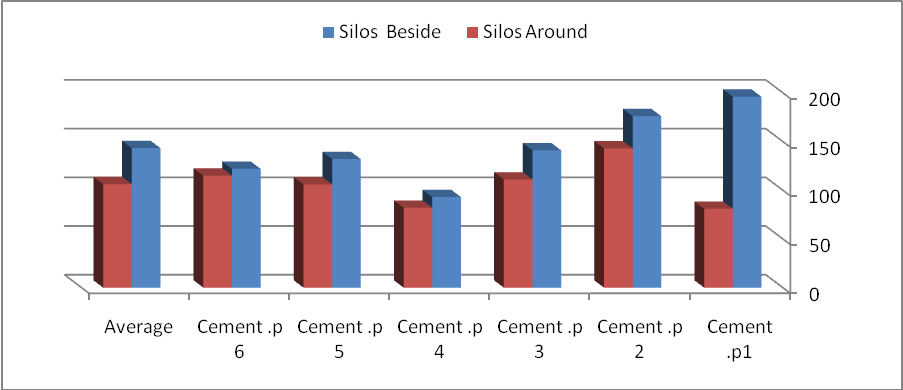 | Figure 1. The average of emission of PM2.5 by the cement plants |
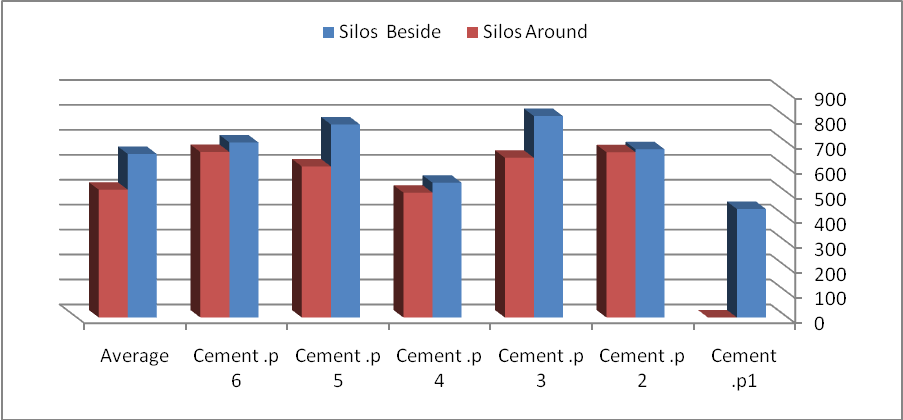 | Figure 2. The average of emission of PM10 by the cement plants |
3.2. Appearance of Respiratory System Symptoms
- Respiratory tract symptoms reported in this study among the exposed workers to PM were cough, sputum build-up and dyspnea. These symptoms were found to be related to exposure of PM.Cough reported significantly among exposed workers to PM and data analysis shows that 88% of the case group suffer from cough, but 94% of the control group do not suffer from cough. Also showed that the presence percentage of exaggerated cough among cases and control. That confirmed 86.4% of case that have cough increased or exaggerated during exposed cement dust. And 79.5% of case that have cough show that they have sputum buildup, but do not buildup in the control group.Also identified the presence percentage of dyspnea that 86% of the case group suffer from dyspnea, but 92% of the control group do not suffer from dyspnea and the rest of the same group (8%) suffer from dyspnea.
3.3. Parameters of Pulmonary Function
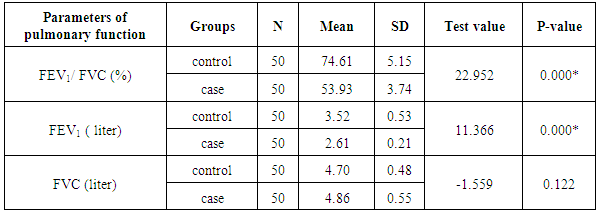
- The result of electronic spirometer for lung function that statistically explained that mean of FEV1 is significantly different between case group and control group which show: The mean of FEV1 for control group is significantly greater than that for FEV1 for case group and there is insufficient evidence to conclude that mean of FVC is insignificantly different between case group and control group. In other words, there is insignificant difference in the mean FVC between case group and control group. In addition to findings confirmed that mean of FEV1/ FVC (%) for control group is significantly greater than that for FEV1/ FVC (%) for case group (Table 1).
|
3.3.1. Forced Expiratory Volume in One Second (FEV1)
- The mean for FEV1 for case group equals 2.61, with SD of 0.21. For control group, the mean for FEV1 equals 3.52, with SD of 0.53. The value of the T-test equals 11.366, with p-value equals 0.000. This implies that there is sufficient evidence to conclude that mean of FEV1 is significantly different between case group and control group. Since the sign of the T-test is positive, then mean of FEV1 for control group is significantly greater than that for FEV1 for case group.
3.3.2. Forced Vital Capacity (FVC)
- The mean for FVC for case group equals 4.86, with SD of 0.55. For control group, the mean for FVC equals 4.70, with SD of 0.48. The value of the T-test equals -1.559, with p-value equals 0.122. This implies that there is insufficient evidence to conclude that mean of FVC is insignificantly different between case group and control group. In other words, there is insignificant difference in the mean FVC between case group and control group.
3.3.3. FEV1/ FVC (ratio)
- The mean for FEV1/ FVC (%) for case group equals 53.93, with SD of 3.74. For control group, the mean for FEV1/ FVC (%) equals 74.61, with SD of 5.15. The value of the T-test equals 22.952, with p-value equals 0.000. This implies that there is sufficient evidence to conclude that mean of FEV1/ FVC (%) is significantly different between case group and control group. Since the sign of the T-test is positive, then mean of FEV1/ FVC (%) for control group is significantly greater than that for FEV1/ FVC (%) for case group.Figure 3 explained 92% of case group have moderate obstruction and the rest of the same group (8%) have mild obstruction. This abnormalities were found to be related to exposure of PM air pollution.
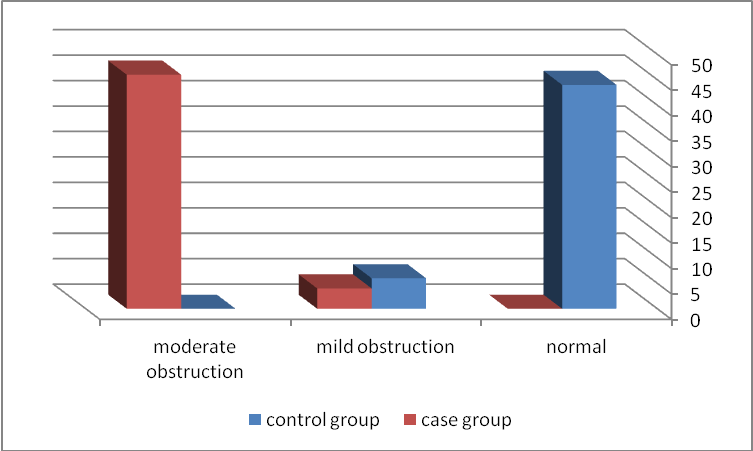 | Figure 3. Shows that the correlation between group and diagnosis |
4. Discussion
- Data in figure (1) reveals that the emission of PM2.5 by the cement plants varies widely from 82 to 196 μg/m3, with an average particulate matter from 106.3 to 143.3, which is about more than 4 times higher than the particulate matter (PM2.5) existing standard of 35 μg/m3 [13].Also, data in figure (1) reveals that the emission of PM10 by the cement plants varies widely from 501 to 808 μg/m3, with an average particulate matter from 615 to 656, which is about more than 4 times higher than the particulate matter (PM10) existing standard of 150 μg/m3 [13].Positive significant relationship is observed between cement dust air pollution exposure and appearance of respiratory system symptom (cough, sputum build-up and dyspnea).The results of the acute respiratory symptom scores are in agreement with data reported by Mwaiselage et al, 2005, Meo et al, 2013, Zeyede, 2010 [14, 15]. Who found a high prevalence of shortness of breath, stuffy nose and sneezing among exposed cement factory workers.In parallel to our findings, Merenu et al, 2007 [6]. investigated the effect of cement dust exposure on cement factory workers with a mean of 10 years exposure to cement dust on lung function. They found that the vital capacity and forced expiratory volume in one second were significantly lower in cement factory workers than in control subjects.The statistical strength of these relationships are in line with review paper carried out by Mariammal T. et al, 2012 [16], where several studies worldwide were reviewed, and observed that occupational respiratory diseases are usually caused by extended exposure to irritating or toxic substances that may cause acute or chronic respiratory ailments. The incidence depends upon the chemical composition of dust, size of the particles, duration of exposure and individual susceptibility. Dust originating from work operation like drilling, blasting and grinding becomes airborne and inhalation of particles may induce accelerated lung function decline.Moreover, results of this study are also in agreement with those in studies conducted in different geographic regions on sample of the general population. Zeleke et al. 2010 [17] found an association between acute respiratory symptoms and acute ventilatory effects and exposure to PM in a combined cross-sectional and cross-shift study in study was conducted in Dire Dawa cement factory in Ethiopia. At the differences, Fell et al, 2003 [18] found that the mean pulmonary function indices were similar for cement plant workers and control group. There was no duration-response-related decrease in lung function indices. However, in the present study we found a decline in lung function parameters with period of exposure to cement dust. The main reason for this difference is the selection protocol of the cement plant workers and the control group. Fell et al, 2003 [18], selected 119 cement plant workers, from them only 19 were non smokers; remaining all were either smokers or ex-smokers.Similarly to our findings, Merenu et al. 2007 [6] investigated the effect of cement dust exposure on 56 cement factory workers with a mean of 10 years exposure to cement dust on lung function. They found that the vital capacity and forced expiratory volume in one second were significantly lower in cement factory workers than in control subjects. Their results suggest that chronic cement dust exposure impairs lung function. Similarly, El Badari and Saeed, 2008 [19] reported a significant reduction in FVC, FEV1 and PEFR in cement dust exposed workers compared to control. The lung function indices were found to be reduced with increasing duration of exposure to cement dust. Our results are in conformity with these results.In parallel to our findings Nordby et al. 2011 [20] reported that Forced Expiratory Volume in the first second (FEV1) reduced with an exposure-response relationship in the highest compared with the lowest exposure level of cement dust. Concurrently, Zelke et al. 2010 [17], found that FVC, FEV1 were significantly reduced among the cement production workers but not among the controls. The reduction in lung function was probably associated with high cement dust exposure.Also, Mwaiselage et al. 2004 [21] investigated ventilatory function in cement factory workers and reported that exposed workers had significantly lower FVC, FEV1, and PEF than controls. Nordby et al. 2011 [20] reported that Forced Expiratory Volume in the first second (FEV1) reduced with an exposure-response relationship in the highest compared with the lowest exposure level of cement dust. Concurrently, Zelke et al. 2010 [17] found that FVC, FEV1 were significantly reduced among the cement production workers but not among the controls. The reduction in lung function was probably associated with high cement dust exposure. Moreover, Sultan A Meo et al, 2002 [22] In cement plant workers, showed a statistically significant reduction was demonstrated in the mean values of FVC, FEV1, PEF, and MVV. The mean value for FEV1/FVC ratio was significantly higher in cement plant workers. Beside that, Al-Neaimi et al. 2001 [23], demonstrated that the ventilatory function (FVC, FEV1, and PEF) were significantly lower in the cement plant workers compared with unexposed subjects.In addition to Sultan A Meo et al, 2013 [14], explained that cement plant workers exposed for more than 10 years showed a significant reduction in FVC, FEV1, MVV, and PEF relative to their matched controls. As well at differences, Fell et al, 2003[18] found that the mean pulmonary function indices were similar for cement plant workers and control group. There was no duration-response-related decrease in lung function indices. However, in the present study we found a decline in lung function parameters with period of exposure to cement dust. The main reason for this difference is the selection protocol of the cement plant workers and the control group. Fell et al. 2003 [18] selected 119 cement plant workers, from them only 19 were non smokers; remaining all were either smokers or ex-smokers. They selected the control group from an ammonia producing industry.In the present study, it observed statistical significant association between particulate matter air pollution exposure and (decrease lung function that measured be spirometer). These results are consistent with the results of related previous studies.
5. Conclusions
- PM10 concentration that emitted from the cement plants varies widely from 521.4 to 656 μg/m3, PM2.5 concentration that emitted from the cement plants varies widely from 106.3 to 143.3 μg/m3.Respiratory tract symptoms reported in this study among the exposed workers to cement dust air pollution were cough, sputum build-up and dyspnea. These symptoms were found to be related to exposure of PM air pollution.Decrease lung function (decreasing FEV1, increasing FVC or normal, decreasing FEV1/FVC) reported in this study among the exposed workers. These disturbances were found to be related to exposure of PM air pollution.The findings of this study can then be given recommendations related to workers and environmental health, among which are:1. Pre-placement medical examination for the exposed workers should include a base line clinical examination of the respiratory and cardiovascular system with pulmonary functions testing and chest X-ray to exclude workers with chest troubles.2. Workers should be informed about the different hazardous effects of particles air pollution on health and enforced them to the proper use of protective clothing and equipment.3. Development of laws to protect the industry and protect them from damage pollutants and the development of recommendations and requirements of engineering and environmental appropriate to each industrial activity.4. Environmental and engineering control of PM emissions in the different cement plants operations of should be applied.