-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(4): 83-89
doi:10.5923/j.phr.20150504.01
Socio-Cultural Determinants of Contraceptives Use Among Adolescents in Northern Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdadow Yidana1, Shamsu-Deen Ziblim1, Thomas Bavo Azongo2, Yakubu Ibn Abass2
1University for Development Studies, School of Medicine, Department of Community Health and Family Medicine, Tamale, Ghana
2University for Development Studies, School of Allied Health Science, Department of Nursing, Tamale, Ghana
Correspondence to: Adadow Yidana, University for Development Studies, School of Medicine, Department of Community Health and Family Medicine, Tamale, Ghana.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Adolescent in both rural and urban areas in developing nations are often underserved by family planning service providers. This limits the knowledge level of young men and women about contraceptive methods. The purpose of this study was to examine what determines contraceptive use among adolescents. Data collection spans January to December 2013 with 400 adolescent men and women of reproductive age as study respondents in the Yendi Municipality of Northern Region of Ghana. The data collection tool was questionnaire and focus group discussion. SPSS version 20 was used in the analysis. It was found that most adolescents would use contraceptives if they did not want to get pregnant or if they want to continue with their education. Overall, the desired family size was lower among all the adolescents. It was observed that once a teenage woman has had a child; contraceptive use prevalence rises to a level comparable to that of women in their twenties. The paper recommends that the family planning officers should give more attention to adolescents. Successful side-effect management and proper education in family planning could increase contraceptive use among adolescents.
Keywords: Adolescent, Contraceptives, Pregnancy, STIs
Cite this paper: Adadow Yidana, Shamsu-Deen Ziblim, Thomas Bavo Azongo, Yakubu Ibn Abass, Socio-Cultural Determinants of Contraceptives Use Among Adolescents in Northern Ghana, Public Health Research, Vol. 5 No. 4, 2015, pp. 83-89. doi: 10.5923/j.phr.20150504.01.
Article Outline
1. Introduction
- Unexpected or unplanned pregnancy poses a major public health challenge in women of reproductive age, especially in developing countries [1]. The rising rate of premarital sexual activity in developing countries has drawn attention of experts regarding adolescent’s decisions about various aspects of reproductive health behaviour [2,3]. In this regard, concerns have been raised about the adverse effects of early childbearing, particularly for unmarried adolescents, and the risks of contracting sexually transmitted diseases. This has given rise to a renewed interest in sexual behaviour of adolescents [4]. Adolescent as used in this study refers to persons aged 14-19 years, though others may peg it at 14-24 years [5]. In parts of developing countries, adolescents are noted to have special sexual and reproductive health needs [6]. As a result many are often exposed to inaccurate or incomplete information [7, 8]. It has been observed that many adolescents in recent times engage in unsafe sex, leading to high rate of unplanned pregnancies [9]. Situations of this nature call for contraceptive use in adolescence to be given special attention [10]. Another important dimension is that adolescents between 14-19 years have been noted to be sexually active yet; they rarely use contraceptives due to negative societal attitudes [11-14]. As a consequence, a number of adolescent girls who get pregnant often drop out from school (if they are in school) and are unlikely. Many of them do not often have the social and economic means to raise their children [15-17]. The Ghana Demographic and Health Survey (GDHS) have indicated that about 13.0% of 14-19 years olds are pregnant or are already mothers. Surprisingly, 69.0% of births to this category are either unwanted or mistimed [18-20]. According to [21], Northern region of Ghana has the highest total fertility rate of 6.8 children per woman, and the contribution of adolescents to these rates cannot be over looked. If young people continue to experiment with sex and yet fail to use contraceptives, the likelihood of many of them becoming pregnant is very high. Such pregnancies may end up with ‘back street abortions’ or teenage childbearing. This paper examines factors associated with the use of contraceptives among adolescent males and females in the Yendi Municipality in the Northern Region of Ghana.
2. Methodology
- A descriptive cross-sectional study was carried out from August 2013 to July 2014 in the Yendi Municipality in the Northern Region of Ghana. The selection of respondents was done at both institutional (schools) and household levels. The total number of adolescents interviewed was 400. The sample size was estimated using Yamane’s Equation: n = N/[1+N(e)^2], where ‘n’ is the sample size, ‘N’ is expected adolescents and ‘e’ is level of precision at 7%, using 95% confidence interval. To minimize bias in the selection, respondents at the institutional level were selected for interview using systematic sampling technique. At the community level, respondents were selected at shops where they do their daily business. Two final year nursing students were recruited and trained to help administer the questionnaire. An informed consent was sought from all participants before the commencement of the interview. Each interview administered questionnaire lasted between 25 to 35 minutes. The language for the research was English language and Dagbani precisely because the indigenous dialect in the area is Dagbani. Permission and approval was sought from the Ghana Education Service and heads of the various schools before the commencement of the research.
3. Results
3.1. Socio-Demographic Characteristics
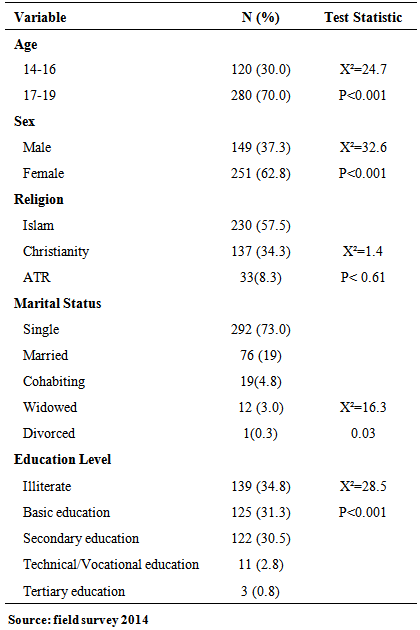
- The mean age of the respondents was 17.29 ± 1.38. Most of the respondents were between 17-19 years (70%) whilst those between 14-16 years constitute 30% of the study participants. Of this number, 62.8% were female and 38.2% male. On religious affiliation, 57.5% were Muslims, 34.3% Christians and the rest belong to other religions. On marital status, 19.0% were married, 73.0% single with 4.8% cohabiting. On their educational status, 34.8% were illiterates with 31.3% educated to the basic level and the rest from secondary to tertiary levels. A test of association between the socio-demographic characteristics of respondents and their use of contraceptives showed that respondents’ age has a significant relationship with the use of contraceptives. As the age of respondent increases, the likelihood of contraceptive use also increases (P<0.001 and X²=24.7). Sex of respondents was also found to be positively correlated with the use of contraceptives as more females were found to be using contraceptives than males (P<0.001 and X²=32.6). The same trend was established for the educational status of respondents; as the educational level of respondent increased, the more likely he/she is to use contraceptives (P<0.001 and X²=28.5). Marital status was also found to be statistically significant. However, the strength of association between marital status and contraceptives usage was not as strong as the other variables (P<0.03 and X²=16.3) as shown in table 1.
|
3.2. Knowledge of Contraceptives Methods and Practice
- Knowledge of respondents on the various contraceptives use show that majority of the respondents (74.8%), have knowledge of contraceptives, especially the male condoms. However, 3.3% had knowledge of tubal ligation and 3.8% on vasectomy. About 56.2% knew of the oral contraceptive pill and 51.8% showed knowledge of the Injectables, especially Depo Provera, with 9.8% indicating knowledge of Norplant. About 36.8% knew that contraceptives are used to limit births whilst 63.2% did not know that contraceptives are used to limit births. Additionally, only 29.3% were able to indicate that contraceptives are used to delay pregnancy, with 69.7% lacking knowledge on this. In the same vein, 77.3% indicated that contraceptives are used to prevent pregnancy.
3.3. Relationships with the Opposite Sex
- Results show that 49.5% of respondents either have a boyfriend or girlfriends. Out of this number, majority of them started their relationship 6 months prior to the study. About 8.8% indicated that they started the relationship within the past two years, 3.0% had their relationship more than 2 years preceding the study. With regard to the age at which the relationship started, 5.5% started before age 10. The results also show that majority of the respondents (76.3%) who were into relationships admitted that they engage in sexual activities with the opposite sex. For those who never engaged in sexual activities, the reasons given were that they are involved in distant relationships, making it very difficult for such activities to take place. With regard to those who engaged in sexual acts, the results show 38.8% indicating that adolescents engage in premarital sex due to curiosity whereas 28.5% attributed it to quest for financial gains or support from their partners. In addition, 12.0% indicated that parental neglect and low parental supervision was the reasons for premarital sex among teenagers. Figure 1 shows the reasons why teenagers engage in premarital sex.
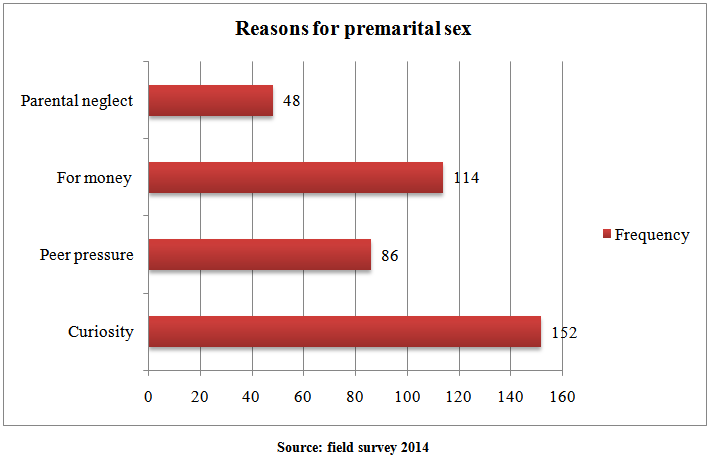 | Figure 1. Reasons for premarital sex |
3.4. Fertility and Family Size Preference
- The size of the nucleus family respondents belong to showed that some of them (33.5%) were in a family size of 3-4 people whilst 24.8% were in a family of seven (7) and above. The fertility preference of respondents was found to have a positive correlation with the family size of the respondents as majority of them (51.0%) said that they desire to give birth to 3-4 children in future. About 10.5% of them said that they desire to give birth to seven (7) or more children. This show that, the desire to give birth to more than seven (7) children declined (from 24.8% to 10.5%) when compared with the nucleus family of the respondents. There was however an increase in the number of respondents desiring a family size of 1 – 2 when compared with the parental background. Factors that were found to influence the fertility preference of respondents include their religious beliefs, traditional beliefs, their income level and their educational level. A number of the respondents (46.3%) said that their preference will be determined by their income level whilst 37.3% said that their fertility preference would be determined by their educational level.
3.5. Contraceptive Use among Adolescents
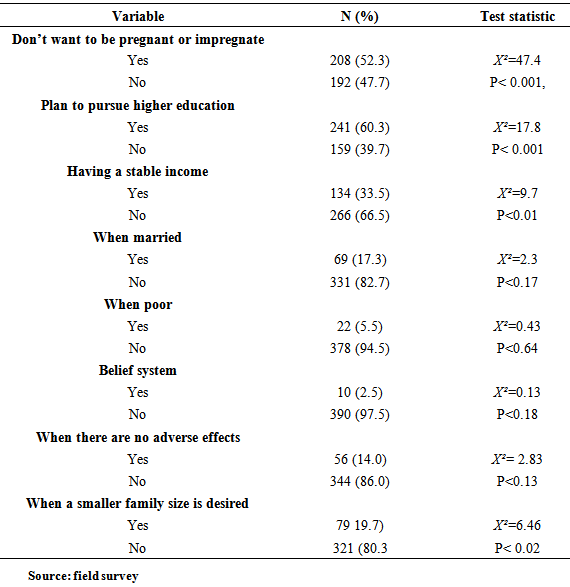
- The study results shows that only 20% of the respondents had ever used contraceptives whilst 80% indicated they never used contraceptives before. Among all contraceptives known to them condom was found to be the most widely used contraceptive method. Of those who have ever used contraceptives; 46.3% of them used the condom, 27.5% used the Injectable and 15.0% used the oral contraceptive pill. With regard to the preferred contraceptive, results show that the Injectable was the most preferred with 61.0%. However, none of the respondents preferred tubal ligation and vasectomy as they were represented (0%) among the respondents. Norplant and IUCD were also least preferred with 6.5% and 2.0% respectively. With respect to conditions under which they would rely on contraceptives, 49.3% said they would only use contraceptives if they don’t want to impregnate a girl or when a girl does not want to become pregnant. Interestingly, 15.3% indicated that they will only use contraceptives if their partners agree for them to use. An assessment of what determines contraceptives use among the adolescents showed that, the factors such as when they don’t intend becoming pregnant or impregnating somebody (P<0.001 and X²=47.4), plan to pursue a higher education (P< 0.001 and X²=17.8) and the desire to have a smaller family size (P<0.02 and X²=6.46). However, factors that also determines but were statistically significant include; when they are married (P< 0.17 and X²=2.3), when poor (P< 0.64 and X² = 0.43), belief system (P<0.18 and X²= 0. 013). Table 2 below shows the determinants of contraceptives utilization among adolescents.
|
3.6. Socio-cultural Barriers to Contraceptives Use
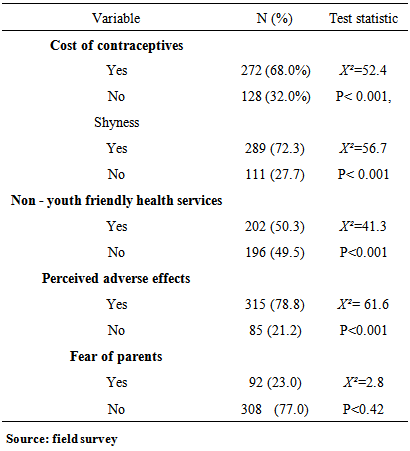
- Barriers that were found to hinder contraceptives use among adolescents were; cost of contraceptives (P<0.001 and X²=52.4), shyness in buying contraceptives (P<0.001 and X²=56.7), non- youth friendly health services (P<0.001 and 41.3) and perceived adverse effects of contraceptives (P < 0.001 and X²=61.6). It was also observed that fear of parents also serves as a hindrance but was not statistically significant as the test of association was insignificant (P< 0.42 and X² = 2.8). This is shown on table 3.
|
4. Discussion
- Ideally, it is expected that young people are provided with sexual and reproductive health information and services prior to sexual debut. Many of them, it must be noted, experience sexual debut long before marriage [22]. The findings show that 74.8.0% of the respondents have ever heard of contraceptives especially the male condom. This apparently may be due to the popularity of the male condom in the fight against HIV/AIDS. This result is similar to the findings by [23] who found that about 90% of adolescents reported of haven heard of contraceptive methods. Another important area worth mentioning is the source of information. This is crucial in determining the quality of the information given. Experts have argued that knowledge about the contraceptive methods is a determinant in its use [22]. In a study by [24; 25], women who ever heard about Injectable were significantly associated with current use of any contraceptive method. Apart from the condom, other known contraceptives in the study are the oral contraceptive pill (56.2%) and the Injectable (51.8%). This finding confirms the claim by [20] that the best known contraceptive method in Ghana is the male condom which was found to be familiar to 88% of females and 91% males. The results show that Norplant, vasectomy and tubal ligation were the least known methods 9.8%, 3.8% and 3.3% respectively. This supports [26] claim that methods such as sterilization (male/female), intrauterine device (IUD), and diaphragm, were least commonly known by most adolescents. With regard to the purpose for which contraceptives are used, 77.3% said that contraceptives are used to prevent pregnancy whilst 36.8% knew that contraceptives are used to limit births with 29.3% indicating that contraceptives are used to delay pregnancy. Similar findings were made in the Sekondi – Takoradi Metropolis of Ghana where 29.6% and 37.6% males and females, respectively, indicated that their purpose for the use of contraceptives is to prevent pregnancy [27]. This result is further confirmed by [28] study in Uganda which found that adolescents’ knowledge of contraception is related to the prevention of unwanted pregnancy. The prevention of pregnancy rather than STIs prevention is the single most important reason adolescents use contraceptives. These responses probably were as a result of the fact that their priority as unmarried couples is preventing pregnancy and not to delay it or avoid contracting STIs.A test of association between the socio-demographic characteristics of respondents and their use of contraceptives showed that age of respondents has a significant relationship with the use of contraceptives. As the age of respondent increases the more likely he or she is to use contraceptives (P<0.001 and X²=24.7). This appears to be consistent with the observation made by [29] that the rate of contraceptive use increased with the increase of age of adolescents. In the same vein, [24] has observed in a study that, adolescents whose ages were below 16 years and 16-18 years age groups were more likely to be current users of contraceptives than those whose ages were above 18 years. To assess the importance of education on contraceptive use, respondents revealed that they will use contraceptives if they plan to pursue higher education (P< 0.001 and X²=17.8). This finding therefore further suggest that education of the adolescent at least up to the senior high school level may be one important strategy that can lead to increase contraceptive uptake. It is an important determinant of contraceptive use and must therefore be taken seriously by stakeholders interested in current and future contraceptive use..The fertility preference of the respondents was found to have a positive correlation with the family size of the respondents as majority (51.0%) said they desire to give birth to 3-4 children in future. This corroborates the findings in [18] that suggest that the average number of children desired by women is 4. It has however contrasted the findings from the same study that, women in Northern region desire to have 6.6 children on average [26]. This may mean that there is a shift in the number of children desired by adolescents compared with their parents. It was also observed that factors such as religious and traditional beliefs, income and educational levels have great influence on the future fertility preference of adolescents. Majority of the respondents (46.3%) said their preference will be determined by their income level. This is contrary to the finding by [31] that suggests that 93.2% of adolescents would be influenced by their income. His findings therefore debunk the fact that a family’s income necessarily implies a larger family size, but rather, it indicates small family size. Relationship is an important factor in determining adolescent sexual engagement. Of the total number of respondents who were into boy or girl friend relationship, 76.3% were engaged in sexual activity. Sexual activity was observed to increase with increasing age. As observed by [23] in a study where sexual activity increases with age. This is worrying because it thus suggests that being in a boyfriend or girlfriend relationship in this environment is synonymous with engagement in sexual activity. Reasons advanced for engaging in sex are; curiosity (38.8%), financial gain or support (28.5%), and parental neglect and low parental supervision (12.0%). In their study, [32] found that, 41% of adolescents had already initiated sexual intercourse before 16 years of age, citing reasons such as curiosity, being forced by a boyfriend or it ‘just happened’. On the contrary, love for the partner was stated by 76% of respondents as being the main reason for adolescents engaging in sexual intercourse. Among these study participants, those who said they were not engaged in sexual activity gave reasons relating to distance between them and their partners, suggesting that they would have been engaged in sex had it not been for the distance. Further assessment of the maternity history of the female respondents show that 19.5% of the respondents had ever been pregnant with 4.8% ever experiencing miscarriage (abortion) and 14.5% of the respondents were found to have children. This confirms [18] report that overall, 13% of women age 15–19 are already mothers or are pregnant with their first child and that teenage child bearing in Northern and Central regions of Ghana have the highest of 23% [20]. The study results show that only 20% of the respondents had ever used contraceptives whilst the current contraceptive use was assessed to be 18.3%. The condom, Injectable and the pill were found to be the most widely used contraceptive methods among respondents. The condom was found to be the most widely used contraceptive method. About 46.3% of the respondents used the condom whilst 27.5% used the Injectable and 15.0% of respondents using the oral contraceptive pill. About 38.4% of the respondents who were currently using contraceptives were using the condom whilst 26.0% were currently using the Injectable, 13.7% were currently using the oral contraceptive pill. There was a similar finding by [27], in which those who indicated they often use the condom constituted 75.6% of the male and 27.3% of the female whereas 13.3% and 19.4% of the male and females respondents indicated they often use oral contraceptives. However [13] observed that Depo-Provera is becoming increasingly popular contraceptive method in the adolescent population which might have been influenced by the advantages associated with its use including lack of a need for daily compliance, interruption of foreplay, or cooperation of the male partner. The low condom use among this sample is worrying owing to the fact that condom use is the single most effective contraceptive method against STIs and HIV/AIDS. There appears to be low contraceptive acceptance rate among the male adolescents and effective strategies need to be designed to increase acceptance and use. Again, [33] observed that trends in methods of contraception used by adolescents over the past 2 decades have shown an increase in oral contraceptive pill (OCP) use and an increase in male condom use. In recent years, the number of adolescents reporting OCP use has remained stable at approximately 18% to 20% [14]. Adolescents are confronted with several barriers with regards to contraceptive use. In this study, the barriers that were found to prevent teenagers from using contraceptives were; perceived adverse effects of contraceptives (P< 0.001 and X²=61.6); shyness in buying contraceptives (P<0.001 and X²=56.7); the cost of contraceptives (P<0.001 and X²=52.4); and non-youth friendly health services (P<0.001 and X² = 41.3). This findings confirm those found among adolescents in Limpopo Province in which 60% of the respondents were not utilizing the health care services, giving reasons such as distance (9%), culturally not permitted (12%), shyness (21%), services not available (9%), and unfriendly staff (16%) [32]. Identifying and knowing these barriers is important in designing effective strategies that can help address the low contraceptive uptake among adolescents in our communities and the country as a whole. Health worker attitude is an important influencing factor to contraceptive use. The study found that, non-youth friendliness of the health worker is a barrier to contraceptive use. This is confirmed by [32] when they found that 42% of respondents in their study felt that health care providers needed to display a positive attitude towards them; (be caring, be patient, be friendly, and improve on communication). Similarly, study results showed that 40.0% of the males and 37.6% of the females said they choose particular service providers because of their friendly attitude towards them [27]. One of the fears that adolescents often express is that fact that the service providers may reveal their identities to their parents, relatives and friends [27]. Since most contraceptives are still provider - dependent in that they requires the client to return to a health care professional's clinic, drug store of pharmacy shop for continuation of the contraceptive method, the health worker needs to be more receptive towards the adolescent seeking contraceptives.
5. Conclusions
- The great potential of contraceptives being used to prevent unwanted pregnancies particularly among the adolescents who constitute majority of the population in Ghana is far from being realized. The study shows that though the general knowledge of contraceptive is fair, the correct knowledge of use of contraceptives is grossly deficient. It has also been observed that contraceptives that are constantly advertised are more in use than the unfamiliar ones that are not advertised. Therefore education is needed to ensure a balance in the use of contraceptives and to make them understand the different uses it is put. There is also the need to establish youth friendly health centres to encourage utilization and exposure to health information.