-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(3): 67-72
doi:10.5923/j.phr.20150503.01
Hypertension and Its Risk Factors – A Cross Sectional Study in an Urban Population of a North Indian District
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRenu Rani1, Vijay Mengi1, Rajiv Kumar Gupta1, Harash K. Sharma2
1PG Deptt of Community Medicine, GMC Jammu, India
2J&K Health Department, Jammu, India
Correspondence to: Renu Rani, PG Deptt of Community Medicine, GMC Jammu, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Background: Non communicable diseases are on the rise at an alarming rate among adult population both in developed and developing world. Among the various risk factors for non communicable diseases hypertension isa significant risk factor in cardiovascular diseases. The study aimed to assess various risk factors and their association with hypertension. MaterialsandMethods: ACross sectionalcommunity based study was conducted in an urban population aged 30 yrs and above in an urban locality of Jammu district of J&K. Every alternate house was visited thus covering 50% of total houses. Standard oral questionnaire, predesigned and pretested was used to obtain information on risk factors for hypertension. Results:Among the risk factors studied for hypertension age, sex, educational status, BMI, alcohol intake and physical inactivity were found to be statistically significant, while no significant association could be found with non vegetarian diet and extra salt intake. Conclusions:Advancing age, male sex, higher BMI, alcohol consumption and physical inactivity were found to be important risk factors for hypertension.
Keywords: Risk factor, Hypertension, Urban area
Cite this paper: Renu Rani, Vijay Mengi, Rajiv Kumar Gupta, Harash K. Sharma, Hypertension and Its Risk Factors – A Cross Sectional Study in an Urban Population of a North Indian District, Public Health Research, Vol. 5 No. 3, 2015, pp. 67-72. doi: 10.5923/j.phr.20150503.01.
Article Outline
1. Introduction
- Hypertension, a chronic non communicable disease, also known as high or raised blood pressure, is a global public health issue. Populations in low and middle income countries are disproportionately affected as they have weak health systems. Globally cardiovascular diseases account for approximately 17 million deaths a year, nearly one third of the total. Of these, complications of hypertension account for 9.4 million deaths worldwide every year. Hypertension is responsible for at least 45% of deaths due to heart disease, and 51% of deaths due to stroke. It contributes to the burden of heart disease, stroke and kidney failure and leads to premature mortality and disability.Hypertension is usually asymptomatic in the initial stages and many people go undiagnosed. Those who are diagnosed may not have access to treatment and may not be able to successfully control their illness over the long term [1]. As the disease has long latent period before it manifests as a clinical entity, and generally being asymptomatic during its clinical course, its detection as well as control is a major public health challenge in both developed and developing countries. Factors that predispose to hypertension vary from country to country and even within different places of the same country. Due to rapid urbanisation & social changes new risk factors of hypertension are also emerging [2]. The major risk factors include ethnicity, obesity, diabetes, age, sex, alcoholism, sedentary lifestyle, diet (including salt intake), and family history of hypertension. Life style modification and medical management can ameliorate the effects of some of these risk factors [3].For prevention of serious consequences of hypertension knowledge of its risk factors is important. Community based studies on hypertension and associated risk factors in urban areas are scarce, so it was in this context that the present study was undertaken to determine risk factors and their association with hypertension.
2. Material and Methods
- This cross-sectional one point analysis of risk factors for hypertension, was conducted in Trikuta nagar area of Jammu district in an urban adult population of age ≥ 30 yrs. The area falls under the Department of Community Medicine, Government Medical College, Jammu. Before the start of the study, clearance from Institutional Ethics Committee was duly sought. The investigators covered every alternate house in the locality thus enumerating half of the total houses during the study period. The head of the family was first contacted and in case he /she was absent or unable to respond next responsible person of the family was contacted and after explaining the purpose of the study, information was collected. The subjects who could not be contacted during first visit were tried to be enrolled during second visit, after which they were excluded. All the family members who were of age 30 yrs and above were interviewed using predesigned pretested questionnaire regarding their personal habits like smoking, its duration and frequency, alcohol consumption, its current status i.e. presently alcoholic or non-alcoholic and duration since consuming the alcohol, their eating habits i.e. whether vegetarian or non vegetarian, if taking extra table salt with meals. Family history of hypertension was also obtained from participants. Information on physical activity was collected and subjects classified into sedentary, moderate & heavy workers based on recommendation of WHO expert committee [4]. The study subjects were classified on the basis of Kuppuswamy socio-economic scale and those already diagnosed and taking anti-hypertensives were classified as hypertensives for the purpose of the present study.Weight and height of all the persons in the study population were recorded to calculate the body mass index (BMI). The data thus collected was compiled, tabulated and statistically analysed using Epi-info 6.04 version. Chi square test was used to find the association and values <0.05 were considered significant.
3. Results
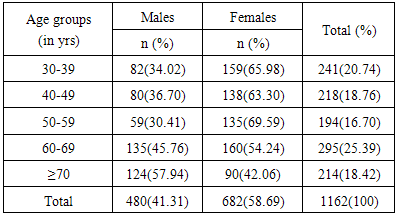
- A total of 528 houses were surveyed during the course of study. A total of 480 males (41.31%) and 682(58.69%) females comprised the study population of 1162 (table 1). Of the surveyed population, 653/1162(56.20%) comprised of people age <60 yrs while 509/1162 (43.80%) were of more than 60 yrs. Trend analysis of hypertensive patients showed a rising trend in relation to age from 40-49 years progressively with marked rise from fifth decade onwards (Fig.1). 1141/1162(98.88%) of study population belonged to upper and upper middle class. None belonged to “upper lower” and “lower class” in the study population (table 2). Majority of males 400/480 (83.33%) in the study population had an educational qualification of graduation and above. Among females, 451/682(66.13%) were graduate and above. Majority of the families were Hindus i.e. 468/528(88.64%) followed by Sikh families 45/528(8.53%). Out of 1162 study subjects, 672 were found to be hypertensives. Hypertension was more prevalent among people who had received education up to high school or below. Prevalence was also higher among those consuming alcohol 80/117(68.38%) as compared to those not consuming alcohol 592/1045(56.65%) and as the duration since alcohol intake increased from <5yrs to >15 yrs the prevalence of hypertension also increased from 33.33% to 78.13% (Fig.2). Higher proportion of hypertension was found among sedentary workers 610/1023 (59.63%) as compared to moderate workers in whom prevalence of hypertension was found to be 62/139 (44.60%). The results also revealed that study subjects who had BMI ≥25 had higher proportion i.e. 499/803(62.14%) as hypertensives.
 | Figure 1. Trend analysis of hypertension with age |
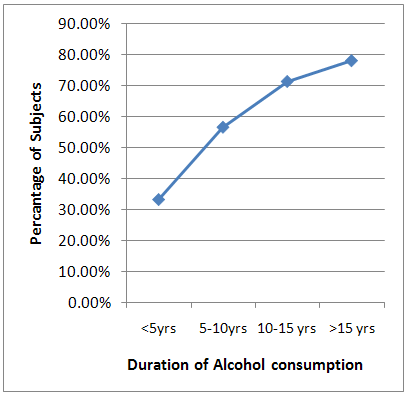 | Figure 2. Trend analysis of duration of alcohol intake with hypertension |
|
|

|

4. Discussion
- The results of the present study revealed that 57.83% of the study subjects were suffering from hypertension. Among the various risk factors studied, highly significant association of hypertension was observed with age. Prevalence increased steadily with age and was more in ≥70 yrs age group as compared to younger age groups. The similar association of hypertension with age has been documented in different studies [2, 5, 6].In the present study higher proportion of males were suffering from hypertension 313/480(65.21%) as compared to females 359/682(52.4%) and the association of sex with hypertension was also found to be statistically significant. Other studies conducted in India by Yadav S et al [5], Chandwani H et al [6], Madhu Kumar S [7], Madhumita M [8], and abroad in Addis Ababas [9] also reported similar results. In contrast to our results higher prevalence of hypertension has been reported in females in studies conducted by Gupta PC et al [10].Significant association of hypertension was found with low level of education in the current study. As the education decreased from graduation towards illiteracy the hypertension prevalence also increased. Our results are in agreement with those reported by other authors [11, 12, 13]. Similar statistically significant results were observed in a study [14] in Sao Paulo Brazil which shows 49.5% of illiterate individuals had hypertension and only 12.7% of the individuals who had completed university education level had hypertension. However in a study by Sidhu S et al [15] on adult Punjabi females literacy wise distribution of cases of hypertension suggested that the prevalence of hypertension was higher among literates (25.54%) than illiterates (18.54%) & results were statistically significant. Higher prevalence of hypertension with lower educational level may be due to lesser awareness about disease and lower knowledge of how to prevent the disease.The prevalence of hypertension was higher among non-smokers 649/1119(58%) as compared to smokers 23/43 (53.49%). This association however, was not found to be statistically significant. However, the numbers of smokers in present study were found to be very low (n=43). The results concur with a study conducted by Singh RB et al [16]. In contrast to present study significant association between hypertension and smoking was found in studies conducted by Reddy SS et al [17] and Patniak et al [18].The prevalence of hypertension in the current study was higher among those consuming alcohol 80/117(68.38%) as compared to those not consuming alcohol 592/1045 (56.65%) and results were statistically significant. Similar association has been found in other studies [2, 3, 6, 19, 20]. It was further found in the current study that as the duration since alcohol intake increased from <5yrs to >15 yrs the prevalence of hypertension also increased from 3/9(33.33%) to 50/64(78.13%) and it was statistically significant. Higher proportion of hypertension was found among sedentary workers 610/1023(59.63%) as compared to moderate workers in whom prevalence of hypertension was found to be 62/139(44.60%) and this finding was also statistically significant. Similar association was found in other Indian [21, 22] and international [3, 12, 23] studies. In the Indian meals, salt intake depends on several sources: salt used in cooking, salt added at the table directly and in the form of pickles, pappads etc. In current study, hypertension was more prevalent in subjects taking extra salts & /or pickles with meals 409/692 (59.10%) as compared to those who did not take extra salt and/or pickles 263/470 (55.96%). However, no statistically significant association was found between extra salt intake and hypertension. Similar findings have been reported in studies conducted by Tesfaye F et al [9], Freitas et al [14]. In contrast to current study, extra salt intake was found to be significantly associated with hypertension in other studies [2, 19, 24].In current study higher proportion of subjects with hypertension 310/517(59.98%) were non vegetarian as compared to 362/645 (56.13%) subjects who were hypertensive but vegetarian, however this finding was statistically insignificant. Results of current study are consistent with study conducted by Reddy SS et al [17]. However, in contrast to present study statistically significant association was found between hypertension and non vegetarian diet in a study conducted by Chandwani H et al [6]. Family history of hypertension was not found to be significantly associated with hypertension in the current study. However, many other studies [5, 6, 19, 25] have shown statistically significant association between hypertension and family history. Highly significant association was found between hypertension and BMI in current study. Higher proportion of subjects with hypertension 499/803(62.14%) had BMI ≥25 as compared to 173/359(48.19%) subjects with hypertension who were having BMI < 25. Similar results were reported in studies conducted by Reddy SS et al [17], Patnaik L et al [18] and, and other studies conducted on urban population by Mandal PK et al [2], Goma FM et al [3] and Chandwani H et al [6].Though prevalence of hypertension in current study was found to be more among professionals 130/203(64.04%), unemployed 9/14(64.29%) and semi professionals 147/238(61.76%) respectively but results were found to be statistically insignificant. However in a study on rural household community Muglivakkam, Tamilnadu [26] higher prevalence of hypertension was found in unemployed category & unskilled category and was statistically significant. Hamden et al [12] found higher prevalence of hypertension in retired & unemployed subjects whereas Reddy et al [17] in his study observed higher prevalence of hypertension in business occupation as compared to professionals. It would be pertinent to mention here that different occupational classifications were used by different authors.
5. Limitations
- 1. The subjects were chosen from single locality and thus may not be representative of whole urban area of Jammu. 2. Majority of study population belonged to upper and upper middle class thus all the strata of the society are not represented so the study may not be generalizable.3. Dietary salt intake was assessed by inquiring about added salt i.e. adding salt after food has been served and/or pickles intake (during a meal) which is a qualitative approach. Due to the cross sectional design of the study we might have failed to establish association between extra salt intake and hypertension in those subjects who had changed their behaviour after being diagnosed to have hypertension. Quantitative account for salt intake was not used as it has its own limitations [14] and because of technical constraints. 4. Our information regarding family history of hypertension was not based on documented medical records but merely on the basis of awareness & recall of the subjects.
6. Conclusions
- The present study concluded with the findings that advancing age, male sex, lower educational status, alcohol consumption, increasing BMI are important risk factors for hypertension.