-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2015; 5(1): 28-31
doi:10.5923/j.phr.20150501.05
The Influence of Parents' Educational Level in Children's Oral Health Behavior
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLArdérius A. 1, Veiga N. 1, Godinho M. 1, Ribeiro C. 2
1Health Sciences Department – Portuguese Catholic University, Viseu, Portugal
2Centro Hospitalar do Porto – Hospital Santo António, Porto, Portugal
Correspondence to: Ribeiro C. , Centro Hospitalar do Porto – Hospital Santo António, Porto, Portugal.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Introduction: The impact of oral health in people's quality of life has received an increasing attention by health professionals. The prevalence of oral pathologies and the lack of simple, affordable and effective preventive measures led the World Health Organization (WHO) to draw ambitious goals based on oral health promotion and prevention. Prevention should begin, preferentially, within the family aggregate and continue at school, in order to teach children and adolescents adequate oral health behaviors. Objective: Assessment children’s oral health status and analyze the association of their oral health behaviors with their parents' educational level. Participants and Methods: We conducted an epidemiological, observational, cross-sectional study in a sample of children from nursery and primary schools in Nelas, Portugal. Data was collected by the application of questionnaires to parents about their children oral health behaviors and the household’s oral hygiene habits and an intra-oral examination was accomplished to assess the decayed, missing and filled deciduous tooth index (dmft index) and the prevalence of fissure sealants. Data collection was performed by using the Statistical Package for Social Sciences (SPSS 20.0). For the analysis of the continuous variables we used measures of central tendency (mean) and dispersion measures (standard deviation). Prevalence was express as proportions (percentages). In order to test the variables' independence, it was used the Pearson's chi-square test and the Fisher's Exact Test, using a significance level of 5% (p=0.05). Results: Data was collected from 499 children aged between 3 and 11 years old. Four variables were significantly associated with the parents' educational level: toothbrushing frequency (p=0.015) toothbrushing duration (p=0.018) parental help during toothbrushing (p=0.012) and the frequency of dental appointments during the last twelve months (p=0.012). According to the data collection of the intraoral observation, we verified a mean dmft of 2.06 with a standard deviation of ± 2.36 and a mean fissure sealants of 1.1 ± 1.55. As for dmft index and the number of fissure sealants we have not found a statistically significant association with parents´educational level. Conclusions: The parents’ educational is associated with the oral health behaviors developed by their children. This can be justified by the fact that a higher level of education permits the acquisition of higher levels of knowledge and information about healthier daily habits.
Keywords: Oral health, Quality of life, Parents' educational level
Cite this paper: Ardérius A. , Veiga N. , Godinho M. , Ribeiro C. , The Influence of Parents' Educational Level in Children's Oral Health Behavior, Public Health Research, Vol. 5 No. 1, 2015, pp. 28-31. doi: 10.5923/j.phr.20150501.05.
1. Introduction
- Nowadays, oral diseases are considered a major barrier concerning people's quality of life, because they affect several aspects such as chewing, speech, appearance and interpersonal relationships. However, if properly prevented or treated in an early stage, oral pathologies such as dental caries and periodontal disease are highly preventable, with low economical costs and high health gains.Epidemiological data confirms a variation in dental caries prevalence inside a country, a district or even within a town, since this pathology is influenced by social and demographic inequalities [1-4].Childhood is a critical period for acquiring knowledge and habits, which may reflect later on their health behavior patterns [5].It has been shown that a child’s oral hygiene patterns are influenced by socioeconomical conditions and parent´s oral health behaviors [2, 4-6]. A family with low socioeconomic status, low monthly income and low educational levels is associated with deficient oral hygiene and a higher risk of more frequent and severe oral pathologies. These families can’t afford an appointment to the dentist or buy oral hygiene products and they have a knowledge deficit concerning health and oral hygiene habits [3, 4, 7, 8].Some studies show that the mother's oral status and her health determinants directly affect their children's oral health. This can occur due to many different factors, that have already been reported, such as the gestational component, oral hygiene, diet, dental appointments frequency and parents’ anxiety / nervousness towards the dental appointments [1, 6, 9].There are several prevention strategies that can be carried out not only by the dentist but also by parents and teachers. We can point out strategies such as anticariogenic diet habits, toothbrushing at least twice a day and daily flossing [5, 7-9]. Dental appointments should be performed twice a year, since there are preventive methods that can only be carried out by these health professionals, such as topic fluoride application and fissure sealants [3]. The prevalence of dental caries in fissures has increased when compared to occlusal surfaces. This type of dental caries is nowadays, the largest contribution towards decayed, missing and filled teeth values (dmft). Such data increases fissure sealants' importance, making them a valuable preventive measure, mainly among the young [10]. The purpose of this study was to assess children’s oral health status and analyze the association of their oral health behaviors with their parents' educational level.
2. Participants and Methods
- An epidemiological, observational, cross-sectional study was conducted in the town of Nelas, district of Viseu, Portugal. Data collection was carried out from March to May of 2013. This study included children aged from 3 to11 years old, from both genders with authorization and informed consent of their parents. At first, parents were given questionnaires to assess the children's oral health behaviors. Then, an intraoral examination was performed (to avoid bias) using an intraoral mirror and a WHO probe. The observation was accomplished in the classroom with both natural and artificial light. Children's oral health status was assessed by calculating the dmft of each individual. It has been respected the diagnostic criteria recommended by the WHO. Data was provided on a voluntary basis and its confidentiality was assured. This sample consisted of 499 children. Due to age discrepancy, children were grouped together for a careful data analysis, 3-6 years old with 28.7% (n=143), 7-8 years old with 41.1% (n=205) and 9-11 years old with 30.3% (n=151). Of the initial sample, 83.8% (n=418) were submitted to a clinical examination and 77.6% (n = 387) of the parents completed the questionnaire.Through the questionnaire, we assessed parents' educational level and we found that 4.1% (n=16) had just four years of schooling, 67.1% (n=259) had from four to twelve years of schooling, while 28.8% (n=111) had a higher degree (university level). We also collected data regarding the children's oral health, such as frequency and toothbrushing duration, parental help during toothbrushing and appointments to the dentist in the last twelve months.Data collection was performed by using the Statistical Program for Social Sciences (SPSS 20.0). For the analysis of the continuous variables we used measures of central tendency (mean) and dispersion measures (standard deviation). Prevalence was expressed as proportions (percentages). In order to test the variables' independence, it was used the Pearson's chi-square test and the Fisher's Exact Test, using a significance level of 5% (p=0.05).
3. Results
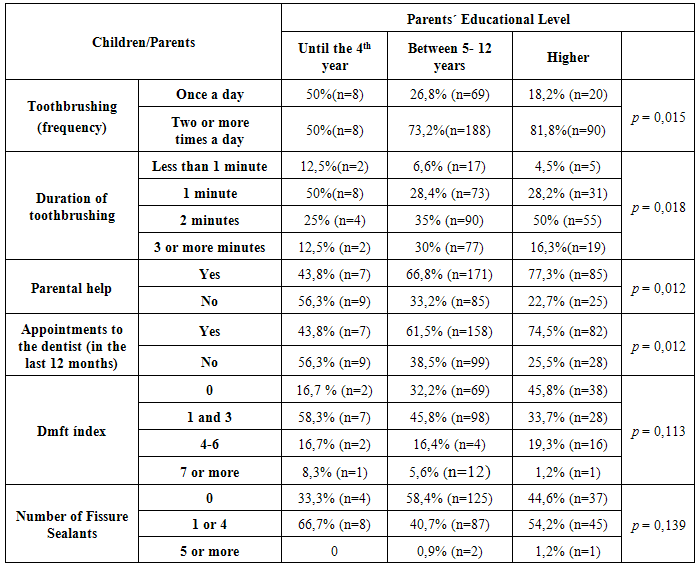
- From the 499 children participating in the study, 262 were boys and 237 were girls, with an average age of 7, 42 ± 1.76 years. Parents reported that 25.1% (n=98) of the children toothbrush their teeth once a day, while 74.9% (n = 286) said that their children toothbrush their teeth at least twice a day. Regarding the toothbrushing duration, 6.3% (n=24) stated that it takes less than 1 minute, 29.2% (n=112) said it takes 1 minute, 38.9% (n=149) spends 2 minutes and 25.6% (n=98) mentioned that the toothbrushing time is less than 3 minutes. When asked if they provided help while the children brushed their teeth, 68.8% (n=263) said “yes” while 31.2% (n=119) said “no”. Concerning the number of dental appointments in the last twelve months, we obtained a variable number of answers: 35.5% (n=136) had no appointments during the past twelve months, 27.9% (n=107) had 1 appointment, 23.8% (n=91) had 2 appointments, 7.3% (n=28) had 3 appointments, 2.4% (n=9) had 4 appointments, 0.5% (n=2) went there 5 times, 1.6% (n=6) went there 6 times, 0.3% (n=1) went there 7 times and there is still 0.8% (n=3) that went 10 times to the dentist in the last twelve months. Children went to the dentist on a routine basis (36.1%), in emergency situations (9.6%), for dental caries treatment (35.4%) and fissure sealants application (18.9%) (table 1). After applying the Chi-square, we confirmed that the parents' educational levels significantly affect children's frequency and toothbrushing duration, as well as the need of regular appointments to the dentist and their perception of providing help when toothbrushing (p<0.05).According to the data collection of the intraoral observation, we verified a mean dmft of 2.06 with a standard deviation of ± 2.36 and a mean fissure sealants of 1.1 ± 1.55. The dmft index was categorized in 4 groups, distributed as follows: 36.1% (n=151) children who have a dmft index = 0, 40.4% (n=169) children who have a dmft index between 1 and 3, 18.2% (n=76) those who have a dmft index between 4 and 6, while 5.3% (n=22) have a dmft index equal or higher than 7 (table 1).We analyzed data gathered on the fissure sealants (n=439). In the sample we found the presence of sealants fully intact in 53% (n=231), total sealants infiltrated without dental caries in 1% (n=5), infiltrated sealants with dental caries in 5% (n=24), partial sealants without dental caries in 40% (n=174) and partial sealants with dental caries in 1% (n=5) (table 1).However, although there is a tendency for educational level to influence dmft and the presence of fissure sealants, we didn´t find any significant statistical association.
|
4. Discussion
- Oral health has an important role in the individuals’ well-being [1, 5]. Parents have a strong influence on child's development in the first years, so their involvement benefits oral health pathologies prevention, such as dental caries [1]. This study assessed some parental characteristics and behaviors that may neglect children's oral health. The results of our study allow us to verify that educational level of parents influence children’s oral health habits, as referred in recent studies from Campbell et al. (2011) [8], Isong et al. (2010) [6], Van den Branden et al. (2012) [7] Bozorgmehr et al. (2013) [1]. The reasons presented by Van den Branden point out to economical difficulties, limited access to information and interaction with healthcare professionals [7]. Oral health guidance is not only a dental professional´s task, but of all healthcare professionals [8].In this sample, 74.7% of the children toothbrush their teeth at least twice a day. This value is higher than reported by Costa et al. [11] (68%) and much higher when compared with the values obtained by Mathur et al. (35.8%) [12]. However, in this study 25.3% of children toothbrush only once a day. Like the study by Vallejos-Sanchez et al. [13], toothbrushing frequency is related to parents’ educational level and it was found that children whose parents have a higher level of instruction brush their teeth more often. Razmienė et al. [14] observed that dental caries was influenced by toothbrushing frequency; however the study conducted by Sarumathi et al. [15] didn’t reach the same conclusions.In order to be effective, toothbrushing demands parental supervision [3]. In our study, we found that approximately 68.9% help their children brushing their teeth. Amin et al. [16] in a similar study, found that 80.8% instructed their children during toothbrushing and that it was really important for reducing dmft.Dental appointments should begin before the first year of age, continuing, at least, twice a year [3, 6]. Therefore, professionals can teach parents and children for a proper oral hygiene [3]. In the past 12 months, 35.5% of the children did not have a dental appointment. However 64.5% went to the dentist at least one time and 36.6% of children followed the recommendations and had a dental appointment at least twice a year. We can state that children, whose parents have a higher education level, have a lower dmft index, which is in accordance with the study by Oulis et al. [17] Sarumathi et al. [15], Borges et al. [18] and Amin et al. [16].Fissure sealants application is not directly related to parents’ educational level. This can be explained by the implementation of the governmental oral health program, which decreases the social and economical differences in oral treatments.
5. Conclusions
- The results can bring a perception of the relation between certain factors that influence parents and their children's oral health status. It is important to reinforce and promote the preventive measures so that the information can reach the populations. Prevention should start, preferentially, within the family and continue in the school environment. The school is the ideal place for the development of oral health programs, allowing children and young people to learn healthy oral behaviors.The focus on education and training should continue and grow, because populations with a higher level of education have more knowledge and information. This population uses their knowledge better, allowing them to establish more effective preventive measures, achieving a reduction of costs and effective health gains.