-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2014; 4(5): 210-218
doi:10.5923/j.phr.20140405.09
Analysis of the Spatial Distribution of Health Facilities in Benue State, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFanan Ujoh, Felix Kwaghsende
Department of Urban and Regional Planning, Benue State University, Makurdi, Nigeria
Correspondence to: Fanan Ujoh, Department of Urban and Regional Planning, Benue State University, Makurdi, Nigeria.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
The provision of adequate and equitable basic health services is becoming increasingly difficult due to rapid population growth, rising poverty levels and lack of available resources. One of the imperatives of health care provision is a concern for both social and spatial justice. This study is an attempt to examine the spatial distribution of health facilities in Benue State. The perspective taken is spatial and focuses on the problem of inadequacy and inequality of public health facilities among populations in Benue state. Health infrastructure provision within the State is analyzed along three lines: between Local Government Areas (LGAs) of the state; between senatorial zones; and on the basis of population per facility using secondary data on number of health care facilities. The study shows that although public health care facilities were nearly equally distributed among the 3 senatorial districts of the state, variations exists between the LGAs and within each senatorial district in terms of the overall distribution of health facilities(public and private). In terms of existing relationship between population and number of health facilities provided, the R-square value of .564 explained the variance in number of health facilities to population. The implications of the mal-distribution manifest in overcrowding and consequent lack of proper attention to patients as well as poor access in some specific LGAs with vulnerable conditions of low number of health facilities especially among the rural dwellers. The study recommends a more robust investigation in the existing health care facilities with a view to establishing the levels of health manpower available, bedding and other facilities as well as the actual access levels individuals and communities have to health care facilities in Benue State.
Keywords: Spatial injustice, Health infrastructure, Senatorial districts, Benue state
Cite this paper: Fanan Ujoh, Felix Kwaghsende, Analysis of the Spatial Distribution of Health Facilities in Benue State, Nigeria, Public Health Research, Vol. 4 No. 5, 2014, pp. 210-218. doi: 10.5923/j.phr.20140405.09.
Article Outline
1. Introduction
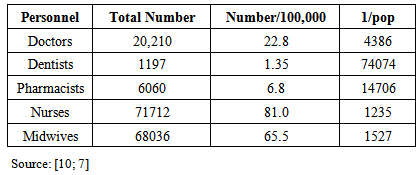
- Health is a universal human right and focus of social and political concern worldwide. The WHO [1] defines health as “a state of complete physical, mental and social well-being”. Such an ideal state may be desirable but is practically limited as most of humanity would be unhealthy at all times and in many cases without access to health services. Hence, healthcare institutions are service-oriented establishments that provide medical care facilities comprising of observational, diagnostic, research and therapeutic and rehabilitative services to the public. Adequate and effective distribution of health care facilities contributes immensely to health care service provision and needs of the people. According to Berman [2], upon independence, most sub-Saharan African countries attempted to provide universal health services to the population through primary healthcare provisions. But the emerging situation where the carrying capacity of existing public health systems declines in the face of a growing need for essential/basic health care simply reveals the rapidly diminishing ability of governments to provide public resources for effective healthcare delivery [3]. The provision of adequate basic health services in developing countries is becoming increasingly difficult by the day. Rapid population growth, widespread poverty and lack of financial resources for the provision of health facilities/infrastructure are identified as the key factors responsible for the poor health care delivery systems in the developing world [3-5].In the health sector, much concern has been expressed pertaining to the pattern of distribution of heath care facilities and level of utilization. According to Inyang [6], distributive equity in healthcare facilities indexes accessibility. In other words, the level of access to health care facilities is a function of the degree of fairness in spatial distribution of the facilities. According to Atser and Akpan [7], inequality in facilities’ distribution is of crucial significance particularly in developing societies where there are dual problems of limited facilities and low personal mobility. Accessibility in this context has spatial theme and signifies the ease with which potential health care seekers get to the health facilities where health care services are delivered. The past National Development Plans have reflected the problems of equitable distribution of health care facilities in the country while regional studies [6-8] have confirmed the existence of inequality in the distribution of health care facilities in Nigeria. The national health policy aims to achieve health for all Nigerians based on the national philosophy of social justice and equity as clearly enunciated in the second National Development Plan of 1970-1974. These principles of social justice and equity and the ideals of freedom and opportunity have been affirmed in Nigeria’s constitution. Thus, the national health policy was formulated in the context of these national objectives and philosophy. To this end, the primary health care is adopted as the means of achieving the national goal of social justice and equity. As defined in Alma-Ata Declaration of 1978, “primary health care... brings health care as close as possible to where people live and work….” [9].Inyang [6] observed that the problem in the health care sector is not so much on the quality of services rendered but on adequacy of health facilities provided. The quality of services rendered is related to the level of manpower available. Although, WHO asserted that Nigeria is yet to develop a health manpower plan that describes the categories and number of personnel required taking into account current status [9], the health manpower level in Nigeria (Table 1) seem to be within acceptable standard for the developing countries.
|
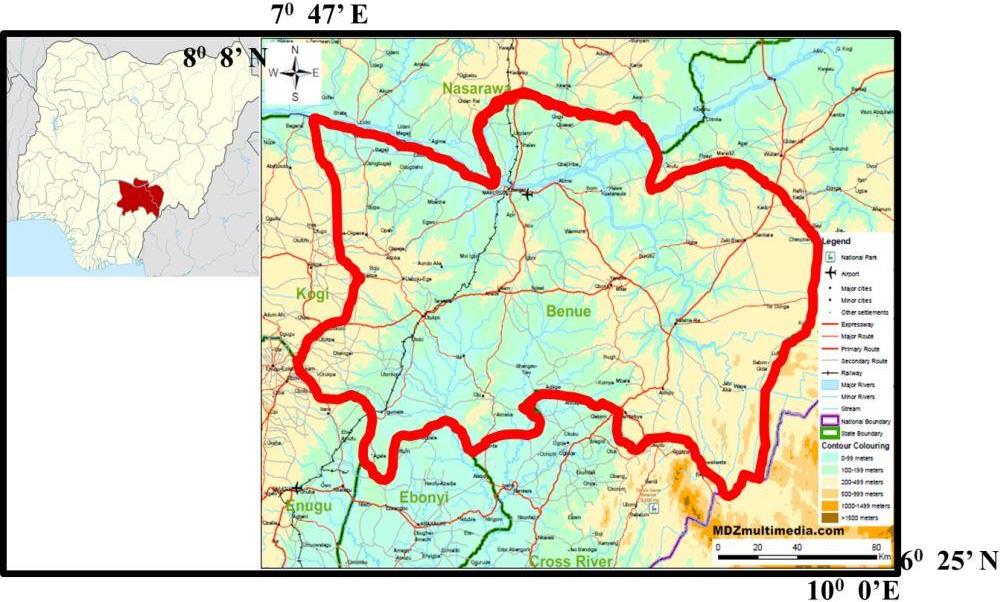 | Figure 1. Study Area |
|
|
|
2. Methodology
2.1. Study Area
- Benue state is the study area. It is located between Longitude 7° 47’ and 10° 0’ East, and Latitude 6° 25’ and 8° 8’ North, and is bounded to the North by Nasarawa state, to the West by Kogi State, to the East by Taraba state and the Cameroun Republic, and to the South by Cross-River and Enugu states (Figure 1). Created on 3rd February, 1976, the State has 23 LGAs and 3 Senatorial Districts, with Makurdi as its capital. The population of the State grew from 2,780,393 persons in 1991 [19] to 4,138,166 persons in 2006 [20] and a projected figure of 5,485,019 persons in 2014 using an annual growth rate of 3%. The ethnic and socio-cultural composition of the population is diverse, comprising the Tiv, Idoma, Igede, Etulo, Jukun, Hausa, Abakwa as well as other ethnic nationalities. There are 3 levels of health care delivery in Benue state. These are the tertiary, secondary and primary levels. The second largest River in Nigeria (the Benue) is by far the most prominent geographical feature in the State. The area is well drained and has a temperature that fluctuates between 23°C to 34°C for most part of the year [21]. With a mean annual rainfall of between 150mm to 180mm and an estimated area of 30,955 km2, Benue state stretches across the transition belt between the forest and savannah vegetation, covering a vast and fertile landmass which is worked by a farming population.
2.2. Method of Data Analysis
- The secondary data used for this study was generated from the Health Management Information System (HMIS) of the Benue State Ministry of Health, Makurdi. The health care facilities’ records used are for the year 2014 which are most recent. Using the 2006 population census figures of each LGA, the population was projected to 2014 using an annual growth rate of 3%. Focused group discussion with some officials of the Benue State Ministry of Health, Makurdi (in addition to knowledge of the study area of over 25 years) also formed part of the methodology for acquiring information used in this study. To explore the influence of types of health facilities (Primary and Secondary) and geo-political zones on the number of health facilities provision, data on health facilities by types and zones were subjected to factorial analysis of variance using factorial uni-variate ANOVA design. This is an extension of one-way ANOVA in that it involves the analysis of two or more independent variables at a time. It allows for assessing the influence of each independent variable separately as well as joint or interaction effects of variables. The independent variables were measured as discrete variables and as such were coded using nominal scale. Thus: Zones (A = 1; B =2 and C = 3); and types of the health facilities (Primary =1, Secondary =2). The dependent variable was the number of health care facilities. Pearson Product Moment Correlation analysis was applied to investigate the relationship between population and number of health care facilities on LGA basis while tables and graphs were used in the display of the data.
3. Results
3.1. Levels of Health Facilities in Benue State
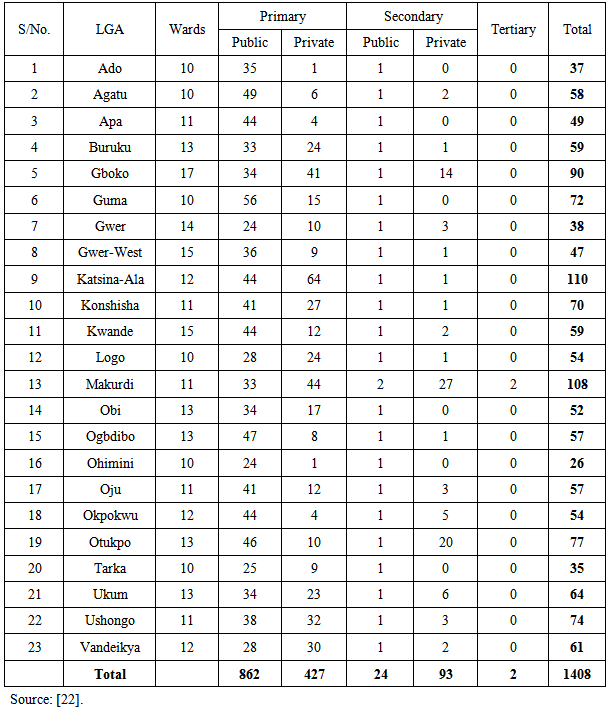
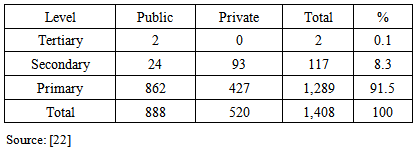
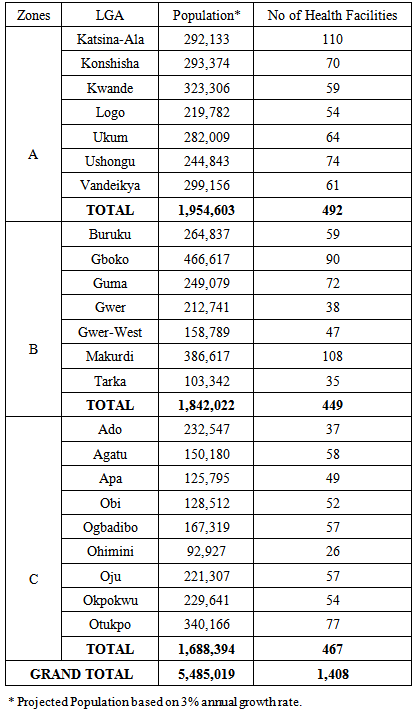
- The distribution of health facilities across LGAs in Benue State is analyzed from different spatial perspectives. There are basically 3 levels of healthcare provision in the State (primary, secondary and tertiary) distributed among the LGAs. A total of 1,408 health facilities exist in the state among the 23 LGAs out of which two are of tertiary levels (Federal Medical Centre, Makurdi and the Benue State University Teaching Hospital, Makurdi). A total of 117 are of secondary levels while 1,289 are primary health care facilities. Their ownership comprises both public and private. The spatial distribution among the LGAs shows that variations exist in both numbers and types/levels of health care facilities available for use by the people as presented in Table 4 while Table 5 presents a summary of the health care facilities distribution by levels and ownership status.
|
3.2. Relationship between Population and Number of Health Facilities
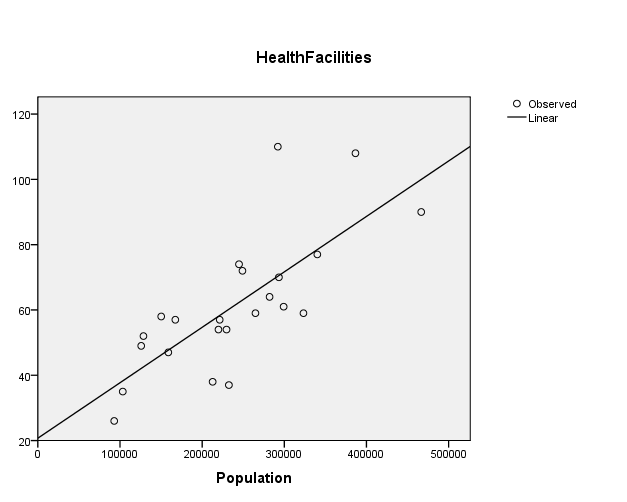
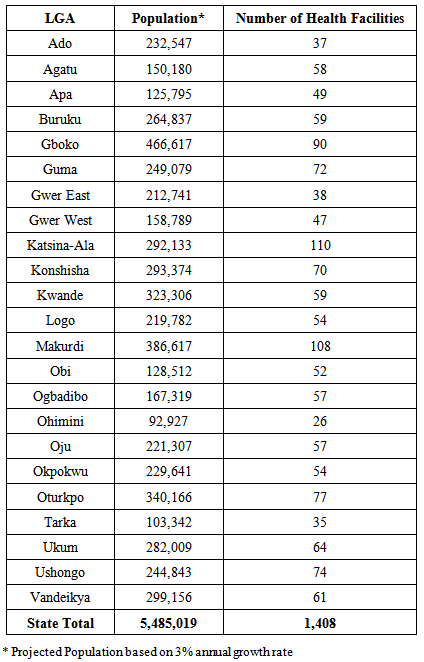
- To investigate this relationship, Pearson Product Moment Correlation Coefficient technique was applied to the data in Table 6 and the result shows that there is a positive relationship between the number of health facilities and population of LGAs. The line of best fit is linear (see Figure 2) while the coefficient of correlation (r) in this case 0.751 is highly significant at 0.05 confidence level. The coefficient of determination (R-square) value of 0.564 indicates that about 56.4% of variance in health facilities is due to population of the LGAs. This is a moderate influence and thus implies that the larger the population of LGAs, the greater the number of healthcare facilities provided. What this result portends is that, the distribution of health care facilities is not entirely based on population. This situation therefore negates the principle of equity and social justice. For instance, Gboko LGA is more populous (466,617) than Makurdi (386,617) and Katsina-Ala (292,133) LGAs, yet Gboko LGA have lesser number (90) of health care facilities when compared with Makurdi (108) and Katsina-Ala (110) LGAs, respectively. Also Kwande and Vandeikya LGAs with larger population have lesser number of health care facilities than Konshisha LGA (see Table 6).
 | Figure 2. Linear relationship of population and number of health care facilities |
|
3.3. Distribution of Health Facilities by Senatorial Districts in Benue State
- Obviously other factors outside population could have influenced the spatial distribution of health care facilities in Benue State. Apart from the political factor which ensures that government projects are distributed on the basis of political patronage in order to appease Political Parties, the private sector may be influenced by the purchasing power of the population as well. The influence of political factor is further revealed as the analysis is made on Senatorial Zonal delineation basis.An analysis of the distribution of health facilities along geo-political Zoning in Benue State (Figure 3) is important. This is relevant to the extent that the State Government employs this classification (Senatorial Zones A, B and C) in the distribution of resources, infrastructure and facilities. The distribution of health facilities along Senatorial districts appear to be near equitable. Perhaps, this is attributable to Government’s policy of ensuring equal distribution of health facilities across the 3 Senatorial Zones in the State. This is shown in table 7 and illustrated in Figure 3.
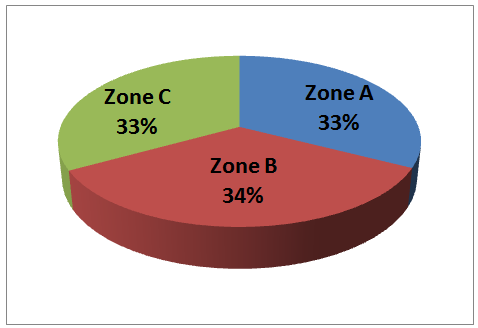 | Figure 3. Distribution of Healthcare facilities per Senatorial District in Benue State |
|
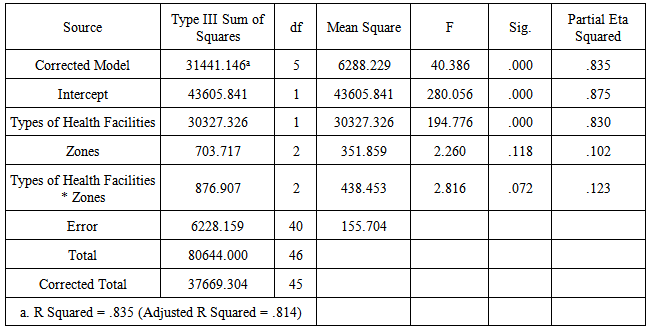
3.4. Variation among Healthcare Levels in Benue State
- In terms of variance between primary and secondary health care facilities, Table 8 shows that there is significant difference between number of primary and secondary health facilities (F= 194.776, P < .05). This difference is expected as there are 117 secondary health facilities as against 1,289 primary health facilities. In terms of Zonal variance, Table 8 shows that no significant difference exist among the Zones (F= 2.260, P > .05). The p-value of 0.118 is above 0.05 and thus implies that the observed differences are mere chance occurrences but not real differences. This is also expected as the relationship is captured by Figure 3. When the types of health facilities interacts with the Zones, no significant effect was also observed (F=2.816, P > .05). The effect size for types of health care facilities (.830) as shown in Table 8 can be classified as large compared with that of the Zones (.102). The non-significant effect of the interaction of types of health facilities and zones can better be visualized in Figure 4.
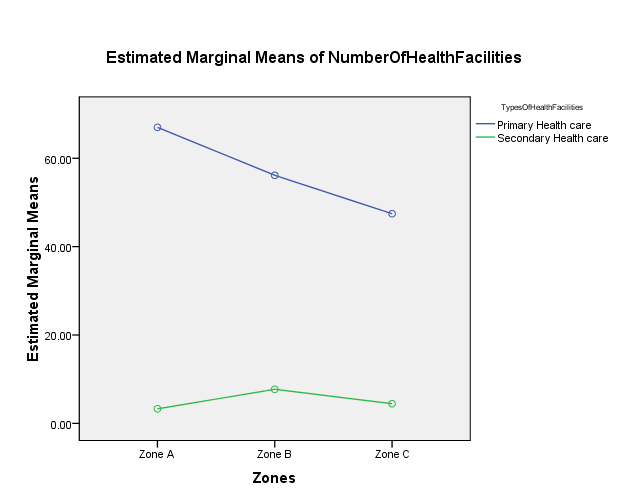 | Figure 4. Interaction between Levels of Health facilities and Senatorial Zones |
|
4. Conclusions and Recommendations
- The distribution of healthcare facilities in the State is not even. The disparity in facility provision is observed among the 23 LGAs. Makurdi the state capital has a general hospital and teaching hospital facilities. The number of primary health centres among the 23 LGAs further demonstrated the persistence of inequalities in healthcare facilities distribution in the state. Thus, the disparity in the distribution of health facilities could generate corresponding disparities in the access of population to healthcare. Of the total number of health care facilities enumerated during the field survey, Government ownership status stood at 888 healthcare facilities (63.07%) while the private sector contributed 520 or 36.93% of the existing health care facilities in the State.From the result of the study, the relationship between population and number of healthcare facilities showed that some LGAs and by extension communities are more vulnerable than others. This implies that some LGAs and communities are in disadvantaged positions while others are advantageous in terms of number of health infrastructure. The consequence is that many individuals and families in the most vulnerable communities cannot attain minimum standards of living due to very poor access to supportive health facilities. Thus, the state presents a discernible imbalance in the relationship between population of LGAs and number of health care facilities.The Millennium Development Goals (MDGs) are the most recent attempts at improving the standards of living. According to [23] and [24], most of the indictors of the MDGs are not likely to be achieved by the target date of 2015 in Nigeria. The result of this study has further supported this assertion. The observed deficiency in the distribution of health facilities in Benue State is counterproductive towards poverty alleviation. There is high level of poverty among the people in various parts of the Benue State. Poverty in this case is seen as a multi-dimensional problem whose definition also emphasizes health dimensions. The problem of poverty becomes very worrisome when viewed from the perspective of basic health facilities. This implies that both inequality and poverty are characteristics of the study area. Because inequality presents a unique form of poverty [25] through mass deprivation, it is emphasized that the provision of healthcare facilities would ensure that growth is consistent with poverty reduction, a topical issue in the provisions of the MDGs. In other words, the poor can be identified as those who are unable to consume a basic quantity of health services, while the rich are those who have adequate access to the basic health services for sustainable living. In the health sector, the 4th NDP noted that rural health care facilities generally are inadequate. It is held that the ratio of population to health infrastructure in most developing countries is far below the WHO standard for health care services coverage in both personnel and space [6]. A moderate correlation coefficient of 56.3% affirms that even in Benue State the relationship between population and number of health care facilities is not very strong. The health sector assessment conducted for USAID/Nigeria in 1991 confirmed the extremely low level of health care provision in Nigeria. The existing inequality of access to health care facilities among the LGAs may generate corresponding disparities in levels of productivity among individuals and communities. This is as a result of the existing correlation between health status of population and productivity. On the basis of the findings from this study, it is recommended that a more robust investigation be carried out in the existing healthcare facilities, especially the primary healthcare facilities, with a view to establishing the levels of health manpower available, bedding and other facilities as well as the actual access levels individuals and communities have to health care facilities in Benue State. Besides, the government should adopt population threshold as a yardstick for health care facility distribution as this is the only approach to ensure equity and social justice in distribution of health care and other basic facilities.
ACKNOWLEDGEMENTS
- The authors are grateful to officials of the Benue State Ministry of Health for providing data on health facilities. Many thanks also to Dr. Jacob Atser for valuable comments and assistance during data analysis.