-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2014; 4(5): 203-209
doi:10.5923/j.phr.20140405.08
Participatory Hygiene and Sanitation Transformation (PHAST) in a Remote and Isolated Community in Samar Province, Philippines
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJoseph U. Almazan
College of Nursing Health Sciences, Samar State University Guindapunan, Catbalogan City, Philippines
Correspondence to: Joseph U. Almazan, College of Nursing Health Sciences, Samar State University Guindapunan, Catbalogan City, Philippines.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Diarrheal disease is one of the leading causes of death in children under five years old, most people who die from this disease actually die from severe dehydration and fluid loss. Moreover, 88% of its global diarrheal disease is attributed to unsafe water supply, inadequate sanitation, and hygiene. This investigation was developed to determine the effect of Participatory hygiene and sanitation transformation (PHAST) program in an isolated community of Mabini, Samar Province, Philippines. Longitudinal research design was used in order to determine the effect of the program one year was implemented in the community. A purposive sampling was utilized in this investigation which accounts a total of 39 households in Mabini community, Basey, Samar, without toilet facilities. The instrument used was the modified questionnaire of the Philippine Red Cross in water and sanitation before and after the program was implemented. Results showed that there was improvement of knowledge on water and sanitation, handwashing practice, household waste practices drinking practices, defecation practices. Thus, program reaching the most isolated and difficult areas experiencing the most detrimental effects which improve poor hygiene and sanitation, improving health, equality and social justice.
Keywords: Participatory hygiene, Sanitation transformation, Remote and isolated community
Cite this paper: Joseph U. Almazan, Participatory Hygiene and Sanitation Transformation (PHAST) in a Remote and Isolated Community in Samar Province, Philippines, Public Health Research, Vol. 4 No. 5, 2014, pp. 203-209. doi: 10.5923/j.phr.20140405.08.
1. Introduction
- Diarrheal disease is one of the leading causes of death in children under five years old, most people who die from this disease actually die from severe dehydration and fluid loss according to [1]. It is also an indication of an infection in the intestinal cavity, which primarily caused by a bacterial organisms and virus. This infection is spread through contaminated drinking-water and food, or from person-to-person as a result of poor hygiene.Moreover, 2.6 Billion People in the world (almost 40% of global population) had a lack access to basic sanitation, 88% of its global diarrheal disease is attributed to unsafe water supply, inadequate sanitation, and hygiene. 5,000 children under 5 die each day due to diarrheal diseases routed in inadequate water & sanitation – deaths which are preventable [2].Consequently, an anticipated 2.5 billion people in the world have lacked access to improved sanitation which is related to diarrheal diseases [3]. Approximately 801,000 children lower than 5 years of age have diarrhea every year highest of these were from in developing countries [4]. It also mentioned constituting 7.6 million deaths of children under the age of five and also means that about 2,200 children were dead every day because of the diarrheal diseases. In addition, diarrheal disease related to inadequate water supply and sanitation is among the leading causes of death among people in the developing world, and stemming the tide means that should look critically at what and does not work in decreasing morbidity and mortality [5].In developing countries, children under three years old experience on average three episodes of diarrhea every year. In the Philippines like the other developing countries, about 20 million Filipinos who do not have an access to improved water supply and environmental sanitation [6].In addition to this, since many Filipinos who do not have an access to improved water supply and environmental sanitation, almost 8 million of these areas defecates in the open. The poorest 20 percent of its rural population went from 36 percent open defecation to a staggering 48 percent open defecation. Open defecation related to poor sanitation and poverty go hand in hand, and the rural poor are four times practice more open defecation than in urban parts [7].However, when the super typhoon Haiyan hit the Philippines, thousands were killed and injured, survivors were warned about the diarrheal diseases such as cholera because of the lack of sanitation. Contaminated water remains a problem of the country because of the bodies along with dead livestock were floating in the water supplies [8]. Similarly, the problem has hampered the implementation of much needed investment in the sector. Meanwhile, Participatory hygiene and sanitation transformation (PHAST), an innovative approach designed to promote hygiene behaviors, sanitation improvements using specifically developed participatory techniques. Hygiene promotion and water treatment in the home are among the most effective interventions. This program depends on the expertise of health education facilitators for community education and motivation according [9].The PHAST program approach helps people to become self-reliant about themselves and their capability to take action and make growth in their communities. Spirits of enablement environment and personal growth are as important as the physical changes, such as cleaning the environment or building toilet facilities [10]. Meanwhile, despite of several hygiene promotion programs to prevent diarrhea, there still pockets of the population that need to be addressed in terms of hygiene and sanitation.Furthermore, International Committee of the Red Cross ICRC mentioned that one of the community in Samar province cited as one of the places vulnerable population areas that needs to be addressed for improvement of knowledge among the affected families in the community of Mabini, Basey, Samar [11]. Moreover, it is also one of the communities that are high number without toilet facilities. Thus the researcher was motivated to conduct the study. Hence, this will valuable to the families, communities, in decreasing the burden of diarrheal diseases in the community. Furthermore, to the local government units this would serve as the basis for the development and prioritizing health programs.This investigation developed to evaluate the effect of program in an isolated community of Samar Province, Philippines.
2. Methods
- This study utilized a longitudinal research design in order to determine the effect of Participatory hygiene and sanitation transformation (PHAST) program to the community. This study was appropriate in order the evaluate of its effect of the program to the community. The baseline assessment was conducted on June 2012; meanwhile the endline assessment was conducted on August 2013 which after the program was implemented.A non-probability-purposive sampling was utilized in this investigation. A total of 39 households in Mabini community, Basey, Samar, without toilet facilities were recruited to participate in the program specifically utilizing total purposive sampling.The instrument of this research was the modified questionnaire of the Philippine Red Cross in water and sanitation. There were two sets of questionnaires. Set I was the demographic profile of the respondents. Set II was determined Knowledge on Water and Sanitation, Handwashing Practices, Drinking Practices, Household Waste Practices, Defecation Practices.In presenting the profile of the respondents, frequency counts, percentage, whichever will be used. The data were analyzed using SPSS, version 19. T –value determines the ratio of an estimated parameter from its notional value and its standard error. Moreover, Paired t-test determines whether before the program and after the program was implemented differs from each other in a significant way.The investigators send an approval letter to the Ethics Committee on Local Government of Basey, Samar before conducting the investigation and was approved. The Confidentiality of information and anonymity of the respondents was maintained by using only code number of the questionnaire instead the name of the respondents.
3. Results
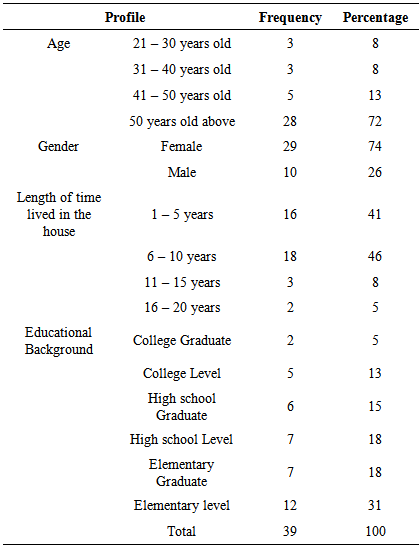
- Table 1 provides information on the demographic profile of the respondents. Most of the respondents were female (29 or 74%) among the 39 respondents. As to age, almost three fourth of the respondents (28 or 72%) have the age range of 50 years old – above. As to the Length of time lived in the house, almost half (18 or 46%) of the respondents live from 6-10 years while only 2 or 5% of the respondents lived from 16-20 years old. Finally, as to their Educational Background, it found out that 12 or 31% respondents were Elementary level while only 2 or 5% were college graduate.
|
|
|
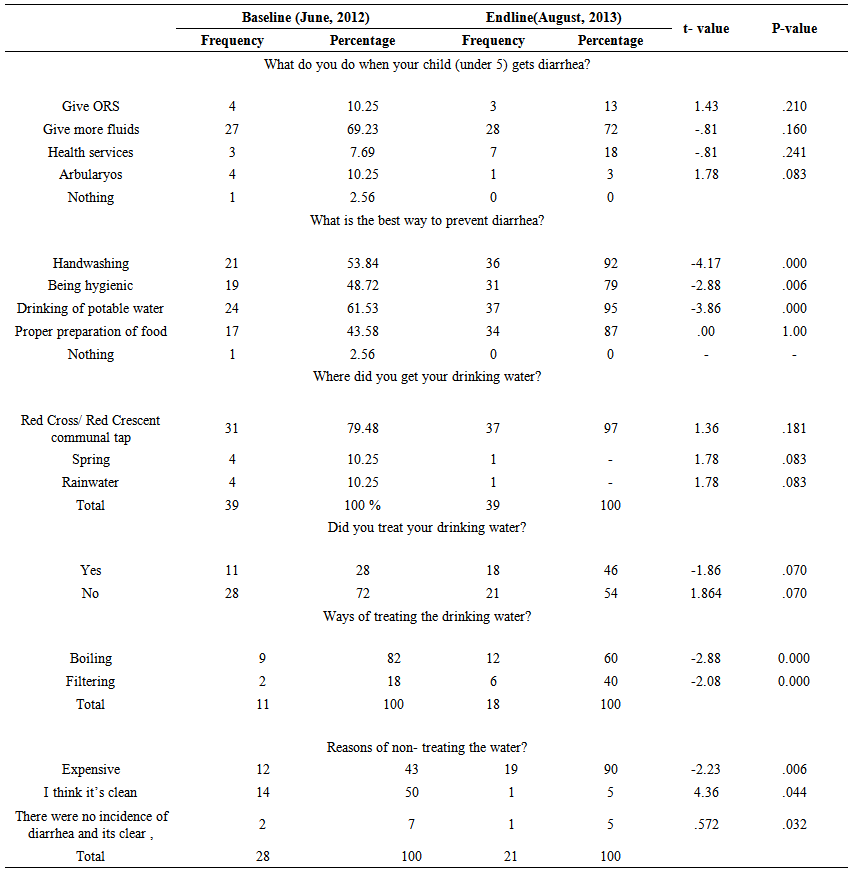 | Table 4. Drinking Practices |
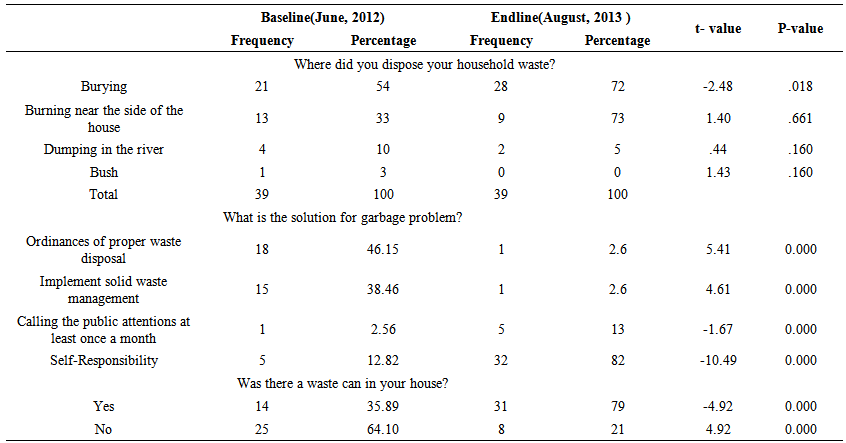 | Table 5. Household Waste Practices |
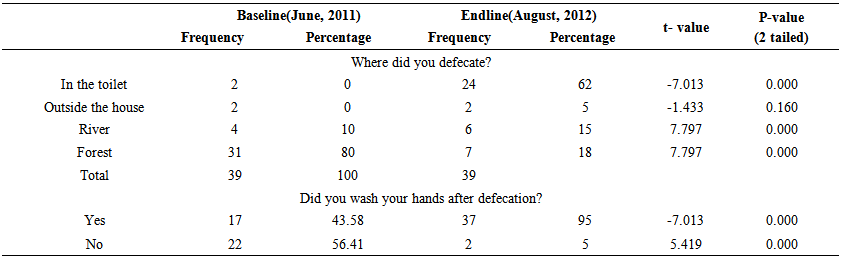 | Table 6. Defecation Practices |
3. Discussion
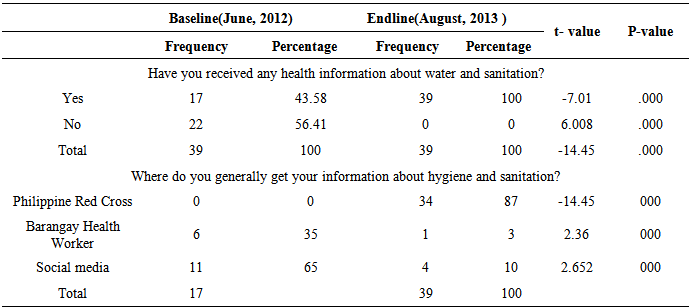
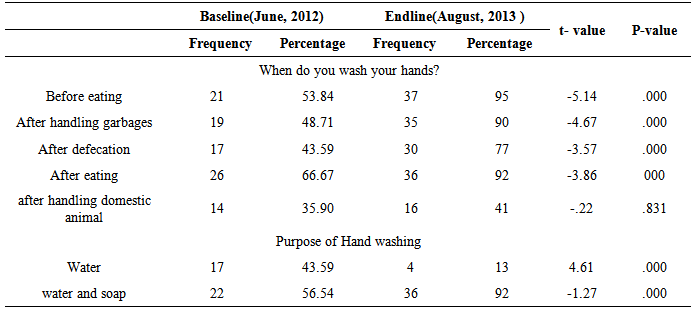
- The results of this study showed improvement in terms of the respondent’s knowledge on water and sanitation. This result was same to the previous results from Uzbekistan [12], Zimbabwe [13, 14] and Vietnam [15] in terms of improvement in knowledge. Moreover, this finding validates the study [16] which revealed the need for handwashing to eliminate unsafe domestic water handling during handwashing and reduce the spread of communicable diseases.Findings also indicated that there were improvement of their drinking practices after the said program was implemented. This affirms to the previous study that improvement of drinking practice has been an important strategy in the effort to reduce diarrheal morbidity [17].This also consistent with the study of [18] diarrheal outbreaks is a sign of insufficient efforts in controlling the garbage problem and monitoring the risk of disease outbreaks. Effective sanitation and hygiene programmes in require a better understanding of the relationship between practices and physical landscape.There also improved hygiene practices, finding further affirms the study [19] who concluded that personal hygiene practices cannot be attained without water supply, which the ICRC constructed 2nd level water facilities in the area.Then, it likewise supports the study of [20] that improvement of people water and sanitation knowledge was factors which can motivate people to adopt safe hygienic practices. Next, the result of the program agrees that community participations promote hygienic defecation and stool clearance practices in order to decrease diarrheal diseases. Furthermore, promoting of safe hygiene is one of the most cost-effective means of preventing communicable diseases.Furthermore, there is progress in sanitation among the community. This corroborates the study of [21] that sanitation has a substantial impact on peoples’ survival. Personal and domestic hygiene was important in reducing the rates of ascariasis, diarrhea, schistosomiasis, and trachoma. Sanitation facilities decreased diarrhea morbidity and mortality and the severity of hookworm infection. However, finding on the baseline assessment proves the study [22] isolate and difficult community was contending with an inadequate public health infrastructure, lack of education programmes, and economic limitations in obtaining hygiene products. Therefore, it carries a greater burden of morbidity and mortality from infectious illnesses.Finally, results also showed improvement of household waste practices after the implementation of the program. This is worth noting, since the previous study discussed in sanitation education decreases the children diarrhea in developing countries, particularly the intervention simple way to promote lower rates of childhood diarrhea [23].
4. Conclusions
- Based on the result findings, the following conclusion drawn and the recommendations that were formulated based on the results of the study.In the context of the study, educational attainment is not a prerequisite in to make effective decision making on hygiene and sanitation. It also creates synergy process on the people perception. Moreover, improvement of knowledge hygiene and sanitation and practices into communities has been shown in preventing diarrheal diseases. This makes a good idea of the health implications on poor hygiene and sanitation. Moreover, they have adequate knowledge about safe hygienic practices. However, it seems that some knowledge was not properly utilized as numerous field visits confirmed that taking a bath in the river of some households even after the program was implemented. In terms of the questionnaire’s results, practices were also found to be higher among households who attended the program indicated that there is improved knowledge and practices. Consequently, enlightening the access to safe water supply and improve sanitation measures, as well as promoting good hygiene, are key mechanisms for the prevention of diarrhea.Therefore, Participatory Hygiene and Sanitation Program reaching the most vulnerable people experiencing the most detrimental effects of poor sanitation and hygiene. Thus, investment in the program, especially for isolated and very remote communities, has the possible to bring about lasting change.
ACKNOWLEDGEMENTS
- Gratitude to Philippine Red Cross, Samar State University that supported the research.
References
| [1] | World health Organization. Water and Sanitation. Retrieved from http://www.who.int/mediacentre/factsheets/fs330/en/, Accessed on April 2013. |
| [2] | World health Organization. Diarrheal Diseases. Retrieved from http://www.who.int/mediacentre/factsheets/fs330/en/, Accessed on August 2009. |
| [3] | United Nations Children Fund. Lack of Sanitation Clean Water. Retrieved from lack of sanitation clean water killing kids says unicef (accessed on 25,March 2013. |
| [4] | Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, Cibulskis R, Li M, Mathers C, Black RE. “Global, Regional, and National Causes of Child Mortality: An Updated Systematic Analysis”. Lancet Nouran. http://www.ncbi.nlm.nih.gov/pubmed/22579125,2012 |
| [5] | Fewtrell, Lorna and Colford, John M. Water, Sanitation and Hygiene: Interventions and Diarrhoea. Health, Nutrition, and Population. Fewtrell&ColfordJuly2004.pdf, 2004. |
| [6] | World Bank. Water and Sanitation Program - East Asia and the Pacific (WSP-EAP). EconomicImpactsofSanitationinthePhils_Summary.pdf, 2008. |
| [7] | United Nations Children Fund. Lack of Sanitation Clean Water. Retrieved from lack of sanitation clean water killing kids says unicef (accessed on 25, March 2013). |
| [8] | World Bank .Water and Sanitation Program - East Asia and the Pacific (WSP-EAP). EconomicImpactsofSanitationinthePhils_Summary.pdf 2008. |
| [9] | Freeman MC., Clasen, T, Brooker, SJ., Akoko, DO, Rheingans, Richard. “The Impact of a School-Based Hygiene, Water Quality and Sanitation Intervention on Soil-Transmitted Helminth Reinfection: A Cluster-Randomized Trial”. Health, Nutrition, and Population Family Journal, http://www.ajtmh.org/content/89/5/875.abstract,2004. |
| [10] | World Bank .Water and Sanitation Program - East Asia and the Pacific (WSP-EAP). EconomicImpactsofSanitationinthePhils_Summary.pdf(accessed on 2008). |
| [11] | International Committee of the Red Cross ICRC. http://www.icrc.org/eng/,2011. |
| [12] | Waterkeyn, J. Cairncross S. Creating demand for sanitation and hygiene through Community Health Clubs: A cost-effective intervention in two districts in Zimbabwe. Social Science & Medicine November 2005, Pages 1958–1970. |
| [13] | http://www.sciencedirect.com/science/article/pii/S0277953605001759. |
| [14] | Freeman MC., Clasen, T ,Brooker, SJ., Akoko, DO, Rheingans, Richard. “The Impact of a School-Based Hygiene, Water Quality and Sanitation Intervention on Soil- Transmitted Helminth Reinfection: A Cluster- Randomized Trial”. Health, Nutrition, and Population Family Journal, http://www.ajtmh.org/content/89/5/875.abstract,2004. |
| [15] | Herbst, S.; Benedikter, S.; Koester, U.; Phan, N.; Berger, C.; Rechenburg, A.; Kistemann, T.(2009). “Perceptions Of Water, Sanitation And Health: A Case Study From The Mekong Delta, Vietnam”.Water Science & Technology, Research on South-East Asia Journal. May 19,2008.2009, Vol. 60 Issue 3, p699-707. |
| [16] | Jenkinsa, M, Anandb, Revellc G, Sobseyb M,. ‘‘Opportunities To Improve Domestic Hygiene Practices Through New Enabling Products: A Study Of Handwashing Practices And Equipment In Rural CambodiaInt”. International Health Journal August 2, 2013, doi: 10.1093/inthealth/iht026. |
| [17] | Jenkinsa, M, Anandb, Revellc G, Sobseyb M,. ‘‘Opportunities To Improve Domestic Hygiene Practices Through New Enabling Products: A Study Of Handwashing Practices And Equipment In Rural CambodiaInt”. International Health Journal August 2, 2013, doi: 10.1093/inthealth/iht026. |
| [18] | Fewtrell, Lorna and Colford, John M. Water, Sanitation and Hygiene: Interventions and Diarrhoea. Health, Nutrition, and Population. Fewtrell&ColfordJuly2004.pdf,2004. |
| [19] | Hoque BA, Mahalanabis D, Alam MJ, (1999). “Post-Defecation Handwashing In Bangladesh: Practiceand Efficiency Perspectives”. Public Health. Journal 1995 Jan; 109(1):15-24 |
| [20] | Kumar, GS, Kar SS, Animesh J. “Health and environmental sanitation in India: Issues for prioritizing control strategies”. Indian J Occup Environ Med. 2011 Sep-Dec; 15(3): 93–96. |
| [21] | Mafuya, NP, Nimish S. (2003). “Factors that could motivate people to adopt safe hygienic practices in the Eastern Cape Province, South Africa”. Int Health. 2013 Dec;5(4):295-301. |
| [22] | Yeager, B, Huttly S, Bartolini, R, Rojas M, Lanata C. “Defecation Practices of Young Children In A Peruvian Shanty Town” Soc Sci Med. 1999 Aug;49(4):531-41. |
| [23] | Aiello, AE Larson, EL. “What is the Evidence for a Causal link Between Hygiene and Infections?”Lancet Infect Dis. 2002 Feb;2(2):103-10. |
| [24] | Stanton BF, Clemens J (1987). An Educational Intervention for Altering Water-Sanitation Behaviors to Reduce Childhood Diarrhea in Urban Bangladesh. Am J Epidemiol. 1987 Feb;125(2):292-301. |