-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2014; 4(1): 25-30
doi:10.5923/j.phr.20140401.05
Validity and Reliability of the Interaction Rating Scale Advanced (IRSA) as an Index of Social Competence Development
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTokie Anme1, Kentaro Tokutake1, Emiko Tanaka1, 2, Taejko Watanabe3, Etsuko Tomisaki1, Yukiko Mochizuki1, Bailiang Wu1, Ryoji Shinohara4, Yuka Sugisawa5, Shuntaro Okazaki6, Norihiro Sadato6
1Faculty of Medicine, University of Tsukuba, Ibaraki, Japan
2Research Fellow, Japan Society for the Promotion of Science, Tokyo, Japan
3Ashikaga University, Tochigi Japan
4University of Yamanashi, Yamanashi Japan
5Ushiku Health Centre, Ibaraki, Japan
6National Institute for Physiological Sciences, Aichi, Japan
Correspondence to: Tokie Anme, Faculty of Medicine, University of Tsukuba, Ibaraki, Japan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The purpose of the current study was to clarify the validity and reliability of the Interaction Rating Scale Advanced (IRSA) as a context-based practical index of social competence development. Participants were 50 adults who completed a five-minute interaction session, during which they were observed and assessed using the IRSA. Furthermore, health social professionals evaluated participants’ social competence using practical assessment.Results indicated a moderately high correlation (r = 0.58) between IRSA scores and professionals’ practical evaluation. The Cronbach’s alpha value was 0.89. Thus, the IRSA appears to measure social competence with high validity and reliability. Since the IRSA provides context-based evidence of social competence development, this measure should be useful for evaluating the various features of social interaction in a practical setting.
Keywords: Social Competence, Interaction, Evaluation, Scale, Adult
Cite this paper: Tokie Anme, Kentaro Tokutake, Emiko Tanaka, Taejko Watanabe, Etsuko Tomisaki, Yukiko Mochizuki, Bailiang Wu, Ryoji Shinohara, Yuka Sugisawa, Shuntaro Okazaki, Norihiro Sadato, Validity and Reliability of the Interaction Rating Scale Advanced (IRSA) as an Index of Social Competence Development, Public Health Research, Vol. 4 No. 1, 2014, pp. 25-30. doi: 10.5923/j.phr.20140401.05.
Article Outline
1. Introduction
- Social competence has been defined as a dimension of social intelligence[1, 2]. Social intelligence is the ability to engage in adaptive and positive social interactions, which is theoretically distinct from general academic intelligence. However, it is often difficult to discriminate social intelligence from general intelligence. Historically, social intelligence has somewhat overlapped with social competence, which is determined by the complex interaction between the individual, his/her home and school environments, peer relationships, and the larger sociocultural environment[3]. Social competence is broadly defined as the ability to understand others in the context of a social interaction and engage in smooth communication. Thus, social competence should be evaluated by the interaction between the individual and his/her social environment[4].Dealing with social stress among adults who display impulsive and maladjusted behavior requires society to prepare appropriate support systems and environments for those individuals. Researchers have been engaged in the study of social competence development for decades. However, methodologies that consider individuals in conjunction with their social environment across developmental stages are not yet well developed.We developed four social competence scales for different stages of lifespan development: (1) the Interaction Rating Scale (IRS), which is an observation method for child– caregiver interactions that assesses children under 8 years old[5,6]; (2) the Interaction Rating Scale between Children (IRSC), which is an observation method for child–child interactions that assesses children 3 to 18 years old[7]; (3) the Interaction Rating Scale Advanced (IRSA), which is an observation method for adult–adult interactions that assess individuals over 15 years old[8]; and (4) the Social Skill Scale (SSS), which uses an enumerator method to assess children under 7 years old[9]. These scales, based on accumulated knowledge from the developmental sciences, have focused on measuring the quality of an environment where positive interactions with the environment are significantly related to healthy development. Two instruments assessing the home environment, namely the Home Observation for Measurement of the Environment (HOME)[10] and the Index of Child Care Environment (ICCE)[11] are often used in research related to context-based child social competence development.The HOME and ICCE evaluate the environment within natural settings, including one’s emotional and verbal responsiveness to another individual as well as one’s acceptance of another’s behavior. The HOME suggests that context-based social competence is essential for lifespan development because it reflects one’s adaptability and convergence in the real world. The HOME is a very popular measure, having been used in more than 100 countries. Several observation-based social competence measures have been developed that focus on specific areas of social interactions; these measures include the Mediated Learning Experience Rating Scale (MLERS), which deals with teacher–student interactions[12]; the Social Skills Rating System (SSRS), which is used to examine caregiver–child interactions[13]; and the Autism Diagnostic Observation Schedule-Generic (ADOS-G)[14] and Childhood Autism Rating-Scale (CARS), which are used to assess social competence individuals suspected of having an autism spectrum disorder[15].Conversely, questionnaire-based social competence measures have focused on more generalized settings and address multidirectional factors, as is the case with the Social Skills Inventory (SSI)[16] (containing six factors: “emotional expressivity,” “emotional sensitivity,” “emotional control,” “social expressivity,” “social sensitivity,” and “social control”), the ENDCOREs[17] (six factors: “self-control,” “expressivity,” “sensitivity,” “assertiveness,” “responsiveness,” and “regulation”), the Adult Behavior Checklist for Ages 18-59 (ASEBA)[18,19] (six factors: “adaptive functioning,” “empirically based syndromes,” “substance use,” “internalizing,” “externalizing,” and “total problems”), and the Weinberger Adjustment Inventory (WAI)[20] (six factors: “distress,” “anxiety,” “depression,” “low self-esteem,” “low well-being,” “self-restraint,” “suppression of aggression,” “impulse control,” “responsibility,” and “consideration of others”). According to the above-mentioned measures, the current study used the most common factors for assessing social competence developing: “empathy/coordination,” “self-regulation,” and “assertion.” Our factors are referred to as “sensitivity/responsiveness,” “self-control/regulation,” and “assertiveness/expressivity.”The purpose of the current study was to clarify the validity and reliability of the IRSA as a context-based practical index of social competence.
2. Methods
2.1. Participants
- Participants were 50 adults, 25 males and 25 females, aged 18 to 48 years old. In order to comply with ethical standards before conducting the research, all participants signed informed consent forms and were made aware that they had the right to withdraw from the study at any time. To maintain confidentiality, a personal ID system was used to protect personal information. Furthermore, all video picture data were stored on a disk, which was password protected. Only the researchers with necessary permission were given access to this data. The ethics committee of the National Institute for Physiological Sciences approved this study.
2.2. Measures
- The IRSA is a 92-item instrument designed as a brief but comprehensive observation measure that assesses basic social competence for individuals over the age of 15. Social competence is examined through five-minute observations of a social interaction. One advantage of the IRSA is that evaluations of interactions can be completed in a short period within normal, daily situations.The IRSA includes a behavioral score and 6 subscales scores that combined provide an impression score: “self-control,” “expressivity,” “sensitivity,” “assertiveness,” “responsiveness,” and “regulation” (Appendix 1). The 92 items were extracted from several sources, including original items from the study authors and items from the IRS[5], SSRS[13], and the ENDCOREs[17].Two different variables are scored: behavior and impression. For the behavior variable, items are assessed in terms of the presence of a behavior (0 = no, 1 = yes), and the sum of all items in provides the overall score. The total score can range from 0 to 92. As for the impression, each observed behavior is rated on a five-point scale where 1 is “not evident at all,” 2 is “not clearly evident,” 3 is “neutral,” 4 is “evident,” and 5 is “highly evident.” The rating procedure is as follows: the evaluator completes the checklist, focusing on the participant’s behaviors (e.g., expressing his/her own feelings to the partner). The health-social professionals provides separately an impression score for each observed behavior. The inter-observer reliability was 90%.
2.3. Procedure
- The IRSA was evaluated during a five-minute video recording of an interaction (two participants play a game called, “Keep it steady!” which consists of a wooden ring and 6 inch long 27 sticks with varying widths. Players grab all the sticks together, slide the wooden ring around the center of the bundle, give it a twist, and stand the sticks up on end. The game begins by pulling out a piece and taking turns until the structure collapses). The recording was carried out in a room with four video cameras, which assessed the interaction from four angles (Figure 1). The participant dyads were escorted into a room furnished with a small table and two chairs. The instructor introduced the game to both participants.
 | Figure 1. Video recording from four directions |
3. Results
- The correlation analysis was used to validate the use of this measure to assess social competence (i.e., how well the IRSA assesses behaviors in conjunction with professional reports).Figure 2 shows the correlation between the total score on the IRSA and professionals’ practical evaluations of the interactions. Results suggest a moderately high correlation (r = 0.58, p < 0.001) between IRSA scores and professionals’ practical evaluations. No significant gender or age differences were found on the IRSA subscales. The internal consistency of the IRSA, as measured by Cronbach’s alpha, was 0.89.
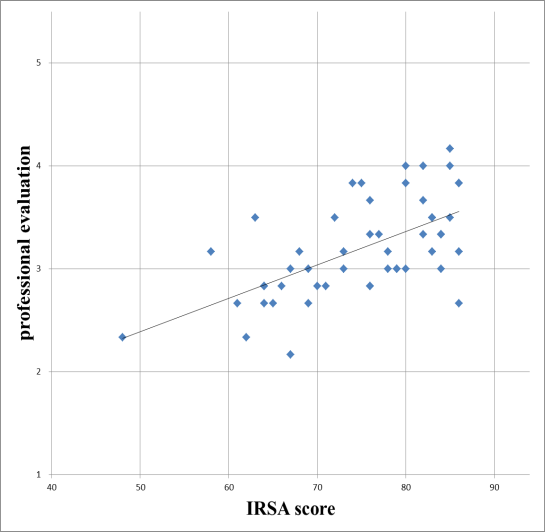 | Figure 2. Correlation between IRSA scores and professional evaluations |
4. Discussion
- This current study provides a measure (IRSA) that can assess social competence with moderately high validity and reliability. The social competence scale for child–caregiver interactions (IRS)[5,6] and child–child interactions scale (IRSC)[7] have already shown adequate reliability, validity, feasibility, and practical utility for examining social interactions over time. It is meaningful that the IRSA can be used to assess social competence continuously along a lifespan developmental continuum.Several studies have indicated that observational outcomes differ from self-administrated outcomes because self-optimism produces biases that provide favorable evaluations for the self[21,22]. Observation-based scale is essential to understand the social competence development actually used in one’s life.Social skills play a role in how well an individual copes with stress. Thus, possessing adaptive social skills should be just as important to social adjustment and well-being as is psychological health[23]. The IRSA may prove useful in research on psychological stress and coping by having the ability to examine individuals' abilities to cope with stress [24]. Additionally, the IRSA could be used as part of communication skills training programs for health care professionals[25].The strength of the IRSA is the ability to assess objective social competence throughout the lifespan. Additionally, the IRSA is easy to use in practice because it is highly adaptable to various age groups.Furthermore, the framework of the IRSA is based on the most common measurement paradigms used around the world; this makes it easier to use this measure within international comparative studies. Additionally, the 6 subscales are based on several categories that are widely used in research on social competence indicators. Even though the IRSA has some valuable strengths, it is also important to acknowledge the IRSA’s limitations. First, the IRSA was assessed with only 50 participants in the current study. Thus, the generalizability of the present results should be taken with caution. Second, the IRSA subscales might not cover all the dimensions of social competence, even though we used the most common components of social competence addressed in previous studies.Despite these limitations, the IRSA appears to be a consistent, valid screening instrument that reflects attributes of social interactions. We have already started to employ the IRSA for assessing individuals with autism in order to characterize behavioral features and the evaluation of treatment outcomes. Further research should enhance the potential to reveal additional features of social interaction development that will be of use to both practitioners and researchers.
5. Conclusions
- This study indicated a moderately high correlation (r = 0.58) between IRSA scores and professionals’ practical evaluation. The Cronbach’s alpha value was 0.89. Thus, the IRSA appears to measure social competence with high validity and reliability. Since the IRSA provides context-based evidence of social competence development, it should be useful for evaluating the various features of social interaction in a practical setting, continuously along a lifespan developmental continuum.
ACKNOWLEDGEMENTS
- This research was supported by a Grant-in-Aid for Scientific Research to N.S. (S21220005) from the Japan Society for the Promotion of Science. Part of this study is the result of a project called the "Development of biomarker candidates for social behavior," carried out under the Strategic Research Program for Brain Sciences by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) and a Grant-in-Aid for Scientific Research (23330174, 24653134).
Appendix 1. All items on the Interaction Rating Scale Advanced
- 1. Expressivity: Expresses his/her thoughts and feelings precisely1) Vocalizes.2) Expresses his/her own feelings to the partner.3) Attempts to elicit help or consolation from the partner.4) Shows self-assertiveness to the partner through a gesture.5) Casts the partner a glance to seek sympathy.6) Shows the change of his/her feelings through facial expressions7) Smiles or laughs.8) Attempts to make eye contact with the partner9) Attempts to elicit a response from the partner.10) Looks at the partner's face to get information/clarification.11) Shows his/her feelings by words and actions together.2. Assertiveness: States his/her opinion or position clearly to others.12) Speaks up to the partner about what he/she thinks.13) There are words and actions that indicate his/her decision.14) Talks to, suggests, or lets the partner accomplish something while he/she pays attention.15) Expresses his/her opinion to the partner.16) Verbalizes a differing opinion or position.17) Exhibits a differing opinion by his/her expression and gestures.18) Uses both verbal descriptions and non-verbal instruction.19) Provides guidance through explanation but not through order.20) Explains his/her opinion according to the level of competence/ability of the partner.21) Instructions and opinions are clear and unambiguous.22) Explains his/her opinion logically.23) Expresses his/her own idea after showing that he/she understands the partner's idea.24) Expresses his/her ideas after indicating his/her understanding to the partner through expression and gesture.25) Makes a decision after indicating that he/she understood the partner's idea/suggestion.26) Makes a decision after showing through non-verbal expression that he/she understood the partner.3. Sensitivity: Ability to read the partner's feelings and thoughts accurately.27) Shows an appropriate reaction through a change in his/her expression and gestures.28) Vocalizes or speaks in response to the partner's verbalization.29) Vocalizes or adjusts own behavior in response to the partner's verbalization.30) Looks at the partner or materials when he/she shows non-verbal behavior.31) Vocalizes in response to the partner's behavior or nonverbal cues.32) Vocalization, makes a facial expression, or moves in response to the partner's behavior or nonverbal cues.33) Vocalizes after noticing changes in his/her partner’s facial expression.34) Looks at his/her partner or materials after noticing the changes in the partner’s facial expression.35) Vocalizes, expresses, or moves according to changes in partner's expression.36) Smiles or frowns within five seconds after the partner's vocalization.37) Looks at the partner's face or eyes when the partner attempts eye contact.38) Behaves appropriately in response to the partner's gestures or changes in expression.4. Acceptance: Understands and respects the partner's opinion or position39) Smiles in response to the partner's smile.40) Praises the partner's efforts, success, and behavior.41) Smiles, claps hands, or shows he/she is glad when the partner is feeling happy.42) Shows empathy by verbal or non-verbal responses when the partner is in a bad mood.43) Emits positive, sympathetic, or soothing verbalizations in response to the partner's feelings.44) Responds to the partner's vocalizations with an affectionate verbal response.45) Smiles at the partner's verbalization.46) Nods in response to partner's verbalizations and/or actions47) Emits a soothing non-verbal response (e.g., pat, touch, rock) at the partner's successes or failures.48) Smiles and/or nods at the partner during the episode.49) Does not vocalize or interrupt the partner while he/she is speaking.50) Nods at the partner's comment.51) Accepts the partner's opinion partially or totally by saying, "let's do it,” or by acting in a manner consistent with the partner's suggestion.52) Accepts the partner's opinion even when his/her own opinion differs.53) Pauses when the partner starts to verbalize.54) Disturbs the partner.55) Allows the partner to decide what he/she wants to do.56) Praises the partner's skills during the assignment.5. Regulation of the interpersonal relationship: Works with the partner to develop a good relationship.57) Provides an environment free of distractions for the partner.58) Does not make negative comments to the partner.59) Does not behave negatively toward the partner.60) Affirms the partner with nods or other gestures.61) Laughs while they are looking at each other.62) Laughs while they are looking at the same thing.63) Moves in the same manner as the partner moves.64) Does not turn away from the assignment and pays close attention to the partner.65) Verbally praises the partner during the assignment.66) Praises the partner with applause.67) Talks to the partner positively or encouragingly during the assignment.68) Says "Thank you" to the partner when he/she grants a concession.69) Does not criticize the partner when they have differing opinions.70) Tries to talk with the partner logically when they have differing opinions.71) Tries to avoid emotional conflicts with the partner.72) Tries to respond calmly when the partner becomes angry or agitated.6. Self-control: Ability to control personal emotions and behaviors.73) Waits for the partner's reaction or action for at least five seconds.74) Emits appropriate movement of eyes.75) Emits appropriate phonation.76) Emits appropriate utterances.77) Emits appropriate movements.78) Makes clearly recognizable hand motions towards materials during the assignment.79) Concentrates on the task and is gentle with the materials.80) Does not interrupt the partner's activity81) Is not destructive/rough with the materials.82) Not tense.83) Does not shout or raise his/her voice.84) Does not display distress cues even when the task does not go well.85) Is not rude to the partner.86) Avoids displeasing the partner.87) Does not speak negatively of others.88) Does not curse at people or at things.89) Follows the rules of the game.90) Touches a task together.91) Emits appropriate emotional expression.92) Praises the partner when he/she succeeds or when the partner fails, he/she commiserates.