-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2013; 3(5): 136-141
doi:10.5923/j.phr.20130305.05
Estimating the Annual Incidence of Violence Related Injuries in Kenya: A Derivation from Review of Hospital Reports in 2007
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWilliam K. Maina1, Nzoya Munguti1, Wilfred G. Mwai1, Alexander Butchart2, Luk Cannoodt2
1Ministry of Health, Nairobi, Kenya
2World Health Organization, Geneva, Switzerland
Correspondence to: William K. Maina, Ministry of Health, Nairobi, Kenya.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Violence related injuries contribute to a significant burden of diseases and affect the social and economic wellbeing of individuals, families and communities in Kenya. Despite this, the true magnitude of injury from interpersonal, self-directed and collective violence remains largely unknown and receives very little attention. This paper presents the situation of injuries due to violence in Kenya and attempts to estimate the magnitude of diseases related to violence as reported in the health care systems annually. Data for this study was collected from various sources. All recorded injuries reported in randomly selected hospitals in 2007 were collected using a data collection tool adopted from the WHO and CDC Manual for the estimation of the economic cost of violence. To establish the distribution and characteristics of the cases, prospective data was collected at Kenyatta National Hospital and Machakos District Hospital where 200 cases were studied between June and September 2008. Further data was derived from the health records and information systems reports. It was estimated that there were 218,592 injuries due to violence that received hospital treatment and/or resulted in deaths in Kenya during 2007. Of these, 10,007 (4.6%) were fatal; 45,889 (21%) were severe and required hospital admission, and 162,696 (74.4%) were slight, requiring emergency department treatment only. 63% of injuries involved men while 37% involve women. By systematically estimating the incidence of violence related injuries in Kenya, this paper aims at highlighting the magnitude of this problem and advocates for urgent action to address it.
Keywords: Violence, Incidence Estimation, Injuries, Kenya
Cite this paper: William K. Maina, Nzoya Munguti, Wilfred G. Mwai, Alexander Butchart, Luk Cannoodt, Estimating the Annual Incidence of Violence Related Injuries in Kenya: A Derivation from Review of Hospital Reports in 2007, Public Health Research, Vol. 3 No. 5, 2013, pp. 136-141. doi: 10.5923/j.phr.20130305.05.
Article Outline
1. Introduction
- Globally, violence accounts for over 1.6 million deaths per year and at least 16 million cases of injury which are severe enough to receive medical treatment in hospitals, and untold suffering for tens of millions of individuals. This translates to over 4,000 deaths daily with 90% of these coming from low and middle income countries. This is roughly the same as the daily toll of deaths due to tuberculosis, and more than the daily toll of some 3,500 deaths due to malaria[1].The World Health Organization (WHO) defines violence as ‘the intentional use of physical force or power, threatened or actual , against oneself, another person, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation’[2]. The World Report on Violence and Health 2002 presents the contexts in which violence occurs by dividing it into three sub-types according to the victim-perpetrator relationship, namely self-directed, interpersonal and collective violence[3]. Violence is expensive, for instance, it is estimated that violence in the United States of America cost about 3.3% of the country’s Gross Domestic Product (GDP) every year[2]. Although violence disproportionately affects low and middle income countries, lack of data and information on the magnitude of the problem is a major hindrance to comparisons with high income countries. In the Sub Saharan Africa violence has remained a major public health problem where together with the Latin America regions the rates of homicide are highest[3]. Like the other Sub Saharan African countries, Kenya suffers from longstanding high levels of day-to-day interpersonal violence which seldom receives attention, and the magnitude of which may be severely under-estimated by official statistics. The country also experiences some collective violence in the shape of disputes between and within communities and cross-border confrontations with neighbouring countries.Several studies conducted in Kenya have attempted to highlight the problem of violence. It has been found that 65% of Kenyan women have experienced physical or sexual violence at the hands of their husbands. It has also been reported that 50% of all women in Kenya have experienced violence since they were 15 years and that 64% of women who had separated or divorced had experienced violence since they were 15[4]. Data from the Nairobi Urban Health and Demographic Surveillance system for 2003-2005 showed that interpersonal violence was the second leading cause of premature mortality, accounting for 12.1% of years of life lost after HIV/AIDS and Tuberculosis (49.9%)[5].Violence related injuries in Kenya are either reported through the police crime reports or hospital morbidity and mortality data systems. These two data sources in most cases do not match in terms of numbers and types of injuries. For instance in 2007, the data from hospital records indicated a mortality rate of 9.37 per 100,000 populations for both self-directed and interpersonal injuries while police sources report 3.9 per 100,000 populations[6,7].This paper aims at highlighting the magnitude of violence related injuries in Kenya and advocates for urgent action to address it. It also attempts to establish which population groups bear the greatest burden of these injuries disaggregated by age and sex. The study applied guidelines for estimation of the burden of injuries as outlined in the WHO and CDC Manual for Estimating Cost of Injury due to Violence[8]. It therefore provides evidence that these guidelines are a useful tool not only for estimating the economic cost of injuries but also the magnitude of the problem in a country.
2. Methods
- Data in this study was collected in two stages. The first stage involved prospective recording of cases of injuries reporting in two hospitals – Machakos District Hospital and Kenyatta national Hospital between the months of June to September 2008. It involved capture of data on the first 100 patients who presented in each of the two hospitals with violence related injuries. This data was to provide for the characteristics of injury cases distribution by sex, age groups affected and severity of injuries. The second stage involved collection of information on all cases of injuries reported in randomly selected hospitals in 2007.
2.1. Sampling
- A random sample of 165 hospitals (30%) was drawn from the 551 accredited hospitals in the country. This was a multistage sampling where the first stage involved stratifying all hospitals according to ownership. Thus, the hospitals were categorized into public, faith-based and private hospitals. The hospitals in each category of ownership were then grouped according to their geographical regions namely Central, Coast, Eastern, Nyanza, Rift Valley and Western regions. For each of the three types of ownership and for every region, 30% of the hospitals were randomly selected. This ensured that the sample was representative of all types of hospitals and regions in Kenya.
2.2. Questionnaire
- Data collection tools were developed by the research team using the templates provided in the WHO and CDC manual for the estimation of the economic cost of violence[8]. The questionnaire captured information on number of injuries reported, with details of those that were admitted for at least 24 hours and those treated as outpatients.
2.3. Data Collection
- To each of these 165 hospitals a questionnaire was sent through registered mail and a backup soft copy by email attachment to the officer in charge of health records and information to gather incidence data on injury cases treated in their respective hospital in 2007. Data was obtained from patient registers and in-patient files. The required information was gathered from available records, such as emergency department logbooks and patient files. The questionnaires were filled by the health records officers who had full knowledge of caseloads handled by their hospital emergency departments and admission wards. Telephonic follow-ups were made by members of the research team to clarify issues on the information required to maximize on the response rate. After filling the questionnaires, the information was counter-checked by the respective medical superintendent or senior hospital administrator. All filled questionnaires were then delivered to the study team for data entry and analysis. Data were analyzed using simple Excel spread sheets through calculation of proportions and creation of cross tabulations for categories of variables.
2.4. Estimation for Incidence
- The proportional contribution of each category of hospital (public, faith-based and private) was based on the average bed capacity for each category as a measure of the size of the hospitals work load. The total number of cases recorded for each category was then computed. The total case load was then calculated by extrapolating this number by the proportion that each category contributed to the total national bed capacity.
3. Results
- There were a total of 551 accredited hospitals in the country. Of these, 165 were sampled where 86 were public, 46 were private-for-profit while 33 were faith-based hospitals. This sample represented 30% of the NHIF-accredited hospitals or 31.4% of the total bed capacity of all accredited hospitals in the country. Overall, 97 hospitals (58.8%) responded, representing 56.1 % of all beds in the sample hospitals and 17.6% of beds in all accredited hospital in the country. Participation varied by hospital ownership. Only 41% of private hospitals participated, compared to 59% of the public hospitals and 82% of the faith-based hospitals. Although the sample was chosen to be representative of all provinces, in the Nyanza and Rift Valley provinces, only 40% and 45% respectively of selected hospitals responded. In Nairobi province 58% of hospitals responded, while in the Western and Eastern Provinces response rates of 75% and 78% respectively were obtained and 87% in Coast Province.
3.1. Total Incidences of Injuries Reported in the 97 Hospitals in 2007
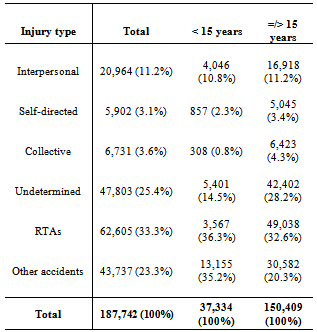
- The 97 responding hospitals reported handling 187,742 injury cases. By cause of injury, 33% were due to road traffic crashes. Other unintentional causes combined (such as burns, falls, drowning and poisoning) represented 23% of all cases. Violence-related injuries represented about 19%, of which 11.2% were due to interpersonal violence, 3.4% to self-directed violence, and 4.3% collective violence. Cases reported as being "undetermined” (whether due to intentional injury or not) accounted for over 25.5% or 47,803 cases (see Table 1).
|
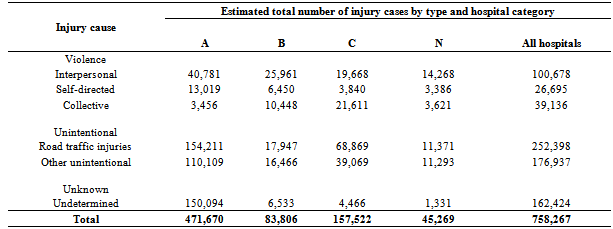
3.2. National Estimates of the Caseload of Injuries Treated in Hospitals
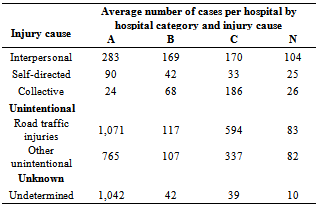
- The National Health Insurance Fund (NHIF) classifies all accredited hospitals in 4 categories (Category A, B, C, and N), based on the range of services they provide as well as other infrastructural attributes and quality of service measures (Kenya Quality Assurance Model KQM)[9,10]. Table 2 shows the distribution of injury causes by hospital category for the 97 sampled hospitals. A-category hospitals in the sample handle the most cases of all injury causes (except collective violence-related injuries), while N-category hospitals handle the fewest cases.
|
|
|
3.3. National Estimate of Deaths due to Violence
- WHO burden of disease mortality estimates for 2004 reported an estimated 7,200 deaths due to interpersonal violence (20.76 per 100,000); 2,200 due to self-directed violence (6.35 per 100, 00); and 400 (1.15 per 100,000) due to collective violence[11]. The population size at that time was 34,675,000 inhabitants. In 2007, the total population was estimated to be 36,913,721 inhabitants projected from the 1999 population census[12]. Assuming the death rates due to violence remained the same as in 2004, the total number of fatal injuries for Kenya in 2007 can be estimated to be 10,432 deaths (7,663 for interpersonal violence, 2,344 were from self-directed violence and 425 were due to collective violence). Based on this data, the interpersonal injuries caused 73.5% versus 22.4% for the self-directed and 4.1 for collective violence fatalities.
3.4. Characterization of Violence Related Injuries Based on 2 Hospitals Prospective Data
- From the prospective data from the two hospitals (Kenyatta and Machakos), it was found out that of all cases of violence treated, 63% were males while 37% were females. Of all males, 24% in the 30-44 year age group while 17% were in the 15-29 year group. Among the females, the age groups 30-44 and 15-29 were equally affected at around 26% of the total cases. Assuming that all injuries reported in the country have similar characteristics, we can estimate that of total of 272,284 reported violence related injuries, 203,072 (74.6%) were slight injuries, 58,780 (21.6) were severe/serious injuries and 10,432 (3.8%) were fatal injuries.
4. Discussion
- This study is probably the first ever to estimate the annual incidence of violence in Kenya. It also presents the most thorough and comprehensive use of hospital based data to provide estimates of violence-related injuries that received medical attention and treatment in the country. The study demonstrates that the hospital records provide plenty of information that if analyzed and packaged well can bring more insight about the distribution of injuries among age groups, sex, types and severity of injury. The findings of this study indicate that 261,852 people were attended in hospitals in Kenya in 2007 due to violence related injuries. Considering that the reported outpatient attendance for that year was 2,497,578, violence therefore contributed nearly 10% of the total number of out-patients during this period[6]. This is a significant burden considering that the health systems are already overburdened by communicable diseases and an emerging epidemic of non-communicable diseases. Like in many countries, our study found that males carry the highest burden of violence related injuries (63%) as compared to the females (37%). Most of those afflicted are within the most productive age groups of 15 to 44 years (48% for males and 52% for females). Prevention programmes therefore need to target specific groups such as the young and women for the country to realize tangible impact. This data flags out violence and injury prevention as an important public health subject that needs prioritization in health policy and practices in the country.These data reporting systems for injuries need to be improved and strengthened in particular ensuring that the same system of data capture such as WHO system of registering morbidity and mortality (ICD -10) is used in all hospitals[13]. We found that in Kenya this system of reporting is only practiced in the public and faith-based hospitals and limited in the private for-profit health providers in the country.The data collection efforts from different sources revealed at the same time the limitations of each source and the inherent gaps that exist and often result in underestimates of the real burden. Estimates on the incidence of the various forms of violence are often reported differently by various sources (police, hospitals and the Ministry of Health). The various types of violence and resulting deaths and non-fatal injuries are incompletely and inconsistently reported by different sources. For instance in 2007, the health information systems data from hospital records indicate a mortality rate of 9.37 per 100,000 populations for both self-directed and interpersonal injuries while police sources report 3.9 per 100,000 population[6, 7].The estimated incidence of interpersonal and self directed violence in Kenya in this study was about 575 per 100,000. Our study also found that violence related mortality incidence was about 28 deaths per 100,000 populations. The WHO Global Burden of Diseases provided estimates of 27.1 deaths per 100,000 population in 2004[11]. The study estimates correspond very closely with the WHO estimates done in 2004. The majority of those involved are young age groups in the range of 15 to 44 years of age. Men are more affected than women, especially those within the age group 30-44[14]. These are the most productive years, at the same time; these years bear the greatest burden of economic costs resulting from injuries due to violence. This study has various limitations since the various types of violence resulting in deaths and non-fatal injuries are incompletely and inconsistently reported by different sources. Information about cases seen in hospitals is not routinely available, and national police data on deaths appear to severely undercount the true number of cases. Without accurate numbers on the national incidence of violence in the country disaggregated by age group, type of injuries and severity, it may be difficult to target interventions for prevention purposes as well as mobilize sufficient resources for the response. There is need to harmonize the reporting formats to enable program managers in the field of violence develop appropriate policies to reduce violence in the country[15].The study relied on information from the HMIS which does not record information about the causes of injury, and may underestimate the total number of injuries arriving at hospitals because, except for public health facilities, reporting to the system is not mandatory. The Ministry of Health database only captures injury cases attended or admitted and deaths occurring in hospitals. Therefore estimates reported in this paper do not include the many violent acts in the country that never arrived in hospitals. In order to estimate the accurate incidence of violence, data from other sources are also needed. However, as noted elsewhere in this paper, the data from the hospital records do bring more insight about the distribution of injuries among age groups, sex, and severity of injury.While further special studies and surveys can help to overcome some of these problems, they are no substitute for improved vital registration and health information systems designed at the outset to include violence and injury indicators. This study has demonstrated that the approach recommended in the WHO-CDC Manual for estimating the economic costs of injuries due to interpersonal and self-directed violence[8] is feasible in a developing country context with few routinely available data. Application of the manual has provided insights into the magnitude of violence-related deaths and injuries in Kenya.
5. Conclusions
- The findings of this study reiterate the high burden of diseases occasioned by violence in the country. It further raises concern over the challenges to data collection and reporting of violence related injuries. With this report, Kenya joins other countries that have made progress in documenting their burden of violence related injuries. The challenge now is to use the findings in this report to advocate for increased investment in violence prevention.
ACKNOWLEDGEMENTS
- The authors would like to acknowledge the World Health Organization for the technical and funding support to conduct this study. We also appreciate the contribution of provincial health records and information officers who coordinated the collection of the data from hospitals.