-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2013; 3(5): 124-129
doi:10.5923/j.phr.20130305.03
Investigating Claims of Contraceptive Failure among Women of Reproductive Age in Nigeria: Findings from a National Survey
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOladipupo Ipadeola1, Chinazo Ujuju2, Jennifer Anyanti2, Samson Adebayo3
1Malaria Action Program for States, Abuja Nigeria
2Society for Family Health, Abuja Nigeria
3National Agency for Food and Drug Administration and Control, Abuja Nigeria
Correspondence to: Oladipupo Ipadeola, Malaria Action Program for States, Abuja Nigeria.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Uptake of contraceptives in Nigeria is low despite the several interventions and efforts on family planning in the country. Contraceptive failure among other factors may be responsible for this occurrence as women reason “why use it if it doesn’t work”. This paper investigates claims of contraceptive failure among women aged 15 to 49 years in Nigeria using data obtained from the 2007 National HIV/AIDS and Reproductive Health Survey. A total of 5360 women were interviewed in the study. Using the Chi Square test of association and the logistic regression, variables such as level of education, place of residence, geopolitical zones and exposure to mass media intervention on family planning were explored. Findings showed that more than 86% have ever been pregnant and about 10% had become pregnant while using contraceptive (P = 0.0992, CI =0.0888, 0.1096). Report of contraceptive failure was highest among women aged 25 years and above (85%), while self employed group were more affected than women in other occupational groups. Also, women from rural areas reported more cases of contraceptive failure than their urban counterpart (54.1% to 45.9%). Daily oral pills accounted for about 21.5% of all reported contraceptive failures while condoms and Injectables accounted for 19.6% and 13.9% respectively. Women with secondary and higher levels of education are 1.7 times more likely to experience contraceptive failure than women of lower educational level. Significant spatial pattern was observed at the level of geopolitical zones. Intervention on client adherence to pills and introducing Cyclebeads to women who prefer traditional methods may be explored.
Keywords: Contraceptives, Contraceptive Failure, Family Planning, Injectables, Pregnancy, Logistic Regression
Cite this paper: Oladipupo Ipadeola, Chinazo Ujuju, Jennifer Anyanti, Samson Adebayo, Investigating Claims of Contraceptive Failure among Women of Reproductive Age in Nigeria: Findings from a National Survey, Public Health Research, Vol. 3 No. 5, 2013, pp. 124-129. doi: 10.5923/j.phr.20130305.03.
Article Outline
1. Introduction
- The provision of contraceptives for family planning and birth control has received more attention from the international communities and donor agencies in recent times. Most of these supports are provided to African countries especially the sub Saharan Africa. Nigeria, like any other African country, is faced with the challenges of high rate of unwanted or unplanned pregnancy which poses major health challenge to women of reproductive age. Statistics has shown that 210 million pregnancies occur worldwide, with 80 million unplanned, and 46 million ending in abortion[1]. Studies have also shown that lack of awareness, lack of access, cultural factors, religion, refusal by partners or family members, beliefs of infertility and fear of health risks and side effects of contraceptives are some of the factors contributing to non use of contraceptives[2 - 5].Current contraceptive prevalence rate in Nigeria is 15%, while results from the NDHS 2008 report shows that use of any family planning method increases with age from 7% among women age 15-19 to 20% among women age 35-39, and then declines to 10% for women age 45-49[6]. Most women currently using contraceptive, use a modern method (11%), while 5% rely on traditional methods. The male condom is the most commonly used modern method (5%), followed by the injectables and pills (2% for each), while the intrauterine device (IUD) and female sterilisation are the least popular modern methods (less than 1% each). The rhythm method and withdrawal are the most common traditional methods (2% each). The contraceptive prevalence rate for modern methods has increased from 6% in 1990 to 13% in 2003 and 15% in 2008[6]. Rapid population growth and overpopulation are issues of great concern to many national governments and the international community[7 - 10]. Much of the research work done in this domain has associated high population growth rates with poverty, scarcity of land, hunger, environmental degradation and political instability[11- 14]. Nigeria is the most populous country in Africa, with an estimated population of 150 million people[15]. The country has one of the highest mortality rates in sub-Saharan Africa, the second highest number of maternal deaths in the world. One of seven women (14%) has attempted abortion while 10% ended in unwanted pregnancy[16]. In spite of the efforts made by the government in this direction, the uptake of modern birth-control in Nigeria remains grossly insufficient[17 – 19]. In Nigeria, contraceptives are made available at a highly subsidized rate through social marketing. Awareness programmes through mass media, interpersonal communications and outreaches are conducted on regular basis and knowledge of the benefits of family planning uptake has increased among women in Nigeria. However, contraceptive efficacy remains a concern. One of the determinants of use or uptake of any health commodity or practice is the perceived efficacy of such product and service. There are claims that women get pregnant while using one or other contraceptive. Programme managers in FP have reported that use of contraceptives may be dwindling as a result of failure rate, “why use it if it doesn’t work?” We investigated the claims of contraceptive failure among women in Nigeria tried to identify factors responsible with a view to improving FP uptake.
2. Methodology
2.1. Data
- The Federal Ministry of Health (Nigeria) in collaboration with the Society for Family Health received funding from the United States Agency for International Development (USAID) and the British Department for International Development (DFID) to conduct the first national survey on HIV/AIDS and Reproductive Health (NARHS) in Nigeria in 2003. NARHS aimed at assessing sexual and reproductive health (SRH) and the factors influencing the later as well as the impact of ongoing health interventions in Nigeria. The survey was repeated in 2005 and 2007. Women aged 5 to 49 years and men 15 to 64 years old were eligible for participation in the surveys. Selection was based on a three-level multi-stage probability sampling technique. This paper explores the 2007 dataset in investigating claims of contraceptive failures in Nigeria. A nationally representative sample of females aged 15-49 years and males aged 15-64 years living in households in rural and urban areas in Nigeria was drawn from the updated master sample frame of rural and urban localities developed and maintained by the National Population Commission (NPC). The study area consists of all the 36 states of the Federation and the Federal Capital Territory. Probability sampling was used for the survey. The sampling procedure was a (four-level) multi-stage cluster sampling aimed at selecting eligible persons with known probability. Stage 1 involved the selection of rural and urban localities. Stage 2 involved the selection of Enumeration Areas (EA) within the selected rural and urban localities. Stage 3 involved the listing of eligible individuals within households while stage 4 involved selection of actual respondents for interview and testing. Overall, 11,822 respondents were selected for interview of which 11,521 were successfully interviewed resulting in a 2.5% non response rate.
2.2. Data Analysis
- For the purpose of analysis, simple frequency tables were used to describe the socio and bio-demographic characteristics of the respondents. Bivariate Chi-square analysis was used to test for association between the dependent and proposed independent variables, while the logistic regression was used to identify and quantify degrees of contribution of each of the independent variables. The model utilized ever experienced contraceptive failure against selected background characteristics such as age, education, marital status, social economic status knowledge of contraceptives and types. The Chi-square statistic is calculated by finding the difference between each observed and theoretical frequency for each possible outcome, squaring them, dividing each by the theoretical frequency, and taking the sum of the results. Logistic regression analysis extends the techniques of multiple regression analysis to a research situations in which the outcome variable is categorical.[20]. Variables considered in the analysis are marital status, age at the time of pregnancy, level of education, socioeconomic status, place of residence, geopolitical zones and type of contraceptives used. The response variable is the question whether respondents were pregnant while using contraceptives. All analyses were performed using SPSS version 17 and STATA SE 10. We define the response variable as y, and denote the event y = 1 if respondent became pregnant while on contraceptives and y = 0 if otherwise. Positive association was evident for all variables considered. All the tests were carried out at α level of 0.05.
3. Results and Discussion
3.1. Socio Demographic Characteristic of Respondents
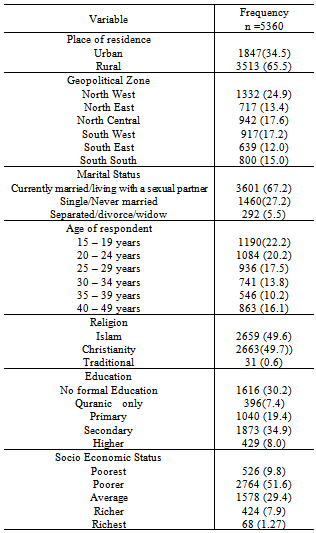
- The 2007 NARHS dataset had responses from a total of 5360 women of reproductive ages from the 36 states and FCT Nigeria. About 66% resides in the rural areas, 67% were currently married or living with a sexual partner as at the time of the survey, while 27% were single. Women less than 25 years were about 40% of the total respondents and constitute the highest in the age categorization. About 50% of the responsible mentioned that they Christians while the Muslim population among the respondents was also 50%. About 30% had no formal education while 42% had secondary and higher levels of education. Over 50% of the respondents belong to the poorer socioeconomic class as observed through ownership of asset while only 10% belong to the richest socio economic class. (See table 1). Among the respondents, mean age at sexual debut, first pregnancy, first marriage and first birth are 17.01 18.58, 17.75 and 18.99 respectively.
|
3.2. Knowledge and Use of Contraceptive
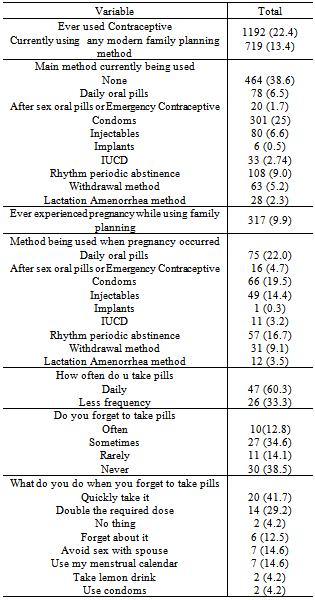
- Table 2 describes variables on knowledge and use of contraceptives. About 73% percent of the women knew at least one method of contraception compared to 82% of men who knew any method. Regarding modern contraceptive methods, 68% of women and 79% of men knew at least one method. While 78% of all the male and female respondents knew of at least one contraceptive method, 74% knew of at least one modern contraceptive method and 51% knew at least one natural family planning method. Among the modern methods, the most known method by men and women were male condom (65%), injectibles (37%) and female sterilization (21%).The percentage of all female respondents that were currently using any modern contraceptive method as at the time of the survey was 10% while that of all men was 16%. Thirteen percent of all females and 18% of all males were recorded to be using any method of contraceptive/child spacing at the time of the survey. The proportion of non-users of contraceptives that indicated intention to use modern contraceptives was 20% among the males and 13% among the females. Almost half of the respondents (44%) indicated that decisions about use of family planning methods should be jointly undertaken by the couple, while a fifth (20%) expressed the opinion that the husband should take the decision alone and 5% indicated that it should be the wife’s decision alone. A higher proportion of the respondents desired to have five or more children (35%) compared to those that desired maximum of four children (24%). However, 34% of the respondents expressed the opinion that the number of children they would want to have was “up to God”. (See table 2)
|
3.3. Contraceptive Failure by Method
- Result showed that users of traditional methods experienced more contraceptive failures than users of modern methods. Also pills accounted for the highest failure reports as about 27% of respondents with failed contraceptives were either using the daily oral pills or the emergency/after sex oral pills. About 3.2% were using IUCD while 14% were using injectibles. Chart 1 summarises the cases of failure with respect to contraceptive method used.
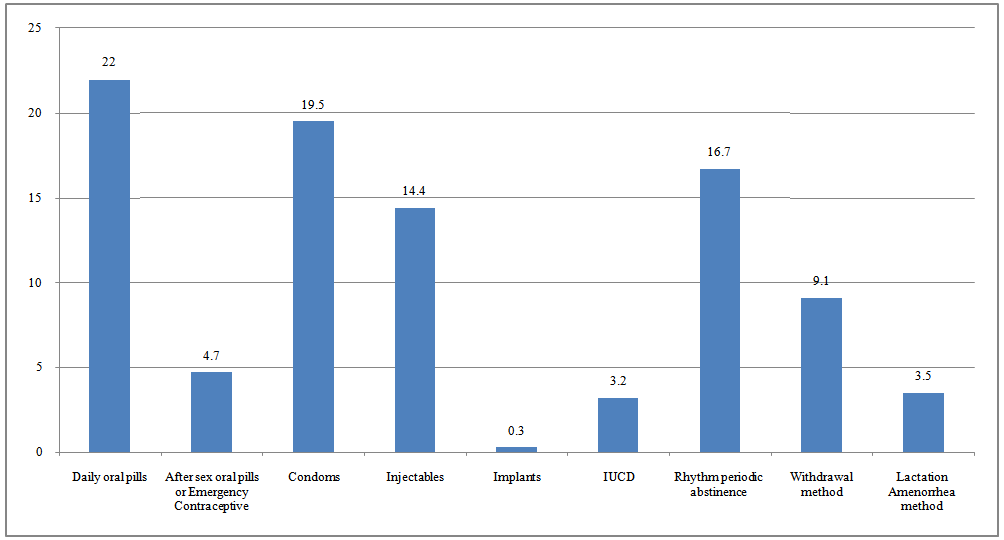 | Chart 1. Percentage distribution of Contraceptive failure by method used |
|
3.4. Test of Association
- Out of 5360 women involved in the study, more than 86% of them have ever been pregnant and about 9.9% of these reported they had become pregnant while still on contraceptive therapies. This proportion was found to be statistically significant (P = 0.0992, CI = 0.0888, 0.1096). Women above 25 years were found to have reported the highest number of contraceptive failure cases (85%) while self employed women were more affected than any other occupation group (about 41%). Result also showed women from rural areas were more affected than their urban counterpart (54.1% to 45.9%) while more than three quarter of the reported cases were from the currently married women (87.3%). The type of contraceptive methods used at the time of pregnancy was considered, daily oral pills accounted for about 21.5% of contraceptive failures, while condoms and Injectables accounted for 19.6% and 13.9% respectively. The traditional methods accounted for the highest failure as about 29 percent of users of traditions methods (periodic abstinence, withdrawal and Lactation amenorrhea method) reported contraceptive failure.
3.5. Output from Logistic Regression
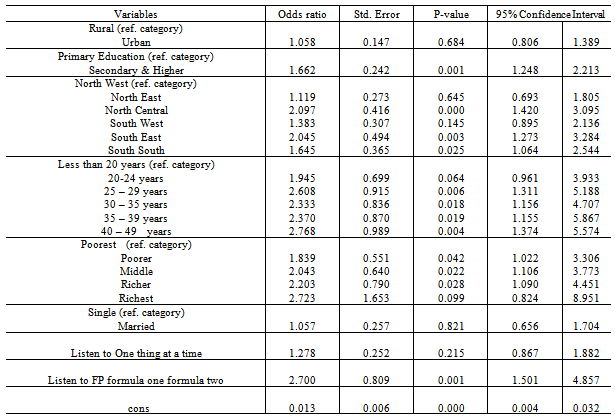
- Table 3 shows output of the logistic regression. Level of education, age of respondent, geopolitical zones and listening to radio program were significant predictors of contraceptive failure among the respondents. Significant and positive association was evident with poorer (OR=1.838, p=0.042), middle (OR=2.042, p=0.022) and richer (OR=2.203, p=0.028) women. Thus, women in the poorer, middle and richer classes of socioeconomic status are more likely to experience contraceptive failure compared to women in the poorest class (P value <0.05) while women with secondary and higher levels of education are about 1.7 times more likely to experience contraceptive failure than women of lower educational level (P value < 0.001). Women older than 25 years are more likely to experience contraceptive failure than those who are younger. Significant spatial pattern is observed at the level of geopolitical zones with p<0.05 except in the North West.
3.6. Discussion
- Contraceptive failure was reported mainly by women with secondary and university education, women in the middle social economic status and self employed women. These women are likely to have busy schedules and fail to adhere to the instructions on use of the contraceptive method. Longer term methods and provider dependent methods which have been reported to experience low failure rate should be recommended for busy women to reduce the chances of contraceptive failure. Several studies suggest long term and permanent methods be made available for these women. Long term methods have also been proved to have reduced up-front costs and many women prefer them to shorter acting methods, an advantage that should be a convincing argument for governments and donors that subsidize contraception [21].Investigating claims of contraceptive failure among women and the possible factors responsible for contraceptive failure is expedient as contraceptive failures impact on level of induced abortion. The unintended pregnancy as a result of contraceptive failure also affects the health and economic status of Nigerian families. Findings from this paper will provide opportunity for government and donor driven programmes to enhance appropriate policy formulation.Modern family planning methods have been proven to be very effective in preventing unplanned pregnancy when used properly. The effectiveness of the modern family planning methods depends on user’s compliance with instructions on use. On average, about 5 out of 100 couples will get pregnant in a year while using the daily oral pill[22]. Findings show that daily oral pills were reported to have highest failure of all the modern methods. Failure could be attributed to inconsistent use as many of the users reported they forgot to take pills often.Traditional methods such as rhythmic periodic abstinence, withdrawal and Lactation amenorrhea method accounted for about 29 percent of contraceptive failure. Introducing Standard Days Method of family planning using Cyclebeads to women who prefer traditional methods because of religious and cultural reasons may be an option[23]. Improvements in the use of traditional methods, for example using the Standard Days Method for periodic abstinence, can dramatically decrease failures of these contraceptive methods[24].
4. Conclusions
- It is evident that a significant proportion of the women who were on contraceptives experienced pregnancy justifying the claims of contraceptives failure. Also daily oral pills and traditional methods accounted for the highest number of reported failure cases. Failure in the daily oral pills is as a result of users not adhering strictly to the doctor’s prescription or inconsistent use. Busy women should be encouraged to adopt the provider dependent modern family planning method. There is need for scale up of awareness campaign on uptake and proper use of the existing family planning methods and users of pills should be encouraged to involve their partners to support them in ensuring adherence which will benefit the family as a whole.
ACKNOWLEDGEMENTS
- The authors would like to acknowledge Society for Family Health and the Federal Ministry of Health, Nigeria, for making the data available.
Conflict of Interest
- The authors declare no conflict of interest. Furthermore, no financial support was received for this work as the data used were secondary data.