-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2013; 3(5): 116-123
doi:10.5923/j.phr.20130305.02
To Disclose or Not to Disclose HIV Status: The Dilemma of Religious Adherents of Tema Metropolis and Ashaiman Municipality in Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBenson Nkansa-Kyeremateng
Presbyterian University College Ghana, Akuapem Campus, Eastern Region, Ghana
Correspondence to: Benson Nkansa-Kyeremateng, Presbyterian University College Ghana, Akuapem Campus, Eastern Region, Ghana.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
HIV status disclosure rate has often been used as a proxy to measure the levels of perceived or real stigmatization of persons living with HIV/AIDS in a community. The study examined the willingness of religious adherents of the two study areas in Ghana to disclose their HIV/AIDS status in religious settings. Using hypothetical questions adherents of Orthodox, Pentecostal/Charismatic, African Independent Churches, Islam and African Traditional Religion were quizzed during periods of forenoon services to elicit the relevant information for the study. Overall, the outcome of the study indicated that more than half of the respondents in both areas were willingness to disclose HIV status especially to their religious leaders than to their respective whole congregations. Adherents of Pentecostal/Charismatic and African Independent Churches were more willing to disclose their HIV status. Female adherents as well as those with higher levels of education were also more willing to disclose their HIV status. The need for care and support, for prayers and counseling were the main motivation for disclosure while the fear of being gossiped about, isolated and blamed constituted disincentive for disclosure. To promote the level of HIV status disclosure within the religious setting there is the need for religious leaders to provide care and support for persons living with HIV/AIDS.
Keywords: HIV/AIDS, HIV Status Disclosure, Religious Adherents, PLWHA
Cite this paper: Benson Nkansa-Kyeremateng, To Disclose or Not to Disclose HIV Status: The Dilemma of Religious Adherents of Tema Metropolis and Ashaiman Municipality in Ghana, Public Health Research, Vol. 3 No. 5, 2013, pp. 116-123. doi: 10.5923/j.phr.20130305.02.
Article Outline
1. Introduction
- Persons living with HIV/AIDS (PLWHA) when they have come to know of their HIV sero-positivity are normally faced with the problem of disclosure, that is, whom to share the information with, how to go about it and when to do it. Persons living with HIV therefore find themselves in a dilemma when confronted with the phenomenon of HIV status disclosure in the light of the benefits and problems that come with it. According to[1] disclosure of one’s HIV sero-positivity status may provide the opportunity of receiving social support in order to cope with the disease. Disclosure also has the potential of reducing HIV infections, particularly, of the sexual partner[2], by raising awareness and decreasing risky behaviours[3]. It may also lead to provision of appropriate medical care for the PLWHA. On the other hand, not disclosing one’s HIV sero-positivity can be a way of protecting oneself against stigmatization and discrimination[4], as the disclosure has the potential of leading to physical violence, fear, worry, shame, rejection or abandonment[5]. Non disclosure of one’s HIV positive status also has the potential of interfering with accessing and adhering to appropriate and critical medical treatment[3]. [6] and[7] have noted that most studies of HIV self disclosure in Sub Saharan Africa have focused primarily on disclosure to sexual partners and spouses especially among women. Few studies examined disclosure to others in the social network[8] including the religious communities[7] and such studies including[9],[10],[11] and[12] are mainly from the Eastern and Southern Africa.[13], however, have stressed that religion is among the many factors which influences HIV positive status disclosure beyond the caregiver-patient dyad, though findings have been somewhat inconsistent. The virtual lack of research in the area of HIV status disclosure in the religious setting in West Africa and for that matter Ghana necessitated this study. The main concern of the study was therefore to assess HIV-self disclosure in religious settings using hypothetical questions for religious adherents of Orthodox, Pentecostal/Charismatic, African Traditional Religion, African Independent Churches and Islam in two areas, namely, Ashaiman Municipality, an urban slums, and Tema Metropolis, an industrial hub of Ghana. Specifically, the study sought to probe into the nature of religious adherents’ HIV status disclosure to the religious community if they were to become infected; identify the reasons for disclosure or otherwise of HIV status in the diverse religious settings.
2. Methodology
- The study was situated in the two communities of Ashaiman Municipality, an urban sprawl, and Tema Metropolis, an industrial hub and the main harbour city of Ghana. The two study areas lie along the eastern coast of Ghana, about 30 kilometres away from Accra, the capital city of Ghana, with Ashaiman Municipality lying a little inland. While Tema Metropolis is planned with all the modern facilities that one can think of, Ashaiman Municipality is an unplanned community developed into urban sprawl with all its associated problems. The two communities have numerous religious groups which co-exist peacefully, with the Pentecostals constituting the largest group followed by the Protestants. The data for this research were secured from a survey carried out by the researcher in the two study areas in 2010.The main research instrument used was self-administered questionnaire. The structured questionnaire apart from capturing the demographic characteristics of the respondents also had questions which measured the following:i. HIV status Disclosure to the religious Community: This was captured using an index made up of two questions:a. If you were HIV positive, would you tell your pastor? Yes/Nob. If you were HIV positive, would you want your congregation to know? Yes/NoAn affirmative answer (that is, Yes) to any of the questions meant that the respondent was in total agreement with the index being measured. The disclosure of HIV/AIDS status to the religious community in the two study areas was examined in the light of an index which was constructed as well as the individual questions that make up the index with respect to religious affiliation, gender and level of education of religious adherents.ii. Reasons for Disclosure and non Disclosure of HIV status: These were solicited from respondents using this question: If you were HIV positive, would you tell your religious leader? If Yes, give reasons, If No, give reasons.The study population for the research was made up of Religious adherents of the following religious traditions found in the study areas: Orthodox Churches (Presbyterian, Methodist, Catholic and Anglican Churches), Pentecostal/Charismatic Churches (Pentecost, Assemblies of God, Apostolic Churches), African Independent Churches (Kristo Asafo, African Faith Tabernacle and Church of the Lord), Islam (Ahmadiyya and the Sunni) and African Traditional religion (Worshippers who worship the Supreme Being through the lesser gods).A multi-staged sampling method comprising purposive and convenience sampling methods as well as stratification procedures was employed to sample 100 religious adherents from Ashaiman Municipality and 150 religious adherents from Tema Metropolis. The sample sizes chosen for the respective areas as well as the various religious adherents were in proportion to their populations according to the 2000 population census of Ghana. The data for the research were analyzed using the SPSS package. The data thereof were presented in the form of tables and bar charts.
3. Results and Discussions
3.1. Sample Description
- The number of religious adherents selected in the study for the Tema Metropolis was 150 while that of Ashaiman Municipality was 100. In terms of gender, 52 percent of religious adherents from Tema Metropolis were males while in Ashaiman Municipality they constituted 46 percent. The age distribution shows that 70 percent of the respondents from the Tema Metropolis were within the age group of 18 to 35 years, 22 percent were within the age group of 36 to 49 while those who were aged 50 years and above made up 8 percent. In the case of Ashaiman Municipality the 18 to 35 years were made up of 71 percent of the respondents, the 36 to 49 age group constituted 19 percent while those were aged 50 and above made up 10 percent of the respondents. What was clear in both study areas were that the respondents were chosen to reflect the youthful nature of the population which is characteristic of urban populations. The small percentage of respondents reflecting 50 years and above also reflected what pertains at the national level. The educational background of respondents showed that in Tema Metropolis 9 percent did not have any formal education, 13 percent had primary education while 39 percent each constituted those who had secondary and tertiary education. In the case of Ashaiman Municipality those who did not have formal education formed 12 percent, 18 percent were those who had primary education, 46 percent were those who had secondary education while those with tertiary education constituted 24 percent. The employment status of respondents showed that in Tema Metropolis 28 percent had formal employment, 29 percent were self-employed, 7 percent were unemployed, 34 percent were students and 2 percent were retired. In the case of Ashaiman Municipality 19 percent of respondents were formally employed, 40 percent were self-employed, 8 percent were unemployed, 31 percent were students and those on retirement constituted 2 percent.With respect to marital status, the study showed that 57 percent of respondents from Tema Metropolis were not married, 3 percent of the respondents were cohabitating, while 37 percent were in marriage relationships with only 3 percent in other relationships (divorced or widowed). In the case of Ashaiman Municipality, 47 percent of the respondents were not married, 14 percent were cohabitating, and 37 percent were married while 2 percent were in other relationships, either divorced or widowed. Apart from the religious affiliations of respondents which have been dealt with in the methodology, 89 percent of respondents attended religious activity at least once a week in his or her religious organization in Tema Metropolis. In the case of Ashaiman Municipality 96 percent of respondents attended a religious activity at least once a week.
3.2. Willingness to Disclose HIV Status and Religious Affiliation
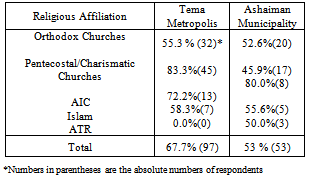
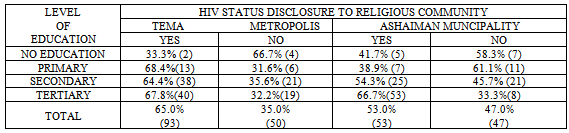
- Disclosure rates are often seen as a proxy for the amount of real or perceived stigma in a society[10]. Disclose rates have also been noted to be generally low in Sub-Saharan Africa, partly due to high levels of stigmatization[14]. Disclosure within the Church, and for that matter in the religious community, is seen as a way of reducing stigma. This assertion was affirmed by[12] when it stated that if one can ‘break the silence’ by disclosing, and be accepted by one’s fellow congregants, this may disrupt the perception that ‘other’ people get HIV, and that it is morally reprehensible. Several factors including education, religion, gender and relationship to the one to whom the disclosure is made have also been shown to influence disclosure of positive sero-status beyond caregiver-patient dyad[13].Table 1 shows the performance of the index used in the two study areas. From the table, religious adherents in Tema Metropolis were more likely to disclose their HIV status to the religious community than those in Ashaiman Municipality. This is because 67.7 percent of religious adherents in Tema Metropolis were willing to disclose to the religious community as against 53 percent of religious adherents in Ashaiman Municipality.
|
3.3. Respondents Gender and Educational Background and Willingness to Disclose
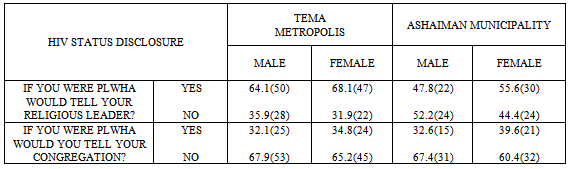
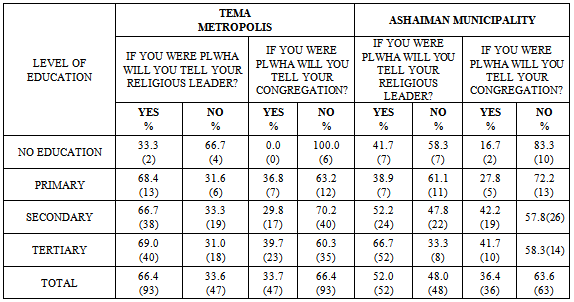
- The HIV status disclosure was also examined using the index and individual questions composing it in the light of the gender and educational background of religious adherents.
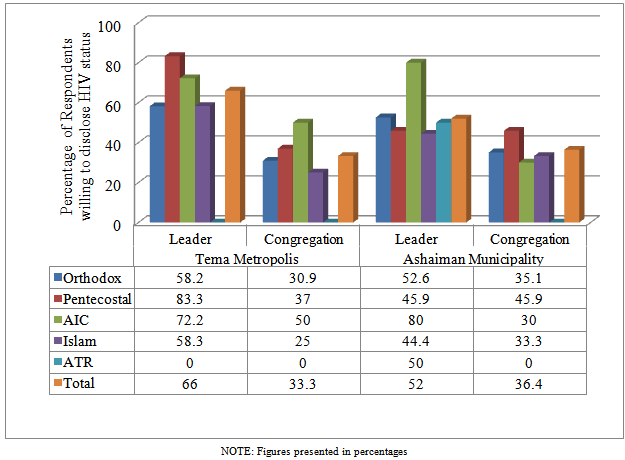 | Figure 1. Disclosure of HIV Status to Religious Leaders and Congregations |
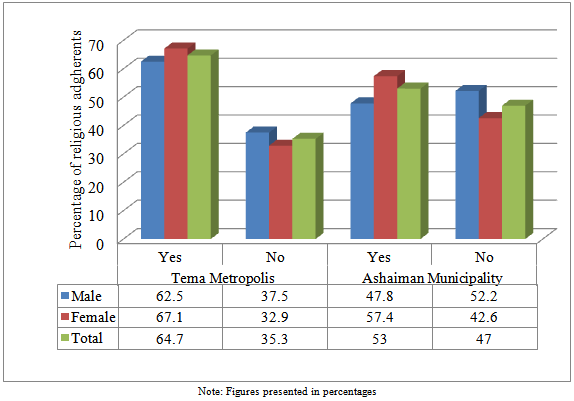 | Figure 2. Hiv Status Disclosure to Religious Community by Gender Using Index |
|
|
|
3.4. Reasons for HIV Status Disclosure and Non Disclosure
- In the main questionnaire questions were asked to solicit reasons for why respondents will or will not disclose their HIV status in a religious setting. The study realized three main reasons why religious adherents were ready to disclose their status. These were a) the need to be prayed for so that they could be healed b) to receive care and support and c) for counseling as shown in figure 3.
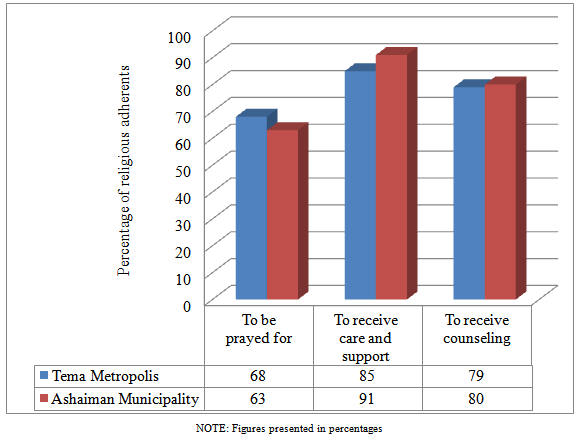 | Figure 3. Reasons for Disclosure Of Hiv Status to the Religious Community in Tema Metropolis and Ashaiman Municipality |
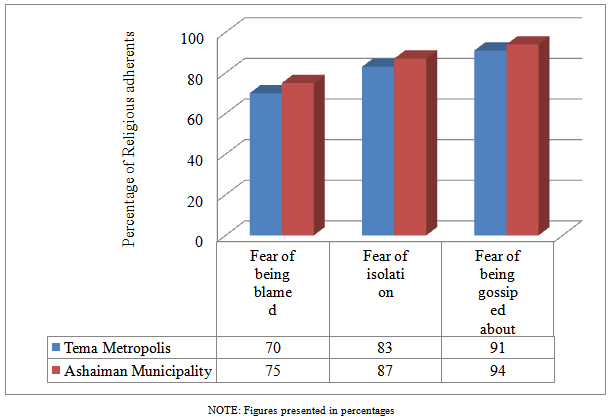 | Figure 4. Reasons for Non-Disclosure of Hiv Status to the Religious Community in Tema Metropolis and Ashaiman Municipality |
4. Conclusions
- In general the willingness to disclose HIV status among adherents in the two areas was above average. In both areas, adherents were more willing to disclose their HIV status to their religious leaders than to their congregations. Female adherents were more willing to disclose their status than their male counterparts. Adherents with higher levels of education were also more willing to disclose their status than those with lower levels of education. This means that religious leaders need to be equipped with HIV counseling skills so that they can be of help to PLWHA who come to them. With respect to reasons for disclosure, majority cited care and support and the need for counseling as reasons why they would disclose their status. For those who said they would not disclose HIV status, they cited fear of being gossiped about, isolated and blamed as their reasons. This implies that religious authorities need to educate their members so that their places of worship will become havens where PLWHA can run to for shelter.