-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2013; 3(3): 71-78
doi:10.5923/j.phr.20130303.06
Efficacy of Instructional Training Program in Breast Self-Examination & Breast Screening for Cancer among University Students
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFathia Attia Mohammad1, Magda Mohammad Bayoumi2, Mona Mohammad Megahed3
1Lecture of Medical-Surgical Nursing faculty of Nursing, Zagazig University
2Assistant Professor-Medical surgical department, college of applied medical sciences- Mohail Assir, King Khalid University
3Lecturer of Maternity and pediatric department, college of applied medical sciences- Mohail Assir, king Khalid university
Correspondence to: Fathia Attia Mohammad, Lecture of Medical-Surgical Nursing faculty of Nursing, Zagazig University.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Background: Breast self examination (BSE) is accepted method for early detection of breast cancer (BC), it could detect 40% of breast lesion, which vital for effective treatment. BSE education and adherence are a gateway to health promotion behaviors . Objectives : the current study were to assess : the students' knowledge, attitudes & practices regarding BSE &BC, the effectiveness of instructional training program on student's knowledge, attitudes & practices and the effectiveness of BSE in early detection of BC. Methods: quasi-experimental design was conducting among 100 students at education &science collage, King Khalid university Mohail Asser between December 2011 to March 2012. Tools of data collection including three instruments, (pre/post program questionnaire sheet , attitude rating scale & an observational checklist. Results: Mean age of the students was 21.6±3.1, 73% of them hadn't information about BSE and 73.8% didn't practice BSE. A statistically significant difference persisted between the pre/ post scores of knowledge & practice BSE (p<0.05). The intervention program had a positive effect on student's knowledge, practice and attitude(p<0.05). Conclusion: the instructional educations improve students' knowledge, modify their attitude, and empower them to take health decisions for BSE, national educational programs for students must be applied to increase their knowledge & improve health literacy. Research was financial supported from King Khalid University by number 11\032
Keywords: Cancer, Breast Cancer, Breast Self-examination
Cite this paper: Fathia Attia Mohammad, Magda Mohammad Bayoumi, Mona Mohammad Megahed, Efficacy of Instructional Training Program in Breast Self-Examination & Breast Screening for Cancer among University Students, Public Health Research, Vol. 3 No. 3, 2013, pp. 71-78. doi: 10.5923/j.phr.20130303.06.
Article Outline
1. Introduction
- Cancer is an important factor in the global burden of disease. The estimated number of new cases each year is expected to rise from 10 million in 2002 to 15 million by 2025, with 60% of those cases occurring in developing countries (1).Breast Cancer (BC) in women is a major health burden worldwide. It is the most common cause of cancer among women in both high and low income countries (2). According to world health organization (WHO) cancer has become a national health priority &BC has become one of the most important health problems for women in Arab countries (3). In Bahrain, Egypt, Jordan, Kuwait, Lebanon, Oman, Saudi Arabia and Tunisia, BC is commonly diagnosed in women under the age of 50(4).BC is at the top among all the malignancies seen in Saudi females, comprising of 21.8%. In addition, BC in young Saudi's women is a crucial problem, with the proportion of young age-onset. BC that developed before the age 40 accounted for 26.4% of Saudi females BC compared with only 6.5% in USA (5).BC is one of the most common reasons for death among women; diagnosis at an earlier stage of the disease allows women more treatment choices and a greater chance of long-term survival (6). Imaging studies that are recommended for early detection of BC cannot be routinely applied in countries with restricted health service resources (7).The etiology of BC is unknown; numerous risk factors may influence the development of this disease including genetic, hormonal, environmental, socio-biological and physiological factors (1). BC is amenable to almost complete cure in its early stages but to seek medical help early in the course of disease, women must be able to recognize symptoms of BC through routine performance of practicable screening (8). Thus it is important to educate the public about importance of early detection of BC by screening (9). BC screening comprises breast self-examination (BSE), clinical breast examination (CBE) and mammography (8, 10).Unlike CBE and mammography, which require hospital visit and specialized equipment and expertise, BSE is inexpensive and is carried out by women themselvesAmerican Cancer Society (ACS)recommended that BSE as an option for breast awareness and early detection of BC. Early detection and effective treatment are important to reduce morbidity and mortality. The low survival rate of young breast cancer patients have been reported due to being diagnosed at advanced stages (11). In fact, BSE alone is believed to be appropriate and effective methods of ensuring early detection of BC. Moreover it is known as an easy, cheapest &empowers self-monitoring especially among the high risk group &detects 40% of breast lesion among women (12). BSE is an examination method that can be applied easily by each woman at her home, may lead early diagnosis in a short time, no need any cost, privacy is kept, a non-invasive process and only takes five minutes of women (13).The value of BSE is controversial (14), it benefits women in two ways: women become familiar with both the appearance and the feel of their breasts and detect any changes in their breasts as early as possible (15). Although there were a lot of studies about knowledge of BC and practice of BSE in female university students (16), there were few studies about the knowledge of BC and practice of BSE in the age group of 14–19 years (17, 18).The adolescent period is a time of rapid change that provides teaching opportunities for shaping health behaviors into adulthood. For example, teaching breast self-care may encourage positive behaviors such as performing BSE& seeking regular professional breast examinations (17). For younger women, BSE education and adherence are a gateway to health promotion behaviors which set the stage for adherence to clinical breast examination and mammography screening later in life (19).Clarke and Savage (20) reported that BSE can be taught by a variety of professionals including nurses, physicians, trained peer educators, researches and graduate students without major differences (21). Health care providers should instruct women about proper technique as well as the benefits and limitations of BSE.(22,23). According to ACS recommendations, women should know how their breasts normally feel and report any breast changes promptly to their health care providers. BSE is an option for women starting from the early 20 s (24). Availability of brochures, pamphlets and shower cards, for example, are important as a reminder to women to use BSE on a regular basis. Finally, providing information on the effectiveness and importance of BSE as an early detection tool is important (25). So the present study conducted aimed to investigate the effectiveness of instructional training program for breast self-examination (BSE) on student's knowledge & practices & its effectiveness in early detection of breast cancer.
2. Subjects &Methods
2.1. Design
- A quasi-experimental design, with pre-post assessment was utilized to conduct the study.
2.2. Settings and Sample
- The study was conducted In College of Education & Sciences, KKU University from Decamper2011 to March 2012. A Systemic random sampling of 100 students was applied.
2.3. Tools of the Study
- The data were collected by using:-First tool was Pre-post questionnaire sheet-Second tool was (Liker's’ scale)-Third tool was an observational checklist. The first tool was developed by the researchers in an Arabic language, based on literature review and experts’ opinions. The questionnaire was pre-tested on convenient sample of 10 female university students& excluded from study participants, and revised accordingly. It included multiple choice & true & false questions. First questionnaire was divided into three parts.First part(8) questions:It included demographic characteristics of students such as age, height &weight marital state, age of menarche, using of contraceptive, family history to breast cancer Second part (8)questions:It included questions among breast cancer such as incidence rate at KSA, risk factors, prevention & management strategiesThird part( 17) questions:It included questions among breast self-examination such as benefits, when & how done as well as barrier to done.Scoring Scheme of knowledgeEach correct response was scored one (1) point and each wrong response was scored zero (0). Total score <60% was considered unsatisfied, where >60% was satisfied.The second tool (22) questions:It included questions among students' attitudes regarding breast cancer & breast self-examination. It was designed by the investigators in accordance with the needs of this study, Scoring Scheme attitude 5 Liker's’ scale (strongly agree/agree/neutral/not agree/ strongly not agree) was used (46) The scoring was reversed for the negative knowledge item. For a positive attitude item, scores of ‘4’, ‘3’, ‘2’, ‘1’ and ‘0’ for ‘strongly agree’, ‘agree’, ‘neutral’, ‘disagree’ and ‘strongly disagree’, respectively. This scoring was be reversed for the negative attitude items.The third tools is an observation check-list developed by Long et al (1993) (47), was the 3rd tools in current study, used as a pre-post training test to evaluates student’s practice of breast self-examination. It involved 10 steps, marked as not done=0, done incorrectly=1 and done correctly=2. The total correct score of practice was 20 points. We used breast palpation Gaumard model in assessing &teaching participants' steps of BSE.Preparatory phase:A review of the current national and international related literature was done by the researchers, questionnaire sheet, attitude scale, were designed by the researchers in Arabic language and was given serial numbers.Pilot study:A pilot study was carried out on 10 students at the mentioned setting, its aim was to evaluate the feasibility and clarity of the tools. Based on the pilot study results, the designed tools have been modified. The group of students who were tested in the pilot study was excluded from the total study sample.Ethical considerations:The Ethics and Research Committee in KKU was approved the study protocol. Confidentiality of the subjects were also assured through coding of all data. The researchers assured that the data collected and information will be confidential and would be used only for the purpose of the study.The field workThe present study was carried out along a period of 4 months, two day weekly. The assessment phase lasted for one month. The implementation phase of the program and post-test took 3 months. In assessment phase , the questionnaire sheet & attitude rating scale were distributed to the student's participants as well as an observational checklist was applied after demonstrated the objective of the study as a pretest for preparing program. The questionnaire sheet and attitude rating scale takes 20-30 to completely filled & observational checklist applied by researcher for each student and takes 5-10 minutes. The training program was conducting; its aim was to provide accurate knowledge, in addition to acquiring practical skills, and modifying related misconceptions. It was revised and modified to fit cultural and socio-demographic aspects of the study participants.BSE training program that is given to the participated students composes CD, booklet and posters that are prepared by researchers in Arabic language after review related literatures and includes data about anatomy of breast, epidemiology of breast cancer, risk factors at the breast cancer, signs & symptoms of breast cancer, early diagnosis methods, management strategies, principles of and time of BSE method. The participating students were classified into groups according to their academic schedule. The training has been given to the each group separately and training program took averagely 45-60 minutes. Program implementation was in the form of small group sessions, the program content has been sequenced through 10 sessions (2 sessions for pre-test 6 sessions for program implementation (2 sessions for theory and 4 sessions for practice) and 2 sessions for posttest and observation check list). Group consisted of 25 students chosen according to academic schedule. The lists of participants were prepared and provided to the administration office for agreement, and then printed and distributed in different sitting. Statistical AnalysisThe statistical analysis of data done by using excel program for figures and SPSS (SPSS, Inc., Chicago, IL). program statistical package for social science version 16. The description of the data done in form of mean (+/-) SD for quantitative data. And Frequency & proportion for Qualitative data.The analysis of the data was done to test statistical significant difference between groups. Chi-Square test was used to compare qualitative dataSpearman correlation test was used to test association between variablesN.B: P value is significant if < or = 0.05 at confidence interval 95%.
3. Results
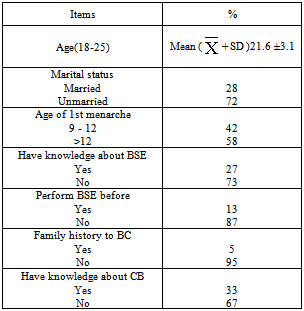
- Total number of 100 students was selected randomly to participate in the study; the mean age of participants was 21.6±3.1 years. Nearly to 3 quarter were unmarried, & hadn’t knowledge about BSE (72% & 73%, respectively). Majority of them hadn't performed BSE in past(87%), only33% had knowledge about CB & only 5% had family history to BC (table ,1).
|
|

|
4. Discussion
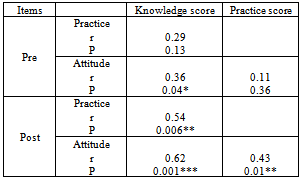
- Breast cancer is currently the top cancer affecting women in the entire world and the leading cancer killer. Early detection of breast cancer can lead to greater like hood of cure and remains the cornerstone of breast cancer control. Breast self-examination is one way for woman to know how her breasts normally fell. BSE is highly significant for younger age women(26).The current study aimed to assess the students' knowledge & practices among BSE, assess the effectiveness of instructional training program for BSE on student's knowledge & practices & assess the effectiveness of BSE in early detection of BC. The mean age of students was 21.6+3.1, most of them were unmarried.Regarding evaluated breast cancer risk factors among study participants, the most frequent identified risk factors were genetic, smoking, non-lactating women , oral contraception, more fat intake, exposure to x-ray and obesity, our results are similar to study conducted among Malaysian female university students(27) . In our study students not appreciate early menarche as major risk factors, this result as the same reported by previous studies in different population (27,28). Only 13% of students reported BSE practicing, their barriers to practice BSE clarified by no one breast cancer infected in their families, not have any breast cancer symptoms, think it's not important and not know techniques, this findings similar to those reports elsewhere (29& 30).Regarding to breast cancer precaution; avoidance of alcohol, smoking, appropriate body weight, low fat intake and increase vegetables were the most protective measures revealed among our study sample. Mass media was easily available and provide broad range of information, this explain our results that mass media represented the most common source of information for breast cancer among students, followed by booklets and magazines, similar findings were reported in previous studies (31, 32,&33).The present study revealed that students had a lack of knowledge about breast cancer, the most common cancer affected women. More than half of them had unsatisfactory level of knowledge pre -program implementation and more than half had a negative attitude. Previous studies confirmed our result (34,35, 36&37). few number of our study sample practice BSE pre- intervention additionally more than two third of them practice it incorrect. This finding is same as another study conducted among young females aged 20 years, 35% performed BSE ,slightly more than half did it inaccurately(38), also another study conducted among 221 female students, found that only 19.0% of them were performing BSE(39).BSE considered as one of the most important public health strategies in the early detection of BC. Young females should be informed about the BSE, which is one the most important steps in adopting the protective health attitudes, and changing negative behaviors to be positive. Educating this age group for learning and practicing BSE is important in order to make them aware about the BC, which is a rapidly increasing disease in recent years, and help them to gain health improvement attitudes (40,41, &42). In the present study training program improve students' knowledge and attitude towards BC and BSE. This result similar as another studies reported that there was statistically significant improvement in knowledge and perception about BC among study participants after intervention (43). The current study intervention involved training of students how to perform BSE correct technique, our results revealed improvement in BSE practice post intervention. Similar as finding of previous study reported that intervention program significantly increased both BSE frequency and accuracy among experimental group(44). There was a positive correlation between knowledge, practice and attitude post- program implementation among our study participants, this result reflected that increasing students' knowledge about BC, by providing them with awareness programs will contribute to improve their BSE practice, this result supported by another study found that women who were informed about BC were more likely to practice BSE (45). There is an evidence that most of early breast tumors are self-discovered and that the majority of early self-discoveries are by BSE performers (46). The current study discover 5% of participating students have breast problems after BSE well trained, and was referred to CBE.
 | Figure (1). Participants’ Knowledge towards breast cancer risk factors |
 | Figure (2). Participants’ barriers towards BSE practice |
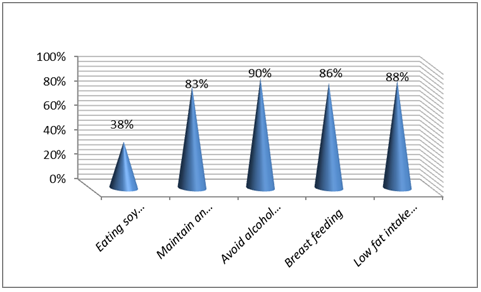 | Figure (3). Participants’ Knowledge regarding breast cancer precautions |
 | Figure (4). Participants’ source of information about BSE |
5. Conclusions
- Generally, there is poor knowledge, limited practice and negative attitude regarding breast cancer and breast self-examination among study participants. The implementation of educational training program resulting in positive improvement in students' knowledge, attitude and practice and help in discover breast problem cases. More efforts must be focused in provide educational programs, reassurance and counseling our young females about breast cancer screening and early detection, also posters and pamphlets in the university campus should be developed to increase heath awareness.
ACKNOWLEDGMENTS
- We grateful to all those who contribute & helped during data collection & applied educational program. Our special thanks to the Dean of KKU of research for financial support this research to conducting.