-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2013; 3(2): 9-17
doi:10.5923/j.phr.20130302.01
Determinants of High Fertility Status among Married Women in Gilgel Gibe Field Research Center of Jimma University, Oromia, Ethiopia: A Case Control Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDube Jara1, Tariku Dejene2, Mohammed Taha2
1Debre Markos University, college of Medicine and Health science Department of Public Health
2Jimma University, college of Public Health and medical sciences Department of Epidemiology
Correspondence to: Dube Jara, Debre Markos University, college of Medicine and Health science Department of Public Health.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Ethiopia is one of the countries with high and uncontrolled fertility in Africa. The TFR is 4.8 children per woman and under five mortality rates 88 per 1000 live births. This study was designed to identify determinants of high fertility status among Married woman Gilgel Gibe Field Research Center of Jimma University. Unmatched case-control study was conducted. Cases are women with number of children ever born alive greater or equal to five and controls are women with number of children ever born alive less than five. Simple random sampling technique was used. Logistic regression was used to analyze the data by using backward variable selection technique. In this study, age at last birth affect fertility status significantly with adjusted OR of 25.65. Under-five mortality affected fertility status significantly AOR of 1.91. Monthly family income, Age at first marriage, history of stillbirth experience and number of children desired before marriage were the other variables that showed significant associations with the level of fertility. The finding implies high fertility status is strongly associated with age at last birth, child death and some other factors like stillbirth. Hence measures that reduce child mortality and stillbirth are believed to decrease fertility status besides promoting child survival.
Keywords: Fertility Status, Under Five Mortality, Child Ever Born
Cite this paper: Dube Jara, Tariku Dejene, Mohammed Taha, Determinants of High Fertility Status among Married Women in Gilgel Gibe Field Research Center of Jimma University, Oromia, Ethiopia: A Case Control Study, Public Health Research, Vol. 3 No. 2, 2013, pp. 9-17. doi: 10.5923/j.phr.20130302.01.
Article Outline
1. Introduction
- The demographic pattern of developing countries is characterized by the co-existence of high fertility and high infant, and child mortality[1]. Fertility is the most important component of population dynamics and plays a major role in changing the size and structure of the population of a given area over time[2]. In 2008, of the 1.4 billion women in the developing world of reproductive age (15-49 years), more than 570 women die per 100,000 live births and 70 percent of this die due to totally avoidable reasons[3]. These women live in countries where their status is poor to extremely poor and these conditions threaten their health in many ways. Studies conducted in a number of countries show that wherever fertility is high, maternal, and infant and child mortality rates are high. Fetal deaths, low birth weight, and related problems are also associated with unregulated fertility. Fertility rate is highest in sub-Saharan Africa than many parts of the world, mainly due to strong kinship networks and high economic and social values attached to children[4].Ethiopia is one of the sub-Saharan African countries where high and persistent fertility rate has been seen for a long period of time. Although a slight decreasing trend has shown from year to year, it is still high as compared to developed nations[5]. Uncontrolled fertility has adversely influenced the socio-economic, demographic and environmental development of the country[6].Various reasons were mentioned for the reasons that kept the fertility rates still high in Ethiopia. Poverty, war and famine, low level of education, economic status and less autonomy of women and traditional barriers were usually mentioned as a reason for this persistent and high fertility rate in Ethiopia[5].The demographic significance of Ethiopian population growth on the African continent is substantial. The country is one of the largest and poorest that even in the midst of crisis, have maintained high levels of fertility[7]. Its population has increased nearly sevenfold from 11.8 million at the beginning of the 20th century to about 73.9 million in 2007. The estimated annual rate of growth and doubling period was 2.6% and 26 years, respectively[8].The Oromia Regional State where the present study was undertaken also is not out of this. The high plateaus of the region have been tremendously affected by uncontrolled population growth throughout ages. The potential health service coverage and utilization of the region is about 70.5% and 27%, respectively. Around 3.7% of women deliver at health care facilities, while over 95% of them deliver at home. The infant, and under-five mortality rate is 76 and 122 per 1000 live births respectively[9, 10]. According to the report of 2011 Ethiopia Demographic and Health Survey (EDHS), the total fertility rate and contraceptive prevalence rate of the region were 5.2 and 13.6 %, respectively[11].The women in Ethiopia were found to be at a disadvantaged position compared with the male counterparts mainly due to their low social status that results from a lack of access to family resources, education, occupation and decision-making power[12]. The women in Gilgel Gibe Field Research Center (GGFRC) where the present study will be undertaken as part of the country are not an exception.Human fertility is a function of a variety of factors. They are broadly classified into proximate (direct) and distal (indirect) factors. The proximal factors are bio-behavioural factors known to be the intermediate determinants are the biological, reproductive and behavioural/attitude factors through which the indirect determinants must devour to affect fertility and affect fertility directly, while the later, distal determinants are socio-cultural factors which consists of socio-economic and demographic factors affect fertility indirectly through affecting the bio-behavioural factors[1, 2].A proper understanding of these factors are of paramount importance in tackling the problem of uncontrolled fertility, which paves the way for the improvement of the prevailing socioeconomic problems of the country. Particularly, it would have a substantial contribution in the improvement of the health status of women and children. It is plausible that they may be related to each other. Therefore, the ultimate objective of the study was to assess the factors that influence high fertility status among married women in Gilgel Gibe Field Research Center of Jimma University, Oromia Region.
2. Method and Subjects
2.1. Study Setting and Design
- This study was conducted from January to February, 2012 at Gilgel Gibe Field Research Center of Jimma University. The Gilgel Gibe Field Research Center setting was identified by Jimma University considering South-West Ethiopia’s physical features, bio-social factors and the newly built dam as a field research and learning setting for Community Based Education (CBE). It is located in Jimma Zone of the Oromia Region about 260km south west of Addis Ababa and about 55 km north-east of Jimma. The total estimated population of these Kebeles is close to 50,000 residing in about 10,500 households[13].The study design was a community based unmatched case-control where cases are women with 5 or greater number of children ever born alive (CEB) and controls are women with less than 5 numbers of children ever born alive (CEB). The cut-off point of 5 is taken because the medical and obstetric risk for mothers with a number of CEB greater or equal to 5 is significantly higher compared with those with less than 5[1]. It is also based on the population policy of Ethiopia which aims to have less than five children per woman by the end of 2015[14]. The study subjects were selected from the Gilgel Gibe Field Research Center database. Total number of women who are married and aged 20 to 49 years of both cases and controls were identified from Gilgel Gibe Field Research Center database. Then the study subjects were selected by using simple random sampling technique from a list of case and control. The age range was restricted as fertility status was affected by age. All women aged 20-49 and who are married for at least 5 years were included in the study. These groups of women were taken for this particular study by taking into account the fact that women in Oromia region are married at an early age and could have more than four children before they celebrate their twenty-fifth birthday[15]. The minimum age was therefore set at 20 to give an equal chance for both the high and low fertile groups.As the investigation was unmatched case-control study, sample size was calculated by taking into account the major determinant. In this regard, a minimum detectable OR (Odds Ratio) of 2 for under five mortality among cases as compared to controls, a 5% level of significance (two-sided), a power of 80% and a two to one allocation ratio of controls to cases (2:1) were assumed.. The prevalence of important factors to be studied, which is the proportion of married women who have an experience of under-five mortality among the low fertile group, is assumed 29.7%[1]. This exposure variable was selected for sample size calculation because recent evidence show that improved child survival is the most powerful stimulant of fertility decline and hence under-five mortality is the most powerful determinant of fertility status[16]. Based on the above assumptions, with an additional 5 percent contingency for non-response the total sample size was 360 with 120 for cases and 240 for controls.
2.2. Measurement
- Structured interviewer administered questionnaire was used which was adopted from Ethiopian Demographic Health Survey (EDHS) and World Fertility Survey (WFS) to enable the comparability of the finding. Pre-test was carried out in one nearby kebele on 36married women of similar age group to familiarize the interviewers with the instrument.The number of children ever born (CEB) alive which is categorized as low fertility when CEB alive is less than 5 and high fertility when CEB alive is greater than or equal to 5 was the outcome variable. Independent variables include socio-economic and demographic, reproductive, biological, sexual behaviour, and under-five mortality.
2.3. Data Collection and Analysis
- Eight data collectors and two supervisors were recruited who were employees of the Research Center having prior training and experience on data collection. Training was given to the data collectors about the objective of the study and they were familiarized with the tool of data collection for two days. Data was collected from February 1 to 15, 2012. Incomplete questionnaires were filled by call back & the principal investigator supervised the overall activities on a daily basis. Each and every completed questionnaire was checked for completeness. Moreover, visiting randomly selected 5% of households were made each day to ensure the reliability of the collected data. Data was entered using Epidata version 3.1 with double entry to minimize data entry error.The data entered was exported to Statistical Package for Social Sciences (SPSS) version 16 for analysis. Logistic regression was fit to the data to identify factors that affect high fertility status as the main statistical method of analysis by using backward logistic regression variable selection technique. All explanatory variables that were associated with the outcome variable in bi-variate analysis with p-value of 0.25 or less were included in the initial logistic models of multivariable analysis. The crude and adjusted odds ratios together with their corresponding 95% confidence intervals were computed. A P-value ≤ 0.05 was considered to declare a result as statistically significant in this study. Ethical clearance was obtained from College of Public Health and Medical Sciences of Jimma University. Prior permission was also obtained from the program managers of Gilgel Gibe Field Research Center. Study subjects were told about the purpose of the study and verbal informed consent was secured. In order to protect the confidentiality of the information, names and house numbers was not recorded on the interviewer-administered questionnaire.
3. Results
3.1. Socio-Demographic and Economic Characteristics of Respondents
- A total of 120 women in the cases and 240 women in controls were included in this study of which 117 cases and 237 controls were willing to participate with overall response rate of 98.3%. This study indicated that among total respondents of cases and controls 103(88%) and 178(75%), respectively, cannot read and write while 14(12%) of cases and 59(25%) of controls can read and write or had attended formal education. Concerning educational status of their husbands, 80(68%) of cases and 147(62%) controls had husbands that cannot read and write whereas 22(19%) of cases and 21(9%) of controls had partners with informal education. On the other hand, 15(13%) of cases and 69(29%) of controls had partners with formal education. Of total respondents of cases and controls, 102(87%) and 183(77%), respectively, were residing in rural area. Many of the respondents, both cases and controls, were living in households with a very low monthly income. Regarding income source, the major sources of income were farming and livestock production for the majority of high fertile groups and low fertile groups.The mean number of children ever born (CEB) alive for older women (age 40-49 years) who are nearing the end of their reproductive period to be 7.26 from parity of 1 to 12 because the mean number of children ever born to older women, who are nearing the end of their reproductive period, is an indicator of average completed fertility. The TFR and the mean number of children ever born for women age 40-49 years would be expected to be similar. It was learned from the present study that the mean number of children per woman in the high fertile group was 6.0 (±2.0SD) while it was 3.0 (±1.0SD) in the low fertile group. The median age at first sex and marriage was 17.0 and 17.0 for both high fertile group and low fertile group, respectively. This study has shown that the median age at first birth was 19.0 for both high fertile group and low fertile groups, and the median age at last birth among high fertile group was 32.0 while it was 25.0 among low fertile group. Meanwhile, the mean duration of marriage among high fertile group was 18.0(median = 18.0) while it was 10.0 (median = 9.0) among low fertile groups.
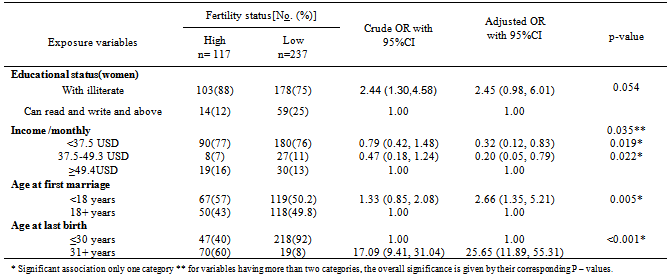
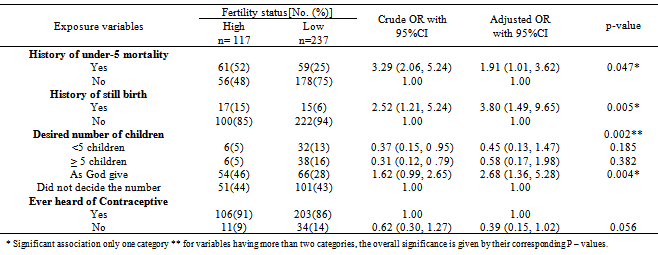
3.2. Determinants of High Fertility Status
- As can be noted from the result in table 2, educational status of women and their husbands, age at first marriage and age at last birth were significantly associated with outcome variable. Age at first sex, which has a high correlation with age at first marriage with correlation coefficients of 0.99, was removed from model as redundancy variables despite its association with fertility status. History of under five deaths, still birth experience, desired number of children, ever heard of contraceptive had a sizeable association with outcome variable (Table 3).In the final model, it was observed that ever heard of Contraceptive and Educational status of women were observed of having effects on fertility status and these factors were kept in the multivariable analysis based on the existing fact. The educational status of women and knowledge about contraceptives turned out to be marginally significant p=0.054 and 0.056 in multivariable analysis, respectively. Based on the existing fact that indicated educational status of women is considered to be an important controlling variable of fertility status. Thus taking into considerations of subject matter and based on the existing fact ever heard of contraceptive and educational status of women were included in the model (Table 2&3).
|
|
4. Discussion
- The high-fertility countries lag in many development indicators, as reflected for example in their rate of progress toward achievement of the Millennium Development Goals (MDGs). These countries have also received less development assistance for population and reproductive health than countries more advanced in their transitions to lower fertility[16].In order to successfully tackle the uncontrolled population growth and associated problems inEthiopia in general and in the present study area in particular, there appears a need to investigate the contribution of a number of factors influencing high fertility. Accordingly, this study has tried to look into determinants of fertility status in the study area by incorporating as many risk factors as possible. According to international standards, the median age at marriage for those married women age 20-49 years of 17.0 in Gilgel Gibe Field Research center. This is earlier than that of the legal age at first marriage in Ethiopia which is 18 years. However, compared to Ethiopia as whole, women in Gilgel Gibe Field Research center tend to get married at slightly similar ages. The median age at first marriage for women age 20-49 years of Ethiopia is 17.1, respectively[9, 11]. The educational status of women has shown insignificant effect on the fertility status of women in multivariable model even though it was turned out to be marginally significant. A similar finding was also reported in Rural Butajira where education of the mother didn’t show statistically significant difference among the low and high fertile group when adjusted for socio-demographic variables[17]. On the contrary, another study showed that uneducated Ethiopian women have three times as many children as their educated counterparts with at least secondary education. Those educated women have lower fertility compared to uneducated women[2, 11]. Educated women are more likely to postpone marriage, have smaller families more often than uneducated women[18]. As this study shown that majority of the women were uneducated and attended only primary level education which requires the development of an enabling condition to increase female student’s participation in school attendance and to reduce those who fail to continue their education. It is to be noted that education is instrumental not only to reduce uncontrolled fertility, but also to enhance many other developmental activities[19].Monthly income of the family was shown a significant association on fertility status of women in the study area similar to fact in the EDHS of 2011 in which Fertility status has also strongly associated with wealth quintiles[9]. Women residing in a family monthly income above 49.3 USD were 3.14 and 5.13 times more likely to have a high fertility status as compared to those women from the family had monthly income less than 37.5 USD and 37.5 USD to 49.3 USD respectively. But the reverse is true from the fact that in the EDHS of 2011 while Women in the lowest wealth quintile have a TFR of 6.0, more than twice as high as women in the highest wealth quintile, at 2.8[9] and also reverse from study conducted on the effect of Education, income, and Child Mortality on Fertility in South Africa in which the lower the income levels the higher the child mortality. Higher child mortality is followed by a higher fertility in individuals[20]. The possible explanation for this traditionally in rural setting people tend to have more children as their income and asset increase special agrarians society believe that children help them in farming and rearing their livestock.Age at first birth didn’t show significant effect on the fertility status of women both in univariate and multivariable analysis in this study. This is slightly different from results of other study while those women who get married at early age exposed to an early sexual intercourse and early first give birth, which in turn leads to too many teenage pregnancies. A study undertaken in Ethiopia revealed a situation in which mothers with an earlier age at first birth are likely to end up in having many children[21]. The possible explanation for this might be in this study there was no such a great variation in age at first birth for both high fertile and low fertile group. And age at first birth for both groups (high and low fertile women) was relatively the same with the median age at first birth was 19.0 for both high fertile group and low fertile groups.Age at first marriage did show a significant effect of on the fertility status of women. This effect is persisted after controlling the confounding factors. This is similar to other findings where age at first marriage highly a significant effect on fertility[19]. Similar results are documented in Nepal, Egypt and Morocco. The earlier age at marriage exposes to an early first intercourse with a consequence to earlier age at first birth. Study conducted on adolescent fertility show that teenagers whose age was between 18 and 19 years were about eight times more likely to be fertile than the younger once[1,21]. In this study area, marriage is acceptable culture of nearly all people. However, age at first marriage has an important factor to control age at first birth. Since early marriage has a major effect of early child bearing, they tend to have a lower rate of contraceptive use due to their inadequate know how of birth control. Women who marry early have on average a longer period of exposure to pregnancy and a greater number of lifetime births.The history of under-five mortality was found to have an association with fertility status of women. As the number of under-five children who had died increased, there appeared in increasing trend in the number of children ever born alive. Where similar result indicated that high infant and under-five mortality causes high fertility through the insurance and replacement effect[22, 23]. Study on analysis of data from rural Ethiopia supports under-five mortality had a strong significant effect on the number of children ever born. An increase in the number of children who have died raises the probability of attaining higher fertility[1]. Similarly the relation between fertility and child mortality experienced by mothers was found to be very strong and positive, in which it illustrated that under-five mortality, had a significant positive effect on fertility status. That is, an increase in the under-five mortality rate increases fertility significantly. As the number of children who died increased, women were exposed to a higher risk of uncontrolled fertility[24].Reducing under-five mortality, beside from giving mothers and fathers limit number of children they would like to have, will also increase the life expectancies of women to a greater extent. Moreover, women will have the opportunity to be occupied in many other activities that would eventually lead them to gain a greater empowerment. A similar finding was obtained in the South and North Gonder[25]. In India, the fear of under-five mortality and their own experience of the child /infant death tend to be increased the size of family, which the mothers considered to be replace the lost child. The death of an infant in an index birth interval and the death of a child immediately prior to the index interval elevate subsequent fertility[26]. High rate of under-five mortality is a contributing factor to a couple’s decision to have more children.History of still birth experience among the married women in this study was found to have an association with fertility status of women which contrary to other finding was obtained in the Butajira study of Central Ethiopia and Awassa whereas the occurrence of stillbirth didn't contribute for significant difference among the low and high fertility profile group[1, 2].The number of children desired before marriage indicated a significant association in the fertility status of women. This is similar to other studies where the desire to have lower children usually come firsts for decline in fertility[24]. This finding is in contrary to other similar studies in Butajira while the number of children desired before marriage did not show significant difference among the two-fertility profile group[1, 17]. The insignificant association seen in butajira might be due to the fact that the study was done in old age (30-49 years) women were desire more child is relatively more common and also difficult to remember desired children before marriage at this age group (recall bias). This study was conducted on both young age group and old age group respondents aged 20-49 which make this study different from study that conducted in Butajira.Knowledge about contraception assessed by asking whether the women ever heard of contraceptive didn’t show significant difference between the low and high fertility group this could be due to more than 85% of respondents have heard of contraceptive. Therefore, there was no such strong evidence at 5% level of significance to reject the null hypothesis of no significant association between ever heard of contraceptive and fertility status of women because there was no such a great variation in ever heard of contraceptive. It is analogous results were documented in Butajira and Awassa where knowledge about contraception whether the woman knows the existence of contraceptives didn’t show significant difference between the low and high fertility group[2, 17].Ever use of contraceptives was not found to have a significant effect on fertility status of women. There was no such strong evidence at 5% level of significance to reject the null hypothesis of no significant association between ever use of contraceptive and fertility status of women again because there was no such a great variation in using contraceptive. As it can noted from the study result both groups (high and low fertile women) were about the relatively the same in using contraceptives (20% vs. 27%). Similar findings were documented in the Gondar studies that both groups (high and low fertile women) were about the same in using contraceptives (22% vs. 25%)[25]. It could be due to women intended to use contraception when they reach or exceed the total number of children ever born alive they would like to have. More than 80% of respondent were living in rural area and poor educational status (even lower than elementary education class) which could be directly or indirectly affect their contraceptive use. Similar findings were found from Awassa, Bangladesh and Ghana while Ever use and current use of contraceptives is not significantly associated with the fertility status of women[2, 26, 27]. Other Similar findings were documented in the Gondar and Butajira[1, 24]. In contrary studies where the use of contraception is significantly higher like Pakistan where contraceptive use was found to be directly associated with the fertility desire and fertility status and the fertility inhibiting effect of contraception has been demonstrated by several studies in developing countries was significant[28,29,30]. Some of the events may be difficult to remember and hence the effect of recall bias may exist. Selection bias might introduce due to incompleteness of database concerning variable of interest for selection.In concussions, various reasons were mentioned as reasons that kept the fertility rates still high in Ethiopia. In GGFRC, the number of children ever born alive is high. This study has tried to come up with the conclusion; the following factors are contributed to this experience of high fertility. These factors are: - family monthly income, under-five mortality and stillbirth, age at first marriage, age at last birth and desired number of children before marriage were the most contributing factors. Among these factors, under-five mortality and stillbirth as well as age at last birth considerably stand as controlling predictors of fertility. More than half of the respondents approved the benefits of having more children and their main reasons for such need were children support in old age, to maintain posterity; children's are honour and uncertainty of children survival. Based on the findings of the study, the following recommendations are made:◆ Measures taken to decrease under-five mortality and stillbirth will indirectly help in reducing fertility. Such strong measures can be vaccination, impregnated bed nets (ITN), access and provision of safe water, reducing maternal infection etc should be put in place to reduce fertility. Incorporating the basic disease prevention methods in primary schools could also be considered. All stakeholders including health extension workers should exert maximum efforts should be trained to practice those mothers, the key child survival interventions like antenatal care follow-up, skilled-based delivery, use of oral rehydration salt and homemade fluids.◆ In Ethiopia in general and in the present study areas in particular, marriage is the destiny of nearly all people. The legal age at first marriage in Ethiopia is 18 years. However, this minimum age at first marriage is not implemented particularly in the present study areas. Hence, all responsible bodies including the remotest Kebele administrations, community, community leader and religious’ leaders should be in a position to ensure the practicability of this marriage law. ◆ It was understood from the present study that there was some evidence regarding the negative influence of current use of contraceptives on high fertility. In this regard, the family planning programs of the region should be strengthened to the extent that they could play significant roles in bringing down the prevailing high fertility. Accordingly, the main stakeholders including health extension workers should exert maximum efforts to make the method of choice available and accessible to the users.◆ Thus community conversation should include education department, women affair, health extension workers and social ritual groups giving emphasis on couple’s knowledge, approval and use to family planning to reduce fertility. Low fertility women’s should encourage about small desired children.
Competing Interests
- The authors declare that they have no competing interests.
ACKNOWLEDGEMENTS
- Jimma University College of Public Health And Medical Sciences Department of Epidemiology is duly acknowledged for giving me this golden and educative opportunity. My deepest gratitude goes to Gilgel Gibe Field Research Center program managers Mr. Fasil Tesema and all other staff member for their cooperation in providing me appropriate information from their database and unforgettable support during data collection period. I want also to acknowledge the data collectors, the supervisor and the participants for their genuine dedication and participation during the data collection. At last, but not least, I would like to express my sincerely thanks to my colleagues MPH students and all those who in one way or another have contributed to my success in conducting this study.
Appendix 1: Conceptual Framework on Determinants of High Fertility Status
- The conceptual framework of the study that deals with the determinants of high fertility status is showed in figure1. The selected socio-economic and demographic factors in the model list the proximate determinant variables. These factors can also determine high fertility of married women. This conceptual framework is constructed based on the peer reviewed published literatures.
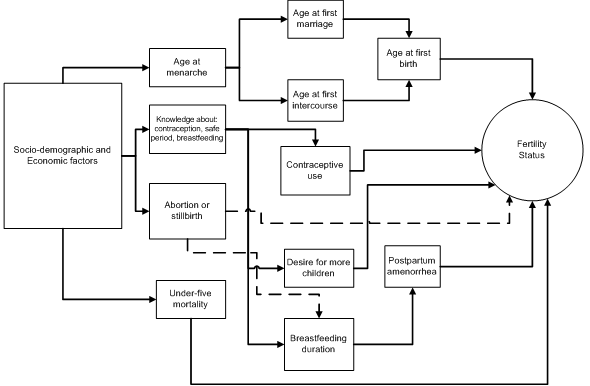 | Figure 1. Conceptual framework on determinants of high fertility status in Gilgel Gibe Field Researcher Center, 2012[31] |
Appendix 2: Schematic Presentation of Sampling Technique
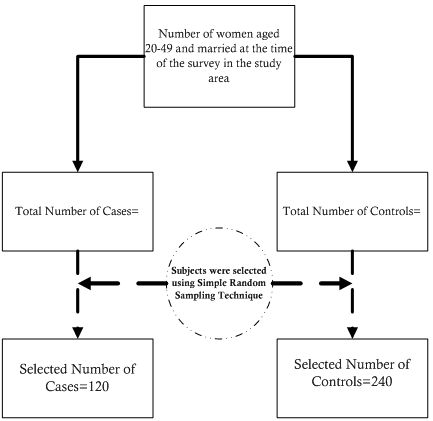 | Figure 2. Schematic presentation of sampling technique of married women in Gilgel Gibe Field Researcher Center, 2012 |
References
| [1] | Yohannes F., Yimane B., Alemayehu W. Impact of Child Mortality and Fertility on Fertility Status in Rural Ethiopia. East Africa Medical Journal, 2004.81(6): 301- 305. |
| [2] | Samson Gebremedhin and Mulugeta Betre, Level and Differentials of Fertility in Awassa Town,Southern Ethiopia,2009: Afr J Reprod Health 13(1):93-112. |
| [3] | World Bank .The World Bank’s Reproductive Health Action Plan 2010-2015 ,April 2010 |
| [4] | Hinde and Mturi. Fertility levels, a trend and differential in sub-Saharan Africa in the 1980's and 1990's. Studies Family Planning. 2001, 26:1-25. |
| [5] | T.Tewodros. Cross Sectional Study of Women Employment and Fertility in Ethiopia, 2011; 1-63. |
| [6] | Ezra M. Demographic responses to environmental stress in drought and famine prone areas of Northern Ethiopia. Int J popul Geogr, 2001; 7:259-279. |
| [7] | Short SE, Kiros GE Husbands, wives, sons, and daughters: Fertility preferences and the demand for contraception in Ethiopia. Population Research and Policy Review, 2002; 21: 377- 402. |
| [8] | Planning and Programming Department, Ministry of Health of Ethiopia. Health and health related indicators Addis Ababa, 2007. |
| [9] | Aynalem Adugna.http://www.ethiodemographyandhealth.or.html Data Aug 1-2010; 1-35.9 |
| [10] | WHO Emergency Humanitarian Action (EHA), Ethiopia Programme, Report on Field Trip to Provide Technical Support in Emergency Preparedness and Response to Oromiya Regional State 2007.10 |
| [11] | Central Statistical Agency, ORC Macro. Ethiopia 2011 Demographic and Heath Survey. Preliminary report. Addis Ababa, Ethiopia; Calverton, Maryland 2011. |
| [12] | FAO, The challenge of the HIV/AIDS epidemic in Rural Ethiopia: averting the crisis in low AIDS –impact communities finding from fieldwork in kersa woreda, Eastern Hararghe Zone, Oromiya Region. Clare Bishop-Sambrook Sustainable Development Department, FAO, Rome.2004.12 |
| [13] | Deribew, A., Alemseged, F., Birhanu, Z., Sena, L., Tegegn, A., Zeynudin, A., Dejene, T., Sudhakar, M., Abdo, N. and Tessema, F. Effect of training on the use of long-lasting insecticide-treated bed nets on the burden of malaria among vulnerable groups, south-west Ethiopia, 2010: baseline results of a cluster randomized trial. |
| [14] | The transitional government of Ethiopia, Office of the Prime Minister, National population policy of Ethiopia Addis Ababa, 1993. |
| [15] | Central Statistical Agency, ORC Macro. Ethiopia 2005 Demographic and Heath Survey. Addis Ababa, Ethiopia; Calverton, Maryland 2006. |
| [16] | Chowdhury S. Determinants and Consequences of High Fertility: A Synopsis of the Evidence, June 2010; 1-30. |
| [17] | Yohannes F., Yimane B., Alemayehu W., Differentials of fertility in rural Butajira. Ethiop J Health Dev, 2003; 17(1):17-25. |
| [18] | Derebssa Dufera Serbessa, Differential Impact of Women’s Educational Level on Fertility in Africa: The Case of Ethiopia, 2002;Cice p1- 17 |
| [19] | Boupha, S., Souksavanth, P., Chanthalanouvong, T.,Phengxay, S., Lao Reproductive Health Survey,2005. |
| [20] | Dust, K., The effect of Education, income, and Child Mortality on Fertility in South Africa. Master of art thesis presented to the school of graduate studies of Simon Fraser University, 2005;pag 22-28 |
| [21] | Tewodros A., Jemal H., Dereje H., Determinants of adolescent fertility in Ethiopia. Ethiop.J. Health Dev,2010;24(1):30-38. |
| [22] | Bamikale j. F.and Akinrinola B. Fertility Transition in Nigeria: Trends and Prospect, 2000; 506-528. |
| [23] | Gyimah,S. Obeng.,Childhood mortality and reproductive behavior in Ghana and Kenya :an examination of fertility and non-fratility models .Ph.D dissertation ,Faculty of Graduate studies ,the University of Wasteren Ontario, London ,Canada,2002. |
| [24] | Ramesh Adhikari, Demographic, socio-economic, and cultural factors affecting fertility differentials in Nepal, BMC Pregnancy and Childbirth 2010; 10:19. |
| [25] | Getu Degu and Alemayehu Worku, Differentials of fertility in North and South Gondar zones, northwest Ethiopia: A comparative cross-sectional study. BMC Public Health, 2008; 8:397. |
| [26] | Hossain, M. B., Phillips, J. F., LeGrand, T.K., The impact of Childhood Mortality on Fertility in Six Rural Thanas of Bangladesh. Population Council. One Dag Hammarskjold Plaza, New York, New York 10017 USA, 2005. |
| [27] | Kwame Boadu, The Effect of Contraceptive Practice on Fertility in Ghana: A Decade of Experience Canadian Studies in Population, 2002;Vol. 29(2): pp 265-291 |
| [28] | Azhar Saleem and G. R. Pasha, Modeling of the women’s reproductive behavior and Predicted Probabilities of Contraceptive Use in Pakistan, 2008;page 1-15 |
| [29] | Feyisetan, B. B, & Casterline, J. B., Fertility preferences and contraceptive change in developing countries. International family planning perspectives, 2000; 26 (3), 100-109. |
| [30] | Sajid, A.and M.M. Franklin White, Family planning practices among currently married women in Khairpur district, Sindh, Pakistan. JCPSP, 2005; 15(7):422 425. |
| [31] | Shapiro, D. Women’s Education and Fertility Transition in Sub-Saharan Africa, 2011; 1-32. |