-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2012; 2(5): 136-142
doi: 10.5923/j.phr.20120205.04
Knowledge, Perceptions and Practices on Antiretroviral Therapy in Farming Communities in Ghana: A Study of HIV Positive Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLDaniel Boateng 1, Dadson Awunyo-Vitor 2
1Department of Community Health, School of Medical Sciences, Kwame Nkrumah University of Science and Technology
2Department of Agricultural Economics, Agribusiness and Extension, Kwame Nkrumah University of Science and Technology, Kumasi-Ghana
Correspondence to: Dadson Awunyo-Vitor , Department of Agricultural Economics, Agribusiness and Extension, Kwame Nkrumah University of Science and Technology, Kumasi-Ghana.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
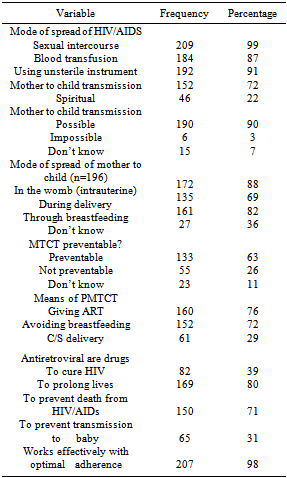
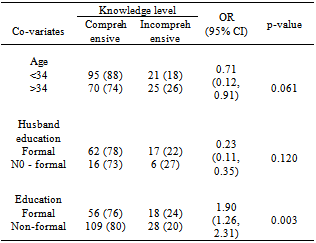
Low levels of knowledge of antiretroviral therapy (ART) and Prevention of Mother-To-Child-Transmission (MTCT) among persons living with HIV present an unwanted window for transmission within the general population. The purpose of this study is to assess the level of knowledge, attitudes and perceptions of HIV positive women on antiretroviral therapy (ART) and Prevention of Mother-To-Child-Transmission (MTCT). The study surveyed 211 HIV positive women from ART centres in two districts in Ashanti region of Ghana. Data was collected through interviews using structured questionnaires and focus group discussion using interview guides. Qualitative and quantitative techniques were used to analyze the data. The study revealed that about 15% of the women exhibited no knowledge about the possibility of transmission of HIV from mother to child whilst 36% had no knowledge on the mode of MTCT of HIV. Those who had knowledge of MTCT indicated that this could be intrauterine (88%), delivery (69%) and through breastfeeding (82 %).Mothers with incomprehensive knowledge on ART were 2.5 times more likely to default ART (OR=2.5, p=0.002). Comprehensive knowledge was positively influenced by high education level (OR=1.9; p=0.003). Social marketing campaigns should be developed and targeted at improving women literacy on their health issues and getting more women to test for HIV in order to incorporate them into PMTCT programmes. Further research however needs to be conducted to ascertain the facility and community based factors that influence the women’s knowledge on ART and PMTCT.
Keywords: HIV, Women, Knowledge, Perception, Ghana ART,PMTCT
Cite this paper: Daniel Boateng , Dadson Awunyo-Vitor , "Knowledge, Perceptions and Practices on Antiretroviral Therapy in Farming Communities in Ghana: A Study of HIV Positive Women", Public Health Research, Vol. 2 No. 5, 2012, pp. 136-142. doi: 10.5923/j.phr.20120205.04.
Article Outline
1. Introduction
- HIV/AIDS remain a major cause of death worldwide with the majority coming from sub-Saharan Africa. AIDS has killed more than 25 million people since 1981 and an estimated 33.2 million (31.4 million – 35.3 million) people are living with HIV/AIDS worldwide with 2.5 million of them from sub-Saharan Africa. In 2007, 2.1 million HIV related deaths were recorded with 1.6 million (76%) from Sub Saharan Africa[13]. In Ghana, HIV prevalence among adults in 2010 was 1.5%. An estimated 267,069 persons made up of 95,206 males and 126,735 females were living with HIV as at 2010 and the prevalence of HIV/AIDS among antenatal clients was 2.0%[14]. Prevalence of HIV among ANC women is therefore 0.5% higher than prevalence among adults population and the estimated number of pregnant women living with HIV in 2009 was 13,000. Currently, the Ashanti and Eastern regions are home to the greatest percentages of HIV positive people with prevalence of 3.2% and 3.0% respectively[15].The HIV epidemic is becoming increasingly feminized with nearly50% of people living with HIV being females globally as at 2010[20]. HIV remains the leading cause of death among women in reproductive age and HIV infection among children has mainly been through Mother-To-Child-Transmission (MTCT). However, the most effective way of preventing MTCT of HIV is to prevent infection in women of reproductive age. As of December 2009, HIV testing and counselling services were accessed by 53% of all pregnant women in Ghana, 74% of whom were tested for HIV and given their results. The HIV prevalence among those tested was 1.7% of which 55% received antiretroviral drugs to prevent vertical transmission. The comparative proportion of babies born to HIV infected women who received antiretroviral drugs for prophylaxis was 30%[8].The rapid incidence and fatality of HIV/AIDS globally with its greatest impact in sub-Saharan Africa has been a growing concern of world leaders and stakeholders in health to continuously seek a remedy to this canker. In the light of this, there have been International and national efforts to improve care and support for PLHIV, including HIV Testing and counselling (HTC) services, establishing ART centres and PMTCT services. Though awareness of HIV and AIDS have been high since 2003, where 98% of women and 99% of men were reportedly aware on HIV, comprehensive knowledge on HIV and AIDS, appropriate prevention and non-stigmatizing behaviour have been lagging behind[5]. As at 2007, 25.1% of young women and 33% of young men aged 15-24 years had comprehensive knowledge (i.e. correctly identified ways of transmitting HIV and rejected misconception about HIV transmission) of HIV and AIDS. In 2008, the Ghana Demographic and Health Survey (GDHS) showed that only 28.3% of female respondents age 15 – 24 and 34.2% of men had comprehensive knowledge about HIV and AIDS. There has thus been little progress along this front[8].Patient’s knowledge, attitudes and practices on HIV/AIDS, PMTCT and ARTs influence their motivation and uptake of ARVs for PMTCT. A good level of understanding about HIV by the patient, a belief that ART is effective and prolongs life, and recognition that poor adherence may result in viral resistance and treatment failure all impact favourably upon a patient’s ability to adhere. Conversely, a lack of interest in becoming knowledgeable about HIV and a belief that ART may in fact cause harm adversely affect adherence[18]. A study in Uganda to find out the barriers to accessing Highly Active Antiretroviral Therapy (HAART) by HIV positive women, found out that women who had not enrolled in the (Highly Active Antiretroviral therapy) HAART-Plus programme had a remarkably lower level of knowledge on HIV/AIDS and HAART compared with those who had enrolled in the programme[4]. Other studies in the continent also found mothers knowledge on PMTCT to be low[1],[7].Ones knowledge of HIV, ART and PMTCT is however influenced by interplay of socio economic and other cultural factors including clients’ educational level and marital status. A lower level of general education and poorer literacy may impact negatively on some patients’ ability to adhere, while a higher level of education has a positive impact[2]. The purpose of this study is to assess the level of knowledge, attitudes and perceptions of client’s on ART and PMTCT and determine the extent of influence of client’s knowledge level on accessing ART. Low levels of knowledge of HIV status among persons living with HIV present an unwanted window for transmission within the general population, in addition to sex with female sex workers, their clients, and non-paying partners[8].
2.Methodology
2.1. Study Design
- The study was a descriptive cross sectional design. The methods were both qualitative and quantitative and data was collected at the individual and facility level.
2.2. Study Area
- The study was conducted at the ART centres in two farming towns in the Ashanti Region, Ejura and Nyinahini. These are two farming dominated towns in theEjura-Sekyedumasi and AtwimaMponua districts respectively. The agriculture sector in the Ejura-Sekyedumase District dominates all the other sectors of the economy in terms of employment as a typical characteristic of a Ghanaian setting. It employs about 68.2% of the population which is above the national rate of 60%.With respect to HIV prevalence, the Ashanti Region recorded the second highest in the country in 2011 (3.0%). Routine HIV testing and counselling are offered during antenatal care visits for pregnant mothers at both ART centres.
2.3. Sampling and Sample Size
- The sample was selected in two (2) stages. Two ART centres were purposively selected from two farming communities in the Ashanti Region. These were the Nyinahin Hospital and the Ejura District Hospital. Systematic random sampling was used to select respondents for exit interviews and FGDs at the ART centre. Administrative records, which included the pharmacy refill register, medical consultation appointment visits, were also used to get information of respondents. A total of 211 respondents were involved in the study.
2.4. Data Collection and Tools
- The data collection technique for the quantitative method was interviews and the tool employed was structured questionnaires (open ended and closed). Qualitative data was obtained using semi-structured interviews, focus group discussions (FGDs) and interviews with key informants using tape recorders and interviews guides as data collection tools. Interviews and the FGD were carried out in quiet and discreet locations in a vacant room in the hospital’s outpatient department. The interviews were conducted and audio-taped in the local language. Tapes were transcribed verbatim in Twi and then back-translated into English. Spot checks of interview and FGD transcripts and translations were regularly conducted to ensure the completeness of the transcription and the accuracy of the translation. Questionnaires and interview guides were pre-tested to check for clarity, consistency and acceptability of the questions to respondents. Following this, the necessary corrections were made and questionnaires finalized for the actual field work.
2.5. Statistical Analysis
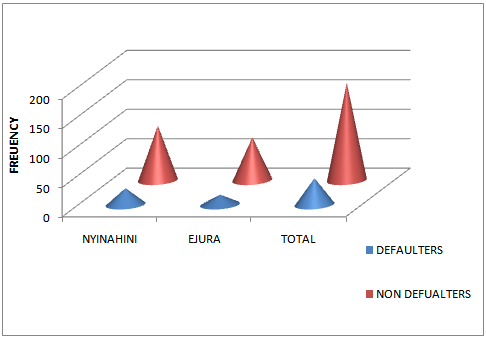
- All questionnaires and interview results from the field were checked for completeness and internal errors. Questionnaires were then sorted, numbered and kept in files labelled per facility from which the participants were interviewed. Responses on the various questions to test for knowledge were coded as yes, no or don’t know. General knowledge level was computed by respondents total correct responses from the various issues posed to test for knowledge. Respondents who accepted all correct responses were groups having “adequate knowledge” and vice versa. Bivariate associations and 95% confidence intervals were used to access the influence of certain socio demographic characteristics on the knowledge level of the women using STATA 11
2.6. Ethical Consideration
- Ethical clearance for the study was obtained from the Committee on Human Research, Publications and Ethics (CHPRE) of the Kwame Nkrumah University of Science and Technology (KNUST) and Komfo Anokye Teaching Hospital (KATH). The participant’s capacity to consent was considered. There was full disclosure or discussion of relevant information/ questions. Translators were used for participants who could not read.
3. Results and Discussion
3.1. Background Characteristics
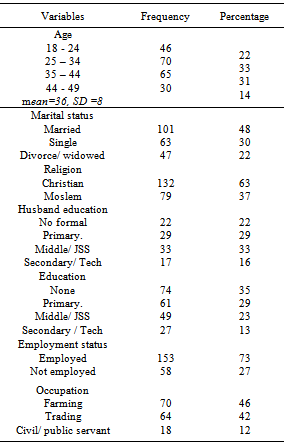
- The research was conducted using 211 HIV positive women from ART centres at Ejura and Nyinahini in the Ashanti Region. One hundred and twenty one of the respondents representing 57% are from Nyinahini, and 90 (43%) are from Ejura ART centre. More than 50% have been on treatment for less than 24 months with the maximum length on treatment being 156 months (figure 1). The mean and median length on treatment is 20 months and 21 months respectively. A regression analysis indicate a statistically significant association between one’s months of being on ART and regularity at ART (t =3.91, p=0.000). Majority of the women aged below 35 years (55%) and the mean age was 36 years (SD = 8). Majority of the women were married and 13% had schooled to the secondary level with 35% having no formal education. Seventy-three percent with farming being the most cited job. In general, the defaulter rate was 21%. This was inconsistent with estimates of average rates of adherence to ART in many different social and cultural settings which range from 50% to 70%[11],[16],[18].
|
3.2. ART Defaulting Rate
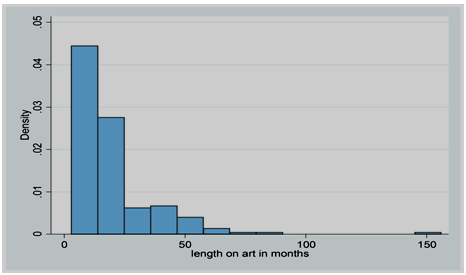
- As detailed in figure 2 the total defaulting rate among the women was 21% (45 out of 211 respondents). At Nyinahini, 28 out of the total of 121 had defaulted ART. Defaulting was higher among respondents from Nyinahini as compared to Ejura (23% vrs 19% respectively).
 | Figure 1. Number of months respondents are on ART |
 | Figure 2. ART defaulting rate |
 | Figure 3. summary of knowledge level on PMCT |
3.3. Knowledge on PMTCT
- Table 2 gives a summary of the responses of the women on their knowledge about MTCT. Seventy-two percent of them knew that HIV/AIDS could be transmitted through MTCT About 15% of the women exhibited no knowledge about the possibility of transmission of HIV from mother to the baby. The women who had knowledge of MTCT indicated that this could be intrauterine (88%), delivery (69%) and through breastfeeding (82%). Thirty-six percent however had no knowledge on the mode of MTCT of HIV.
|
|
4. Conclusions
- It is evident that respondents’ knowledge level plays an important role in their access to ART which supports the findings of[14]. Superstition with respect to the causes of HIV is still high among the respondents. This could be attributed to the fact that, education on HIV given to these women is not targeting misconceptions about the etiology of the disease. However, mothers’ educational level is a key determinant of their knowledge on HIV/AIDS, ART and PMTCT.Generally the respondents understand that is effective and prolongs life. In addition they are also aware that poor adherence may result in viral resistance. This conforms to the result of a study by[18]. Furthermore, majority of the respondents are aware that MTCT was possible and could be through Mother’s breast to the child during breast feeding process. Hence they are likely to accept any measures that would prevent this mode of transmission provided they can afford it and there is no stigma attached to it. The study revealed that counselling at the ART centre is very important in ensuring the respondent regularity at the ART centres to pick their medications[13].The facility and community based educational interventions should therefore be scaled up and should be designed to be acceptable to both the literate and illiterate in the society. This must also seek to demystify the scientific nature of the disease and clear all misconceptions and possible thoughts of spirituality in the etiology of the disease. Social marketing campaigns should also be developed and targeted at improving women literacy on their health issues and getting more women to test for HIV in order to incorporate them into PMTCT programmes. Further research however needs to be conducted to ascertain the facility and community based factors that influence the women’s knowledge on ART and PMTCT.
ACKNOWLEDGEMENTS
- The authors wish to recognize the support of Prof. E.A. Addy, Dept of Community Health, Kwame Nkrumah University of Science and Technology. We are also grateful to our research assistants for their assistance. Finally, we would like to appreciate the support of the management and staff at the ART centre at Ejura and Nyinahini as well as all participants for their cooperation and enthusiasm in this study.