-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
2012; 2(4): 106-109
doi: 10.5923/j.phr.20120204.07
Behavior Changesin Older PersonsCaused byUsing Wood Products in Assisted Living
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLAnme T. 1, Watanabe T. MA 1, Tokutake K. MA 1, Tomisaki E. MA 1, Mochizuki H. MA 1, Tanaka E. MA 1, Wu B. MA 1, Shinohara R. 1, Sugisawa Y. 1, Tada C. 2, Matsui T. 3, Asada S. 4
1Faculty of Medicine, University of Tsukuba, Ibaragi, Japan
2Tokyo Toy Museum, Tokyo, Japan
3Faculty of Wood, Gifu Academy of Forest Science and Culture, Gifu, Japan
4Faculty of Education, Saitama University, Saitama, Japan
Correspondence to: Anme T. , Faculty of Medicine, University of Tsukuba, Ibaragi, Japan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The purpose of this studywas to clarify the effects of using wood products in older persons’ environment by means of an intervention study. The participants were 44 older persons in a single assisted-living facility. Evaluators observed the participants’ behavior at 5 points: (1) not using any products (baseline), (2) using plastic tables and chairs, (3) using wood tables and chairs, (4) using wood tableware, (5) continually using wood products for 5 weeks. Health care professionals evaluated the older persons’ health status and activities of daily living through regular observation.The results indicated that regular use of wood products significantly increased the social interactionand activity levels of the elder. Thus, use of wood products may enhance the possibility of preventing mental and physical decline in the frail elderly.
Keywords: Interaction, Wood Products, Old Person, Evaluation, Scale
Article Outline
1. Introduction
- The effects of natural products, such as those made from wood, are of interest worldwide because people are aware that humans need an ecologically friendly, sustainable society. Previous research has explored the healing [1,2] and safety effects[3,4]of wood products. Few studies, however, have evaluated the actual change that the use of such products might make in the behavior of older persons in assisted living.The increasing number of older persons with dementia and societal maladjustment requires society to prepare appropriate living environments for those people. For decades, researchers, practitioners, and caregivers have been attracted to studyingthe prevention of a decline in social competence. Social competence is determined by complex interactionsbetweenpersons and their living environments, peer relationships, and the larger sociocultural environment[5]. It is defined as the ability to understand others in the context of social interaction and to engage in smooth communication with them. The factors comprising “social competence” have been a frequent topic of research worldwide for some decades, andsome common factors have emerged from the studies. Forexample, SSRS [8] identified three factors—namely,cooperation, self-control, and assertion. Caldarella [9] mentioned five factors—peer relations, compliance, self-management, assertion, and academic success—while Elksninand Elksnin[10] offer such aspects as interpersonal, teacher-pleasing, self-related communication, and assertiveness; Kolb [11] also defines five factors: peer and group interaction, problem solving/decision making, self-management, communication, and assertion. These lists have three factors in common: empathy/coordination with peers, self-regulation, and assertion.The social competence of adults has been evaluated with a number of scales that employ various factors: the Social Skills Inventory (SSI) [12] (the six factors are emotional expressivity, emotional sensitivity, emotional control, social expressivity, social sensitivity, social control); ENDCOREs [13] (self-control, expressivity, sensitivity, assertiveness, responsiveness and regulation); Adult Behavior Checklist for Ages 18-59 (ASEBA) [14,15] (adaptive functioning, empirically based syndromes, substance use, internalizing, externalizing, and total problems); and the Weinberger Adjustment Inventory (WAI) [16] (distress, anxiety, depression, low self-esteem, low well-being, self-restraint, suppression of aggression, impulse control, responsibility, and consideration of others).These factors involved in social competence, along with the scales for evaluating it, indicate clearly that social competence should be assessed by the interaction between persons and their social environment. Many researchers do focus on measuring the quality of living environments and care, based on the theory that living environment is significantly related to older persons’ health. However, methodologies that consider persons in conjunction with their social environment across developmental stages have not yet been well developed.Two instruments have been designed toevaluate persons’ living environment within their natural settings, as well as anindividual’s emotional and verbal responsiveness to otherpersons, and the acceptance of another person’s behavior. The Alzheimer’s Disease Related Quality of Life (ADRQL)[5,6] andthe Interaction Rating Scale Advanced (IRSA)[7] are often used in research related to social competence and quality of life for the frail elderly.The ADRQL and IRSAboth evaluate persons’ living environment within their natural settings, as well as a person’s emotional and verbal responsiveness to otherpersons, and the acceptance of another person’s behavior.Previous research has alluded to the positive effects of wood products:they are alleged to have a relaxing effect and to reduce fatigue through the chemical phytoncide [1]. In addition, visual comfort is attained because of wood’s ultraviolet absorptivity and its emotional harmony [2-4]. The purpose of this study is to clarify the effects of using wood products on older persons through an intervention study. It is meaningful for health professionals to know how a living environment with wood products influences older persons’ social interaction and quality of life.
2. Methods
2.1. Participants
- All of the participants in our study were ina single assisted living facility in the Shizuoka Prefecture, Japan. We excluded members who were severely demented or too disabled to move by themselves. Among the 47 residents of the facility, 44 participated the study. There were15 men and 29 women, ranging in age from 71 to 96 years.This study was approved by the ethics committee of the Art Education Council. In order to comply with ethical standards, signed informed consent forms were obtained from all participants at the beginning, and they were made aware that they had the right to withdraw from the experiment at anytime. To maintain the confidentiality of the personal information of the participants, a personal ID system was used to protect personal information. Further, all the image data were stored on a password-protected disk; only the researchers who were granted permission were given access to the data.
2.2. Measures
- TheADRQL[5,6]consists of 47 items grouped into 5 domains connected with the quality of life of the frail elderly as assessed by a caregiver or health care professional. These domains are social interaction, awareness of self, feelings and mood, enjoyment of activities, and response to surroundings. Each item is weightedby caregivers and experts according to the importance attached to it for quality of life. Item weights are summed to yield a score for each subscale, and these subscale scores are then summed to yield a total score.The IRSA[7]consists of 92 items grouped into 6 domains connected with social competence as assessed through 5-minute observations by evaluators,whohad acquired a reliability of over 90%consistency before the study. These domains are self-control, expressivity, sensitivity, assertiveness, responsiveness, and regulation.Each subscale assesses the presence of behaviors (1=Yes, 0=No), and the sum of all items in the subscale provides the overall behavior score.To avoid duplication, we used the items from only three of the domains of sensitivity—empathy, responsiveness to social engagement, and expressivity as self-expression.
2.3. Procedure
- The evaluators observed the participants’ behaviorin their everyday life at five points: (1) not using any products (baseline, Photo1);(2) using plastics tables and chairs (Photo2);(3) using wood tables and chairs(Photo3);(4) using wood tableware(Photo4);(5) continual use of wood products for five weeks. To score the behavior, two evaluators coded the participants’ observed behaviors. In addition, healthcare professionals evaluated older persons’ health status and activitiesofdaily living based on regular observation at the assisted living facility.
 | Photo 1. Baseline |
 | Photo 2. Plastic product use |
 | Photo 3. Wood productuse |
 | Photo 4. Wood tableware use |
3. Results
- Figure1 shows thechangesin elderly persons’ behavior score according with the stages indicated above, from(1) baseline through(5) continualuse of wood products for 5 weeks.The scores forResponse to surroundings, Empathy,and Self-expression, in addition to the total scores,were significantly increased after using wood products,as observable through the scores kept over5 weeks (Table1).
|
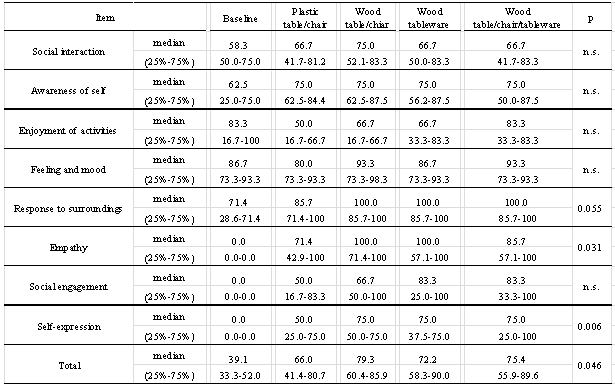
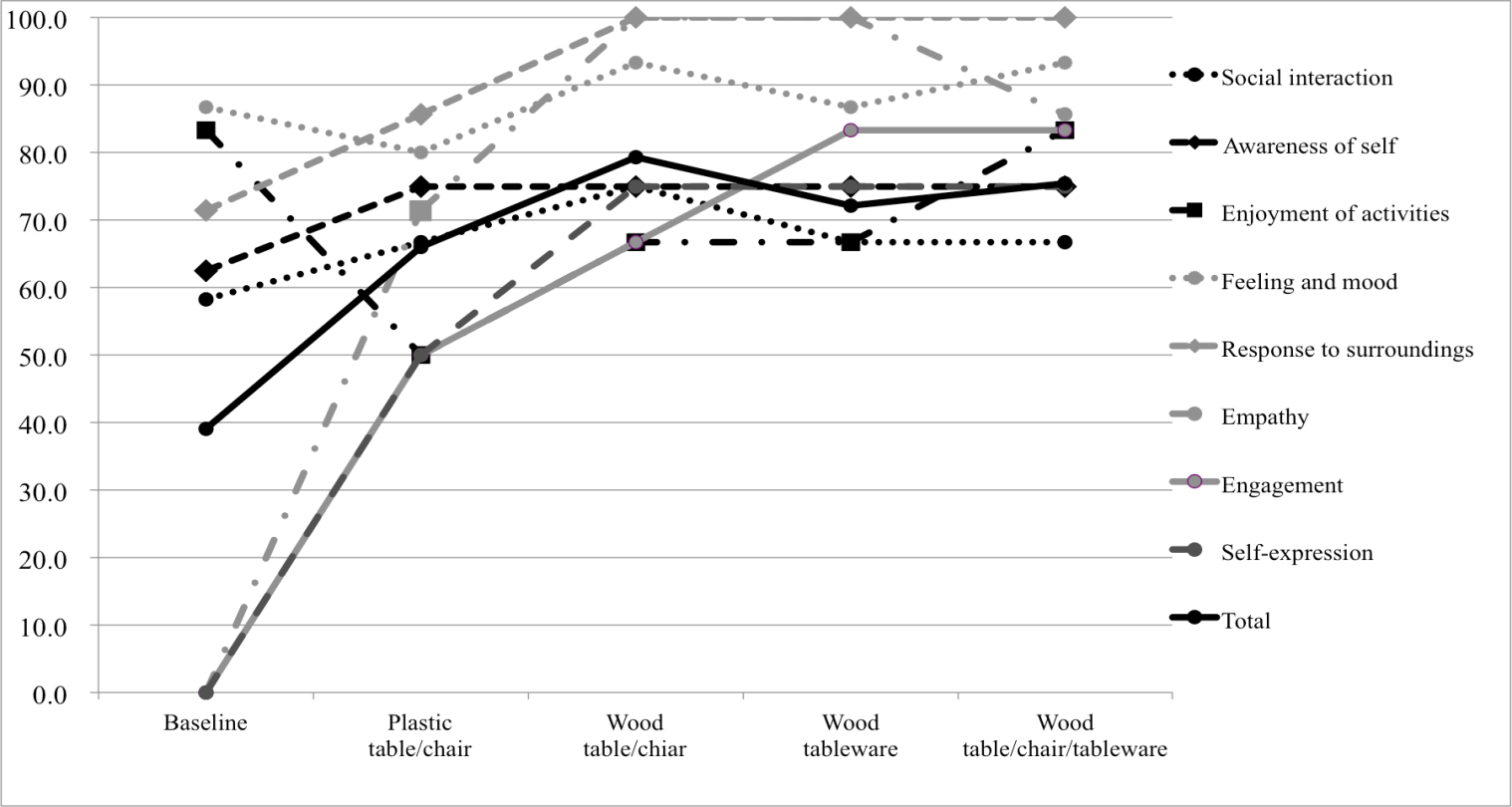 | Figure 1. Change in elderly persons’ behavior score |
4. Discussion
- The results indicated that using wood products increased the interaction between the frail elderly, improved emotional relations based on cognitive function, and expanded self-expression in a positive way. For example, they became more talkative, more willing to engage one another. An environment containing wood products greatly increasedthe older persons’ mutual interaction and harmonious relations.This finding is potentially significant for the well-being of the elderly because much previous research has connected social interaction with emotionally rich relationships and has found that chances of self-expression reduce the risk of dementia and health decline[17-20].Thus, a habitation with wood products may expand the possibility to improve mental and physical abilities for frail elderly. To provide further evidence for the positive effects of wood products, it will be important to evaluate various features of the interaction, such as person-to-person relations, and group activities.
5. Conclusions
- This studyprovides evidence thatolder persons’ behaviors were changed after using wood products, especially increasing positive social interaction. Wood products significantly increased older persons’ interaction and level of activity. Thus, the use of wood products may enhance the possibility of preventing mental and physical decline in the frail elderly.
ACKNOWLEDGEMENTS
- We express our deepest respect and gratitude for Director Suzuki and the participants of Oasis Co. This research was supported by the Grants-in-Aid for Scientific Research (23330174, 24653134).