-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
p-ISSN: 2167-7263 e-ISSN: 2167-7247
2012; 2(3): 37-42
doi: 10.5923/j.phr.20120203.01
Value of Serum Glycated Albumin in Prediction of Coronary Artery Disease in Type 2 Diabetes Mellitus
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLSaba Irshad1, Rabia Riaz1, Farkhanda Ghafoor2
1Institute of Biochemistry and Biotechnology, University of the Punjab, New Campus, Lahore, 54590, Pakistan
2NHRC, Sheikh Zaid Medical Complex, Lahore, 54590, Pakistan
Correspondence to: Saba Irshad, Institute of Biochemistry and Biotechnology, University of the Punjab, New Campus, Lahore, 54590, Pakistan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Coronary artery disease (CAD) is a major vascular complication of diabetes mellitus and reveals high mortality. Up to 30 % of diabetic patients with myocardial ischemia remain asymptomatic and are associated with worse prognosis compared to non-diabetic counterpart, which warrants routine screening for CAD in diabetic population. The purpose of this study was to evaluate the clinical value of serum glycated albumin level in predicting the presence of CAD in patients with type 2 diabetes. Ninety patients with type 2 diabetes were divided into four groups having the coronary artery disease with lumen diameter narrowing < 30 %, Group II with mild CAD contained those patients with lumen diameter narrowing 30-50 %, and Group III with Major CAD contained those subjects with lumen diameter narrowing 50-70 %. Finally group IV with severe CAD including the patients with lumen diameter narrowing > 70 %. Serum levels of glycated albumin was determined using ELISA as well as serum concentrations of glucose, lipids, were taken in questionnaire in all groups. Serum glycated albumin levels were significantly increased in diabetic patients with CAD.
Keywords: Diabetes Mellitus, Coronary Artery Disease, Glycated Albumin, ELISA, Glycated Hemoglobin
Article Outline
1. Introduction
- Diabetes mellitus is a group of metabolic disorder in which there is absolute or relative deficiency of insulin with resultant hyperglycemia, glycosuria, polyuria and polydipsia, which represent typical clinical manifestations. Diabetes can cause acute or chronic complications. The new classification system identifies three types of diabetes mellitus: type 1, type 2, "and gestational diabetes.
1.1. Diabetes Mellitus and Coronary Artery Disease
- Diabetes mellitus (DM) is common associated with both micro vascular and macro vascular complications. Macro vascular complications manifest themselves as accelerated arteriosclerosis, clinically resulting in premature coronary artery disease (CAD), increased risk of cerebrovascular disease, and severe peripheral vascular disease. Patient with type 2 diabetes mellitus (T2DM) have a two to four fold increase in the risk of CAD[1]. Several independent factors, e.g. insulin resistance, hyperglycemia, hypertension, dyslipidaemia, abdominal obesity and low-grade inflammation, have all been associated with this condition in subjects with type 2 diabetes[2].Diabetic state also promotes the Amadori-modification ofmany circulating proteins, giving rise to concentrations of glycated proteins approximately one and a half to three times those found in non-diabetic persons that reflect integrated glycemia to which the protein has been exposed during its residence time in the circulation[3].
1.2. Glycated Albumin
- Early stage reaction product of albumin or serum protein is called Glycated albumin or Fructosamine[4].Glycated albumin exhibits potential atherogenic effects in various cell types, including mesangial, monocyte- macrophage, mesothelial, endothelial, and vascular smooth muscle cells[3].Glycated albumin is the predominant circulating Amadori -type glycated protein in vivo and plays a major role in the development of diabetic vascular complications. An increased serum level of glycated albumin is associated with the presence and severity of CAD, and may be useful in screening patients with T2DM[5].It is suggested that GA provides a significantly better measure to estimate glycemic control in HD patients with diabetes and that the assessment of glycemic control by HbA1c in these patients might lead to underestimation likely as a result of the increasing proportion of young erythrocyte by the use of erythropoietin[6].
1.3. ELISA
- To evaluate the clinical utility of a highly specific monoclonal antibody directed against the glycated epitopes residing in human albumin, Cohen and Hud developed an ELISA using this antibody to measure glycated albumin in plasma samples from non-diabetic and diabetic individuals[7].Relative percent concentration of glycated albumin in a sample is determined by dividing the microgram glycated albumin in the sample by the total microgram albumin in the sample.
2. Materials and Methods
2.1. Study Design and Study Population
- It was a Cross Sectional Analytical study. Among the study population, 90 cases of type II diabetes were registered in the institute of biochemistry and biotechnology at the University of Punjab Lahore. Inclusion Criteria was that individuals with type II diabetes and undergoing diagnostic coronary angiography to find out the presence and extent of CAD were included in this study group and all individuals with type 1 diabetes rheumatoid arthritis and any other inflammatory diseases were excluded from the study.
2.2. Data Collection
- 90 cases of type II diabetes undergoing coronary angiography for the diagnosis of CAD were taken from the Punjab institute of cardiology. All the patients were angiographically confirmed for coronary artery disease. The demographic information like (name, age sex, height, and weight), history of present illness including history of diabetes and cardiac history were taken. The severity of CAD was based on lumen diameter narrowing as < 30 % (Minor CAD), 30-50% (mild CAD) 50-70 % (moderate CAD) and > 70 % (severe CAD) on visual assessment by experienced observer.
2.3. Sample Collection and Serum Separation
- 5 ml of venous blood was drawn from each selected subject using standard venepuncture techniques. The sterilized needles were used for the collection of blood from all the patients. The blood was allowed to clot at the room temperature for 2-3 hours. The clot was then removed while the supernatant was centrifuged at 4000 rpm.
2.4. Quantitative Determination of Glycated Albumin and Total Albumin
- Glycated albumin and total albumin was determined in each samples by using commercially available Glycaben ELISA kit. Glycated albumin can be reported as an absolute concentration (mg / ml) or as a percent (%) of total albumin as calculated from the following equation using determined for each of sample:% Glycated Albumin sample = 100% x Glycated albumin sample / Total Albumin sample
3. Results
3.1. Composition of Study Groups
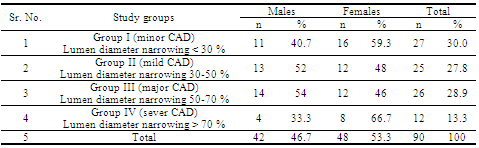
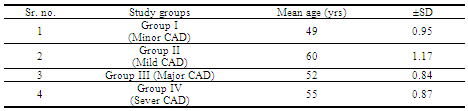
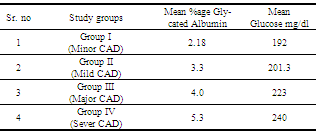
- Out of 90 total subjects 42 (46.7 %) were males and 48 (53.3 %) were females. In Group I (minor CAD), 11 (40.7 %) were males and 16 (59.3 %) were females. In Group II (mild CAD), 13 (52 %) were males and 12 (48 %) were females. In the Group III (Major CAD), 14 (54 %) were males and 12 (46 %) were females. In the Group IV (sever CAD), 4 (33.3 %) were males and 8 (66.7 %) were females (Table 1).Mean age group and SD were calculated for each group. The mean age and SD of the group I (minor CAD) was 48 ±0.95. The mean age and SD of the group II (mild CAD) was 61 ±1.17. The mean age and SD of the group III (Major CAD) was 53 ±0.84 and of the group IV (severs CAD) was 55 ±0.87 (Table 2)
|
|
|
|
|
|
|
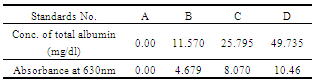
3.2. Determination of Total Albumin and Glycated Albumi by ELISA
- There were three types of information sources for the total albumin and glycated albumin ELISA i.e. the calibration of the standards, quality control samples and the test specimens. These three were subjected to the analytical procedure and some response (color development) was obtained.After running the ELISA test concentration of total albumin and glycated albumin for standards were calculated (Table 8 and 9). Graphical representation is in Fig. 1 (A), (B).
|
|
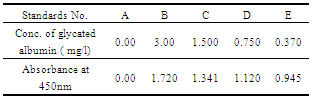
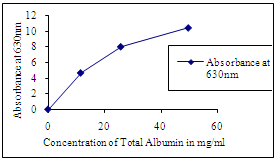 | Figure 1(A). Standard curve for total albumin, whose absorbance is taken at 630 nm |
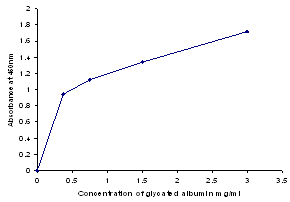 | Figure 1(B). Standard curve for total albumin, absorbance is at 450 nm |
|
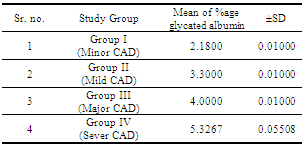
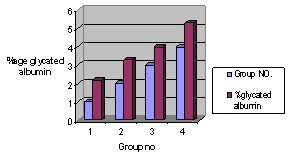 | Figure 2. % age glycated albumin in each study group, groups are taken on x-axis and % age glycated albumin is on y-axis |
3.3. Assessment of Mean BMI With % Age Glycated Albumin
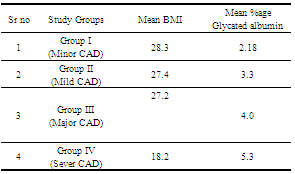
- Mean BMI = height /weightIn-group I (minor CAD) the mean BMI was 28.3, in-group II (mild CAD) the mean BMI was 27.4. In-group III (Major CAD) the mean BMI was 27.2 and in-group IV (sever CAD) the mean BMI was 18.2. The mean % age glycated albumin in the group I was 2.18, in the group II 3.3, in the group III 4.0 and in the group IV the mean % age glycated albumin was 5.3 (Table 11). There is negative association between mean BMI and % age glycated albumin (Fig. 3).
|
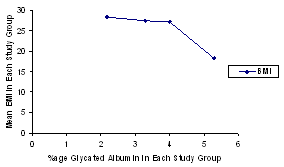 | Figure 3. Assessment of mean BMI with % age glycated albumin, % age glycated albumin decreases with increase in BMI values |
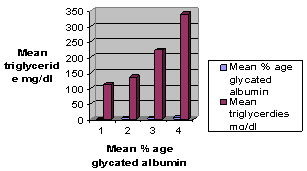
3.4. Association between Mean Triglycerides and Mean % Age Glycated Albumin
- The mean % age glycated albumin and triglycerides level were calculated for each study group (Table 12). It was observed that % age glycated albumin level increases as the triglyceride level increases, providing a direct relationship between % age glycated albumin and TG (Fig. 4).
|
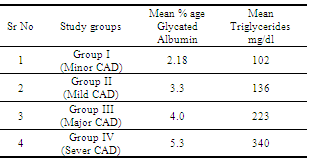
 | Figure 4. Association between mean triglycerides and mean % age glycated albumin |
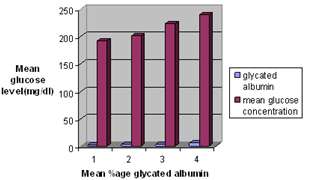
3.5. Association between Mean Glucose Level and Mean % Age Glycated Albumin
- The mean % age glycated albumin and glucose level were calculated for each study group (Table 13). It was observed that % age glycated albumin level increases as the glucose level increases, providing a direct relationship between %age glycated albumin and glucose (Fig. 5).
|
 | Figure 5. Association between glucose level and mean % age glycated albumin |
4. Discussion
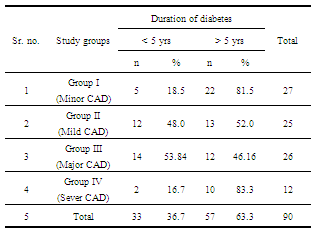
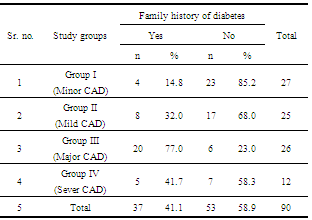
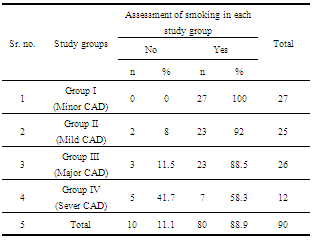
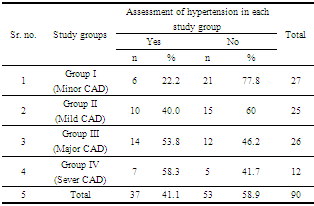
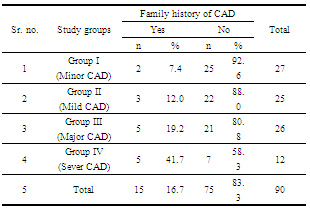
- Diabetes has been recognized as an important risk factor for CAD, and diabetic patients are at 2-fold increased risk of cardiovascular mortality compared to their non diabetic counterparts[8]. Previous studies have demonstrated that silent myocardial ischemia, which is mainly caused by autonomic neural dysfunction, occurred in about 20 % to 25 % of diabetic patients, and the prevalence may be as high as 60 in those at high-risk[9].All proteins in the body can be modified by non- enzymatic glycation. In diabetes mellitus the extent of the non- enzymatic glycation of proteins increases, compared with non-diabetic subjects, which may comprise at least a part of diabetic complications[10]. Among these modified proteins, measurement of HbA1c has been applied for clinical use in order to monitor chronic glycemic control in diabetic patients. But now we try to provide the better indicator of glycemic control in CAD patients which is Glycated albumin, is a kind of early-stage amadori-modified reaction products formed from Schiff's base adducts and has been implicated in the pathogenesis of diabetic complications and better indicator[11, 3]. Stable fraction of glycated hemoglobin (HbA1c) is routinely measured in the majority of patients with diabetes around the world; Since HbA1c reflects glycemic control over the preceding 2-3 months[12]. However HbA1c may not be suitable for evaluation of short term variation in glycemic control because of long life span of erythrocytes (120 days). Because the turnover of human serum albumin is much more rapid (half life of 15-20 days) than that of hemglobin, the measurment of glycated albumin (GA) provides an index of glycemic control over a short period of time than the measurment of HbA1c[13, 14]. There are several risk factors associated with coronary artery disease, such as family history of diabetes and coronary artery disease, smoking, hypertension, hyperglycemia, hypertriglyceridemia, BMI.The prevalence of CAD increased with age and duration of diabetes[15] and in this study 57 (63.3 %) subjects have duration of diabetes more than 5 years and mean age is 55±0.87.Cigarette smoking is a leading risk factor for CVD. Patients with diabetes who are smokers are doubly at risk[16]. Unfortunately, many patients continue to smoke despite having diabetes; for these patients, the benefits that can be derived from modifying other risk factors are mitigated. In this study, 80 (88.9 %) subjects were smokers.High blood pressure accounts for 20 to 25 % of all CAD deaths. Subjects with hypertension have a two-fold higher risk of CAD[15]. In this study, Out of 90 subjects, 53 (58.9 %) patients were hypertensive.Serum glycated albumin levels are low in obese[17]. The result of this study shows the negative association of % age glycated albumin with the BMI. And we found that serum GA levels are influenced by BMI in diabetic patients[18]. Hyperglycemia, leading to the formation of advanced glycation end products (AGE), on vascular function[19]. Glycated albumin is a kind of Amadori-modified derivatives, accounting for about 80 % of the circulating glycated proteins in vivo. Hyperglycemia increases serum glycated albumin level, and the extent of increase reflects glycemia status of diabetic patients over a retrospective period[5]. Although relationship between diabetic atherogenesis and several common risk factors plus non traditional risk markers have been studied extensively and the data is having some controversies[20].
5. Conclusions
- Previous studies showed that glycated albumin was more sensitive than glycosylated hemoglobin (HbA1c) in the evaluation of the severity of diabetes. The present study showed that glycated albumin was an independent risk factor for CAD in patients with type 2 diabetes, with and predicts the coronary artery disease in type 2 diabetes mellitus.
ACKNOWLEDGMENTS
- The authors acknowledge the enabling role of Miss. Blessy Shahzad, Miss Saima Naz, for use full discussion and Dr. Saqib, Dr. Farooq, for blood collection at PIC, Lahore.