-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Public Health Research
2012; 2(2): 16-20
doi: 10.5923/j.phr.20120202.03
Chronic Non-Communicable Disease Prevention in Russian Federation (RF)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLKonstantin G. Gurevich
UNESCO Chair, Moscow State University of Medicine and Dentistry, Moscow, 127473, Russia
Correspondence to: Konstantin G. Gurevich , UNESCO Chair, Moscow State University of Medicine and Dentistry, Moscow, 127473, Russia.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
In the Soviet Union, there was one of the most developed medical systems all over the world with the main accent to preventive medicine. The main component of chronic disease prevention was named “dispanserization”. It includes nurses, doctor’s control, clinic and laboratory methods of investigation one time a year and dynamic control during the year (if it was needed). Perestroika resulted in breakup of the medicine. In 2006, the Ministry of Public Health decided to reconstruct the system of prevention medicine, but it does not work. For example, in Russia, the average duration of life is the lowest in Europe, it does not rank in first hundred of the most development countries anymore; it is on average 12-15 years lower than in Scandinavia. RF is the country with most smokers from all over the world. In 2006, the Ministry of Public Health decided to reconstruct the system of dispanserization. Some of methods of health observation are not supported by evidence-based-medicine. In 2009, the Ministry of Public Health organized the “center for health”. But also this system does not work.
Keywords: RF, Prevention Medicine, State Policy, Dispanserization, Center For Health, Chronic Diseases
Article Outline
1. Soviet Union
- In USSR it was used the Semashko health system. Nicolay A. Semashko (1849-1947) was the first minister of public health in Soviet Union (1918-1930). He developed the new health system just after revolution (1917). The system was based on two main principles: free medical care access and emphasis on prevention of communicable diseases. Patients did not pay any money for their visit to doctor, medical care costs were covered by government[1,2].Semashko medical system was centralized and managed by Ministry of Public Health. The Ministry planned how many medical staff of medical facilities will be needed next year, next five years and so on. This allowed do not have any great difference in medical care access and quality between regions of country, rural and urban territories[1]. But sometimes there was deficient in access to medical care[3].There was the strong control on communicable diseases. It includes sanitary observation, isolation of patients with infectious diseases, immunization and so on. Up to 100% of children and 90% of adults were vaccinated. Strong state regulation did not allow people any access to working place, school or nursing without immunization. Every year children were controlled on excrement contamination by helminthes[4].In the years 1970-1980 in the Soviet Union, there was one of the most developed medical systems all over the world. The average duration of life was one of the tenth all over the world and one of the first in Europe. Sometimes the health system was cost-non-effective, but it works[3].The main component of chronic disease prevention was named “dispanserization”[5,6]. It appeared in 1960-1970 years. Dispanserisation includes nurses, doctor’s control, clinic and laboratory methods of investigation one time a year and dynamic control during the year (if it was needed). In big enterprises there was a doctor or a nurse, which worked full time. In all schools there also were nurses. This medical stuff made up a dynamic observation of all individuals, and if it was needed referred individual to clinics to detail examination[5]. As a rule, nurses and doctors in schools and enterprises also made immunization due to “national schedule of vaccination”. This schedule was developed by Ministry of Public Health and determined time periods in which immunization have to be done. People did not have any freedom to do vaccination or not. Only in medical reasons (for example, kidney disease) individual could be not vaccinated[7,8].
2. Perestroika
- Perestroika (‘reconstruction’, during the 1980s) resulted not only in breakup of the Soviet Union, but also it resulted in the breakdown of the main governmental institutes, including those for medicine. Management of health system was decentralized There was a strong deficient of financial support of medical care and medical access[3].In new financial mechanism doctors and nurses receive money for medical service. So, as more there will be service, as much salary they will have. In such conditions medical stuff does not have any motivation to provide prevention procedures or to help patient to make up their individual behavior healthier[2]. Created as a part of the general Russian medical system, prevention care in Russia has mirrored all the good and bad qualities of that system during Perestroika. The system of dispanserization and rehabilitation was generally destroyed [9].Now in Russia, the average duration of life is the lowest in Europe, it does not rank in first hundred of the most development countries anymore; it is on average 15-17 years lower than in Scandinavia, Japan, France, and USA[10,11]. The average duration of life form men is about 10 years lower than those for women. As it visible from Fig. 1, average duration of life fall down after Perestroika. Resent years it increases but average duration of life is still lower than in time of Soviet Union. In Russia there is one of the highest levels of children which are died during the first year of life (Fig 2)[12].
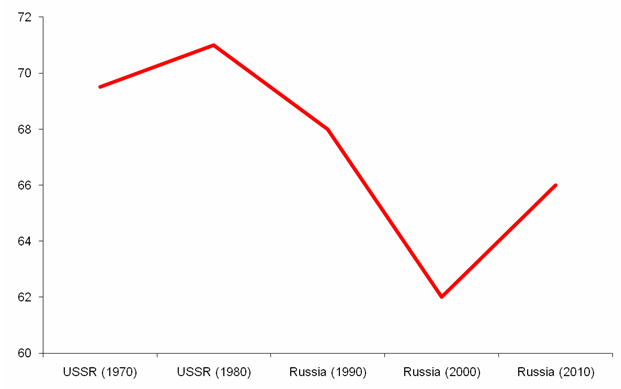 | Figure 1. The Average Duration of Life in USSR and Russia [12] |
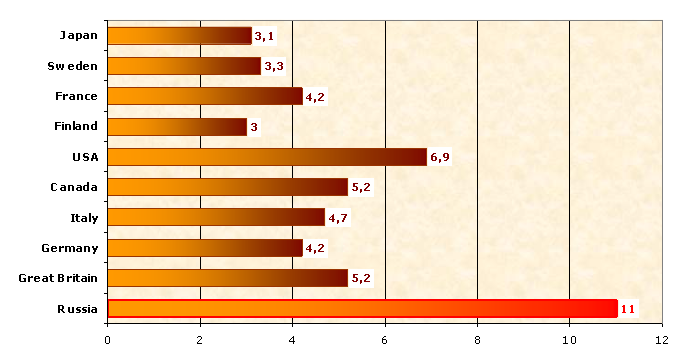 | Figure 2. Number of Children Died During the First Year of Life (on 1000 Born Alive) [10], [12] |
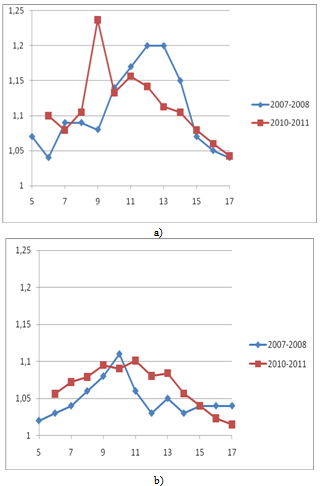 | Figure 3. Body Mass Index of Moscow Schoolchildren in Comparison with Age Norms. (a) Boys, (b) Girls |
|
|
3. Present Day System
3.1. Dispanserization
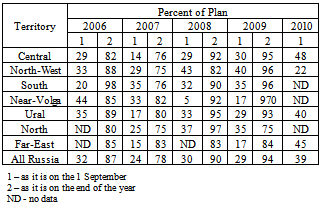
- In 2006, the Ministry of Public Health decided to reconstruct the system of dispanserization[26]. It was made up as one of the national priority projects, developed by the president of country. But nowadays the system of dispanserization does not work.The first years of dispanserization (2006-2009) demonstrated to take in observation about 10% of working people. But WHO proposed that prevention programs are only effective if it includes 80% and more. In 48% of cases the patients examined non-regularly. The untimely examination under all types of diseases took place in 34.3%; incomplete examination took place in 41.7%, the health promotion activities had lower quality in 39.9% and in 36.4% the counselling of specialists provided untimely[27].Every year Ministry of Public Health publishes plans of dispanserization. But this plans are not realised (Table 4). Also it is visible, that the main cases of dispanserization are making up in the end of the year. So, the quality of such dispanserization is a very big question. Also, about 10% of women do not have any access to mammography on the living territory. Some territories have problems with laboratories to make up biochemical analysis of blood[28].
|
3.2. Centre of Health
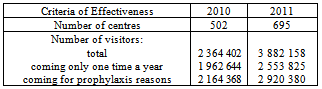
- In 2009, the Ministry of Public Health organized the “centre for health” [31]. In 2010, 502 centers were open in different parts of the country. In 2011, their number was 695. It was supposed that such centers will organize all prevention work in the territory, with the main accent to primary prophylaxis. But also this system does not work (Table 5):● “Centre for health” is open for everybody. More then 80% visitors are people older 75;● There is about 50% shortage of doctors and nurses working in such centers. Many doctors and nurses already worked, but do not have appropriate education;● Many centers do not have any possibility for health promotion (for example, as commercial);● Near 4 million of people went centers in 2011, which is equal to 2,8% citizens of Russian Federation;● Only 25% of visitors did the visit due to prophylaxis reasons;● 74.5% of visitors come to centers only one time a year.
|
4. Conclusions
- The public health system of RF based on Semashko model failed down during Perestroika. The main principles of the system nowadays do not work. A new system still did not appear. Ministry of Public Health provides policy of both preservation of Semashko model, and its reform in the same time. It may be concluded that Ministry of Public Health does not strongly know what to do with public health system. Special sanitary agency (Rospotrebnadzor) and special agency to control work of Ministry of Public Health (Roszdravnadzor) were organized, but nothing generally changed. In present-day public health system money allocates only for immunization as a prevention work. Some money for health promotion is in Ministry of Public Health. But program have low effect. The budget for health promotion is about 10% of the same for commercial of one of fast-food restaurant.In the same time, it is registered dramatically growing up prevalence of risk factors for non-communicable diseases[3]. The first stage of reform of public health system is going on now (2009-2015). But no serious changes were registered.In 2010 the Government of RF adopted National Anti- tobacco Policy[33]. It is planned that to 2015 smoke will be reduced on 10-15%. What will be happen, we will see.In general, there is no state position about how prevention work has to be done. There is total deficient of access to stadiums, swimming-pools, fitness clubs and other places of physical activity. Sometimes when there is some access, the price for visit is too high. TV commercial in general provides unhealthy behaviour. There are no state school health programs.Chronic disease prevention programs in RF nowadays are initiated by the initiative of local parliaments of international organizations (for example, Moscow, Kazan’, Hanty- Mansi’sk). All initiatives of Ministry of Public Health are non-effective or low-effective. So, the Ministry exhausted all the trust itself. Only if the Parliament of RF will be the main in organization of prevention programs something positive seems to be done.
ACKNOWLEDGEMENTS
- The work is supported by grant of President RF MD- 1594.2012.7.
References
| [1] | Ibragimov NG. History of the founding and development of the sanatorium-health resort system in Bashkiria (on the 110th anniversary of the birth of N. A. Semashko), Vopr. Kurortol. Fizioter. Lech. Fiz. Kult, vol. 1, pp. 72-73, 1985. |
| [2] | Antoun J, Phillips F, Johnson T. Post-Soviet transition: improving health services delivery and management, Mt. Sinai J. Med., vol.78, pp. 436-438, 2011. |
| [3] | Popvich L, Potapchik E, Shishkin S, Richardson E, Vacroux A, Mathivet B. Russian Federation. Health system review, Health Systems in Transition, vol. 7, pp. 1-190, 2011. |
| [4] | Gotsadze G, Chikovani I, Goguadze K, Balabanova D, McKee M. Reforming sanitary-epidemiological service in Central and Eastern Europe and the former Soviet Union: an exploratory study, BMC Public Health, vol. 2010, pp. 440-460, 2010. |
| [5] | Order #770 (30 May 1986) Ministry of Public Health USSR “How to organize total dispanserization of people” |
| [6] | The dispanserization and public health in Russia. Report 2: The dispanserization technique as a tool of prevention approach in public health, Probl. Sotsialnoi. Gig. Zdravookhranenniiai. Istor. Med., vol. 3, pp. 4-7, 2011. |
| [7] | Tregubova ES, Nekhoroshev AS. Evaluation of work conditions for teachers of schools, Med. Tr. Prom. Ekol, vol. 8, pp. 29-34, 2011. |
| [8] | The role of preventive activities in the process of disease prevention as an integral part of primary medical sanitary care, Probl. Sotsialnoi. Gig. Zdravookhranenniiai. Istor. Med., vol. 8, pp. 44-46, 2011. |
| [9] | Grigorenko EL. Russian "defectology": anticipating Perestroika in the field, J. Learn Disabil., vol. 31, pp.193-207, 1998. |
| [10] | WHO. World Health Statistics, 2011. |
| [11] | Antonova O, Brui B, Gorbunova T, Nikitina S. The demographic situation in the Russian Federation during the structural transition associated with perestroika and the subsequent economic stabilization, Vopros. Stat., vol. 12, pp. 53-56, 1997. |
| [12] | www.gks.ru |
| [13] | Gurevich KG, Aksenova KI, Degtyarev VP, Kazulin AN, Klimina NV, Konorov ND, Kuz’mina EM, Maev IV, Martynov UV, Mishin VU, Orestova EV, Panchenko LF, Popkov SA, Postugalov SN, Pustovalov DA, Fabrikant EG, Introduction into healthy life style, MSUMD, Moscow, 2005. |
| [14] | Gazina DN, Gurevich KG. Obesity in Moscow school age students: prevalence, age- and gender- related features, Food and Public Health, vol. 1, pp. 1-5, 2011. |
| [15] | Spruijt-Metz D. Etiology, Treatment and Prevention of Obesity in Childhood and Adolescence: A Decade in Review, J Res Adolesc., vol. 21,pp. 129-152, 2011. |
| [16] | Sosa ET. Mexican American Mothers' Perceptions of Childhood Obesity: A Theory-Guided Systematic Literature Review, Health Educ Behav, May 6, 2011. |
| [17] | Bibbins-Domingo K, Coxson P, Pletcher MJ, Adolescent overweight and future adult coronary heart disease, New Engl. J. Med., vol. 357, pp. 2371-2379,2007. |
| [18] | Popkin BM, Conde M, Hou N, Monteiro C, Is there a lag globally in overweight trends for children compared with adults?, Obesity, vol. 14, pp. 1846-1853, 2006. |
| [19] | Biro FM., Wien M. Childhood obesity and adult morbidities, Am. J. Clin. Nutr., vol. 91, pp. 1499S-1505S, 2010. |
| [20] | Poirier P, Giles TG, Bray GA. et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss, Arterioscler. Thromb. Vasc. Biol., vol. 26, pp. 968-976, 2006. |
| [21] | Nazim J, Starzyk J. Obesity in children and adolescents and diabetes, Przegl. Lek., vol. 66, pp. 96-99, 2009. |
| [22] | Burdukova EV, Orlov VA, Pustovalov DA, Dmitrieva EA, Gurevich KG. Features health and physical development of school-children 14-17 years old in Moscow, Vestnik Novgorod State University, vol. 62, pp. 8-11, 2011. |
| [23] | Gurevich KG, Salmanov PL, Pustovalov DA. Distance measur-ing of physical activity among students and workers of Moscow State University of Medicine and Dentistry, Am. J. Med. & Med. Sci., vol. 1, pp.1-4, 2011. |
| [24] | Glazunov IS, Stachenko S. Health promotion and prophylaxis of noncommunicable diseases in Russia and Canada. Moscow, Medicine, 2006. |
| [25] | Schultz DS, Rafferty MP. Soviet health care and perestroika, Am. J. Public Health, vol. 80, pp. 193-197, 1990. |
| [26] | Order #80n (20 Feb 2008) Ministry of Public Health and Social Development RF “About organization in 2008-2009 of additional dispanserization of working people”. |
| [27] | Gasanova AZ. The quality of dispanserization of working population in municipal polyclinics, Probl. Sotsialnoi. Gig. Zdravookhranenniia i Istor. Med., vol. 4, pp. 38-40, 2011. |
| [28] | Kosik NV. Optimization of organization and control of additional dispanserization. Rayzan’, 2010. |
| [29] | Gurevich KG, Kosik NV, Nikonov EL. The main problems during additional observation of adult men, Evidence Base Medicine and Epidemiology, vol. 1, pp.25-33, 2009. |
| [30] | Shchepin OP, Rastegaev VV. The means of increasing the role of dispanserization of population in diseases prevention in municipal health care, Probl. Sotsialnoi Gig. Zdravookhranenniia i Istor. Med., vol. 4, pp. 20-22, 2011. |
| [31] | Order #597 (19 Aug 2009) Ministry of Public Health and Social Development RF “Organization of centers for health to form healthy life-style in Russian citizens including reduction of alcohol intake and smoking” |
| [32] | www.minzdravsoc.ru |
| [33] | Government Resolution #1563 (23 Sept 2010) |