-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(5): 59-63
doi:10.5923/j.otolaryn.20170605.01

Rare Anatomical Variations of Nasal Turbinates: A Prospective Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBorligegowda Viswanatha, Suprabha Munnur Haridas, Maliyappanahalli Siddappa Vijayashree, Abhilasha Somshekhar, Praveena Vemanna
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

With the advent of nasal endoscopes and CT scans, many anatomical variations of nasal turbinates have been described. The most commonly described variation is middle turbinate pneumatization (concha bullosa). Paradoxical middle turbinate is another rarely encountered anomaly. Superior and inferior turbinate pneumatizations have also been described. Rare turbinate anomalies that resemble the middle turbinate are described in recent years. They are - accessory middle turbinate, secondary middle turbinate and bifid inferior turbinate.In the present study 900 patients with sinonasal disease who underwent nasal endoscopy, were evaluated for rare anatomical nasal turbinate variations - accessory middle turbinate, secondary middle turbinate and bifid inferior turbinate.In this study there were 6 patients with accessory middle turbinate, 2 patients with secondary middle turbinate and one patient with bifid inferior turbinate.
Keywords: Anatomical variations, Nasal turbinates
Cite this paper: Borligegowda Viswanatha, Suprabha Munnur Haridas, Maliyappanahalli Siddappa Vijayashree, Abhilasha Somshekhar, Praveena Vemanna, Rare Anatomical Variations of Nasal Turbinates: A Prospective Study, Research in Otolaryngology, Vol. 6 No. 5, 2017, pp. 59-63. doi: 10.5923/j.otolaryn.20170605.01.
Article Outline
1. Introduction
- The embryological development of the nasal turbinate is a complex process. During this development anatomic variations may occur at multiple points [1]. The nasal turbinates extends from the lateral nasal wall into the nasal cavity. The middle turbinate originates from the second ethmoturbinal and the inferior turbinate develops from the maxilloturbinal. The uncinate process takes its origin from the first ethmoturbinal. The supreme, superior and middle turbinates are parts of the ethmoid bone. The inferior turbinates are a pair of independent bones [2, 3].Different anatomic variations of the middle turbinate have been reported. They are choncha bullosa, the paradoxically bent middle turbinate, secondary middle turbinate, accessory turbinate, duplicate turbinate and sagittally clefted middle turbinate [1, 4-7]. These variations are important because they can predispose to the inflammatory pathologies. Middle turbinate is used as an important landmark in endoscopic sinus surgery. Awareness of anatomical variations of turbinates and its clinical importance are important for otorhinolaryngologist. They are useful in evaluation of patients with nose and paranasal sinus diseases and to avoid complications during endoscopic sinonasal surgery [1]. In the present study 900 patients with sinonasal disease who underwent nasal endoscopy, were evaluated for rare anatomical nasal turbinate variations - accessory middle turbinate, secondary middle turbinate and bifid inferior turbinate.
2. Aim of the Study
- To study the rare anomalies of the nasal turbinates: 1. Accessory middle turbinate, 2. Secondary middle turbinate and 3. Bifid inferior turbinate.
3. Materials and Methods
- In this study 900 patients with various sinonasal complaints, undergoing diagnostic nasal endoscopy were evaluated for rare turbinate anomalies. There were 6 patients with accessory middle turbinate, 2 patients with secondary middle turbinate and one patient with bifid inferior turbinate.1. Accessory middle turbinate:In this study here were 6 patients with accessory middle turbinate. They went diagnostic nasal endoscopy for their nasal complaints. Four patients were male and two patients were female. Four patients had deviated nasal septum, one patient had epistaxis and one patient had allergic rhinitis. All the patients underwent required treatment. Accessory middle turbinate was unilateral in five cases and bilateral in one case. In all the 6 patients accessory middle turbinates were asymptomatic.
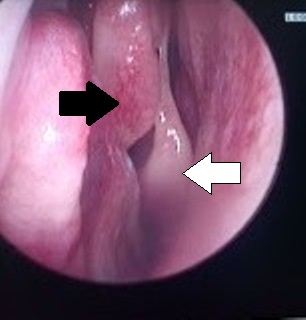 | Figure 1. Endoscopic picture showing accessory middle turbinate [black arrow] and middle turbinate [white arrow] on the right nasal cavity |
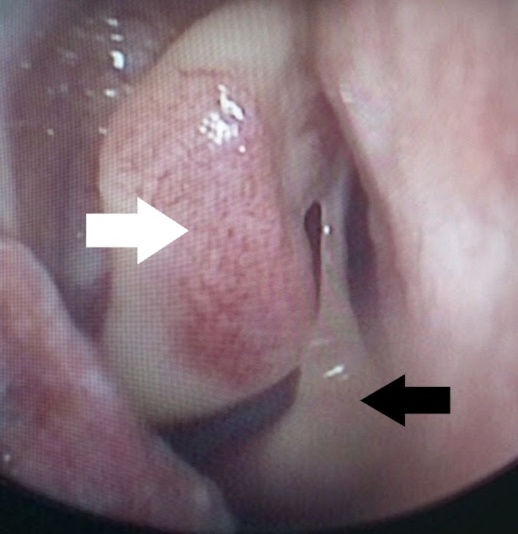 | Figure 2. Endoscopic picture showing accessory middle turbinate [black arrow] and middle turbinate [white arrow] on the right nasal cavity |
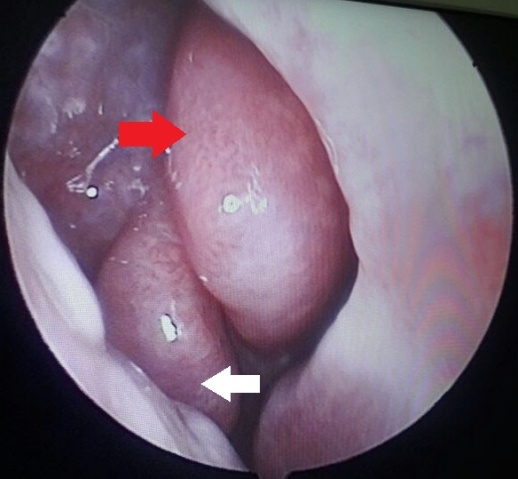
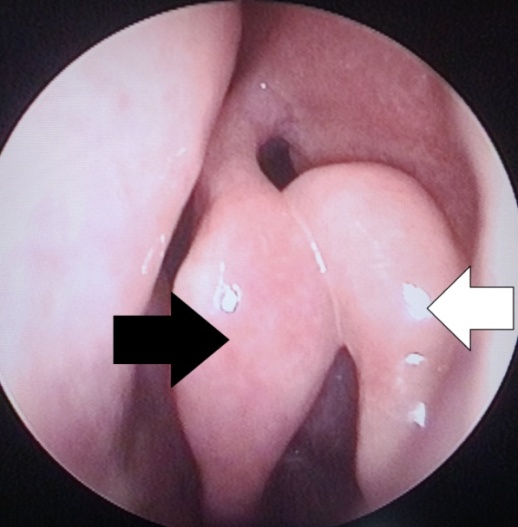 | Figure 3. Endoscopic view of the middle turbinates [white arrow] showing the secondary middle turbinate [black arrow] |
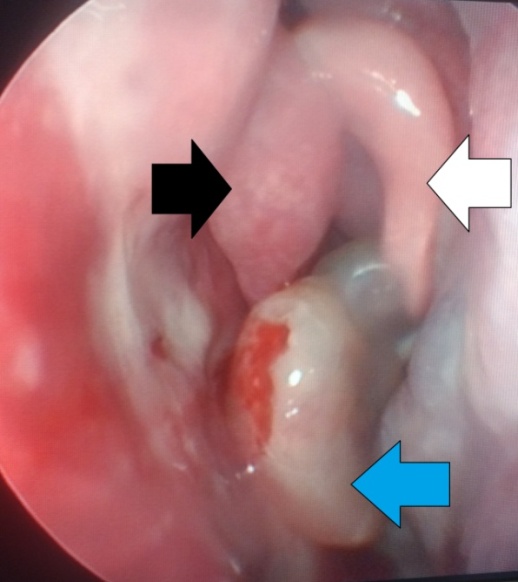 | Figure 4. Endoscopic view of the middle turbinates [white arrow] showing the secondary middle turbinate [black arrow] and antro choanal polyp[blue arrow] |
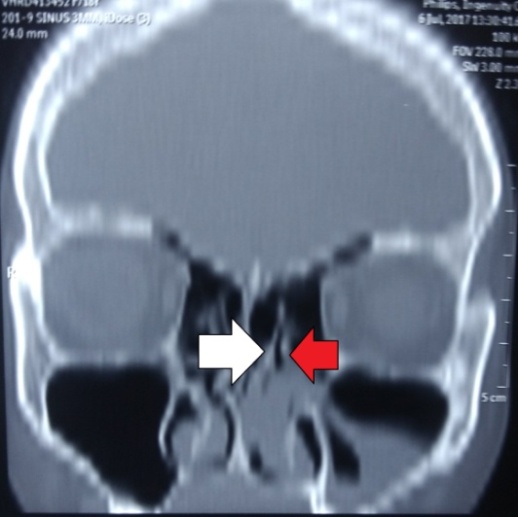 | Figure 5. Coronal CT scan of the paranasal sinuses showing the left middle turbinate [white arrow], secondary middle turbinate [red arrow] and soft tissue mass in the left maxillary antrum and nasal cavity |
 | Figure 6. Axial computed tomography scan of the paranasal sinuses showing the soft tissue mass in the left maxillary antrum and nasal cavity |
 | Figure 7. Endoscopic view showing the bifid inferior turbinate [white arrow] and middle turbinate [red arrow] on the right side |
 | Figure 8. Coronal CT scans of the paranasal sinuses showed a right bifid inferior turbinate and uncinate process of that side is absent |
4. Discussion
- Turbinate anomalies that can mimic middle turbinate are the accessory middle turbinate, secondary middle turbinate and bifid inferior turbinate [8, 9]. Accessory middle turbinate has been described as a medially bent and an anteriorly folded uncinate process [8, 9]. It can resemble a secondary middle turbinate or bifid inferior turbinate. It is different from the secondary middle turbinate because of its distinct developmental origin [9, 10]. Accessory middle turbinate is a variation formed by displacement of the uncinate process medially [10]. In a study by Murat Ozcan et al the incidence of accessory middle turbinate was found to be 6.8% [10].According to Bae S and Lim S [8], if the normal uncinate process is present in a patient with a doubled middle turbinate, the term accessory middle turbinate is appropriate. In contrast, if a turbinate like structure originates from the inferior turbinate and the uncinate process is absent, the term bifid inferior turbinate is appropriate.Accessory middle turbinate may appears as an additional middle turbinate during endoscopic examination. Murat Ozcan [10] suggests that during surgical interventions of ostiomeatal unit, frontoethmoid recess or nasolacrimal duct, an accessory middle turbinate that resembles real middle turbinate should be differentiated and correct anatomic orientation should be maintained [10].In the present study there were six cases of accessory middle turbinate. Four cases had bilateral accessory middle turbinate and two cases had unilateral accessory middle turbinate. They were detected during nasal endoscopic examination for other sinonasal symptoms.The secondary middle turbinate is a rare anatomical nasal cavity variation that was first described by Khanobthamchai et al. [11]. It consists of bone covered by soft tissue and originates from the lateral wall of the middle meatus [5, 11, 12]. The secondary middle turbinate, a bony projection that arises from the lateral nasal wall, is a rare variation, differing from the accessory middle turbinate by its distinct developmental origin [9]. It originates from the lateral nasal wall just beneath the basal lamella [12]. The incidence has been reported to be 1.5% by Khanobthamchai et al [11], 6.8% by Aykut et al [13] and 0.8% by Aksungur et al [4]. Khanobthamchai et al defined the secondary middle turbinate as an incomplete anterior wall of the ethmoid bulla without explaining its club-like tip [11]. Aksungur et al suggested that secondary middle turbinate might be an additional turbinate originating embryologically from a section of a frontal ridge [4]. The secondary middle turbinate can be mistaken for a polyp or an osteoma at endoscopical examination [5]. The secondary middle turbinate projects from the lateral nasal wall in the middle meatus, and traverses medially and superiorly [11]. Aksungur et al. [4] and Apaydın et al. [5] reported cases with secondary middle turbinate, which curve inferiorly and medially. According to Apaydın et al., superomedially projected secondary middle turbinate has no clinical significance. However, inferiorly projected secondary middle turbinate, especially if hypertrophied and pneumatised, may narrow the ostiomeatal unit and predispose to inflammatory sinus disease [1, 5, 12]. In the present study one patient had had inflammatory antro choanal polyp on the same side. It was interesting to note that the soft tissue mass had come out of the antrum before completely filling the nasal cavity. Usually antro choanal polyps partially or completely fill the antrum before it comes into the nasal cavity through the ostium. This may be due to altered physiology of the air flow in the nasal cavity caused by the secondary middle turbinate.The secondary middle turbinate was reported to be bilateral in all cases in the literature [4, 5, 11]. Aksungur et al examined coronal computed tomographies of 253 cases of sinusitis for the presence of additional turbinates and bilateral secondary middle turbinates were detected in two cases [4]. Adil Ozturk reported first case of unilateral inferolaterally projecting secondary middle turbinate [1]. In the present study both the cases had unilateral secondary middle turbinate.Bifid inferior turbinate was described for the first time by Aksungur et al [4] in 1999. It is an extremely rare anatomical variation that arises during embryological development of the lateral nasal wall. There will be two turbinates in place of the single, inferior turbinate. It is diagnosed by paranasal sinus CT and endoscopic nasal examination [3].The first case described by Aksungur et al [4] had a unilateral bifid inferior turbinate and bilateral secondary middle turbinates; the uncinate process on the side of the bifid inferior turbinate was absent. Another case reported by Spear et al had bilateral bifid inferior turbinates and did not have any variations of the middle turbinate. The uncinate processes were absent bilaterally [7]. Seluck published report of bilateral bifid inferior turbinates coexisting with a unilateral secondary middle turbinate. [3]. Murat ozcan et al evaluated nose and paranasal sinus CT scans of 384 patients and found one case of bilateral bifid inferior turbinate [10]. In the present study patient had an unilateral bifid turbinate. To the best of our knowledge ours is 5th reported case of bilateral bifid inferior turbinate.According to Murat et al [10] none of the turbinate variations have significant association with mucosal pathologies. They are of the opinion that during endoscopic sinus surgery, whether variation of the turbinates need surgical intervention or not is important for choosing the appropriate treatment approach.
5. Conclusions
- The uncommon anatomical variations of nasal turbinates are accessory middle turbinate, secondary middle turbinate and bifid inferior turbinate. Nasal endoscopic examination and CT scans can easily identify such uncommon anatomical variations. These variations may not be clinically significant. None of the turbinate variations have significant association with mucosal pathologies. The knowledge of anatomical anomalies of turbinates is important in evaluating patients with nasal and paranasal sinus diseases. In symptomatic patients, surgeon should be aware of these variations to avoid any complications during surgery.