-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(4): 57-58
doi:10.5923/j.otolaryn.20170604.03

Pyocele of the Middle Turbinate
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSuprabha MH, Borligegowda Viswanatha
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Mucoceles are rare lesions and the majority of mucoceles are seen in the fronto-ethmoidal complex. A pyocele occurs when a mucocele becomes infected. A case of pyocele arising from the middle turbinate is reported along with the review of literature.
Keywords: Middle turbinate, Pyocele, Mucocele
Cite this paper: Suprabha MH, Borligegowda Viswanatha, Pyocele of the Middle Turbinate, Research in Otolaryngology, Vol. 6 No. 4, 2017, pp. 57-58. doi: 10.5923/j.otolaryn.20170604.03.
1. Introduction
- The middle turbinate is part of the ethmoid bone. It may be cellular, or cystic. Enlargement of cystic turbinate may result in deranged nasal physiology of the paranasal sinuses. Mucocoeles are epithelial-lined cavity containing mucus ad they slowly expand [1]. Pneumatised middle turbinate is known as concha bullosa. The pathogenesis of infections of the concha bullosa region is unclear. The concha bullosa has a mucociliary transport system which connects the aerated cell to the frontal recess, lateral sinus or hiatus semilunaris, through an ostium. Obstruction of the ostium and inflammatory changes within it can cause mucocele in the concha bullosa. A pyocele occurs when a mucocele becomes infected [1, 2]. This is, to our knowledge, the third case of middle turbinate pyocele reported in the literature.
2. Case Report
- An 18 year old female patient presented with history of nasal obstruction on the left side. Initially it was partial nasal obstruction and gradually progressed to the present state. There was no history of nasal discharge, pain or fever. There were no other rhinological or ophthalmological symptoms. There was no history of trauma or surgery. Patient did not find any improvement with antibiotics medicines and steroid nasal spray.Anterior rhinoscopic examination showed a large mass in the left nasal cavity arising in the middle turbinate region. On probing it was found to be bony hard and it was arising from the lateral wall of the left nasal cavity. There were no signs of overt infection in the nasal cavity or nasopharynx. Diagnostic endoscopy showed a mass in the region of middle turbinate and it was hard on palpation [Figure 1].
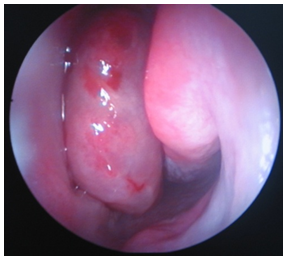 | Figure 1. Endoscopic picture showing mass in the middle turbinate region |
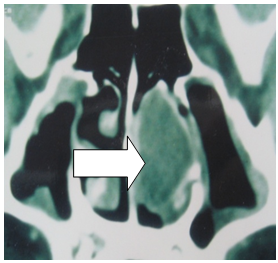 | Figure 2. CT scan picture showing cystic mass (arrow) arising from the lateral wall of the left nasal cavity |
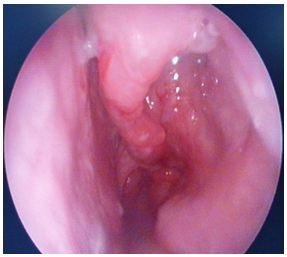 | Figure 3. Postoperative endoscopic picture (after three weeks) showing the left middle turbinate |
3. Discussion
- Concha bullosa is the pneumatisation of the middle turbinate and is one of the most common variations of the sinonasal anatomy. It may be cellular, or cystic. Enlargement of the middle turbinate can alter the nasal physiology, with disturbance in air-flow and obstruction to the natural drainage of the paranasal sinuses. This can result in facial pain or sinusitis [1, 3]. In the present case patient did not had any facial pain, sinusitis or epiphora.Mucoceles usually arise in the frontal or ethmoid sinuses, and these are well documented [4]. A pyocele occurs when a mucocele becomes infected. Review of literature showed only two reported cases of isolated pyocele of the middle turbinate [1, 2]. Initially an enlarging middle turbinate may be asymptomatic, because nasal cavity has a large empty space to fill before causing any symptoms. It should be distinguished from a neoplasia [2]. Cases of cholesteatoma of the concha bullosa presenting as cystic lesions of the middle turbinate, has been reported and it should be considered in the differential diagnosis [5]. Diagnostic nasal endoscopy and CT scan of nose and paranasal sinuses play a very important role in the management of these conditions. First case of pyocele of the middle turbinate was reported by Irwin and lesion was operated through lateral rhinotomy approach [1]. Second case was reported by Badia et al and lesion was operated through intranasal approach [2]. Our patient was operated through transnasal endoscopic approach. This is safe and gives good results.Pyocele of the middle turbinate is rare. An otolaryngologist should be familiar with this rare clinical entity. This is, to our knowledge, the third case of middle turbinate pyocele reported in the literature.