-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(3): 44-46
doi:10.5923/j.otolaryn.20170603.03

Acute Epiglottitis: Changing Trends
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShashikala BS, Borligegowda Viswanatha
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: We present our 10 years long experience on the clinical features and therapeutic management of acute epiglottitis. Patients and method: Fifty patients diagnosed as having acute epiglottitis, either by indirect laryngocopy, laryngoscopy, and radiological features on X-ray soft tissue neck (lateral view) were studied through a series of clinical parameters. Results: This study showed a male preponderance. Most common presenting complaints were dysphagia / odynophagia (90%). Dyspnoea was present in 10% of the cases. All the patients responded well to medical line of management. There was no complication or mortality. Conclusions: Acute epiglottitis usually presents with a sore throat. An awareness of this condition is essential for early diagnosis and prompt treatment, which will reduce the morbidity and mortality. Prior to the introduction of Haemophilus influenza type b vaccine, epiglottitis was common in paediatric age group. Now it is mainly seen in adults.
Keywords: Acute epiglottitis, Changing trends
Cite this paper: Shashikala BS, Borligegowda Viswanatha, Acute Epiglottitis: Changing Trends, Research in Otolaryngology, Vol. 6 No. 3, 2017, pp. 44-46. doi: 10.5923/j.otolaryn.20170603.03.
1. Introduction
- Epiglottitis is an infection of the supraglottic larynx. It is a potentially lethal condition if not recognized and treated promptly. Epiglottitis can lead to death by obstructing the upper airways. Prior to the introduction of Haemophilus influenza type b vaccine, epiglottitis was common in paediatric age group. After the introduction of the vaccine, it is seen mainly in adults. Severe sore throat and dysphagia with disproportionate signs of oropharyngeal inflammation was the main presenting picture [1].The most frequent aetiological agent is type B Haemophilus influenza. Other bacteria reported are Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumonia, Bacteroides melanogenicus and Mycobacterium tuberculosis [2, 3].Despite the decrease in the incidence of disease, epiglottitis should always be considered in the differential diagnosis in patients presenting with acute upper airway obstruction. This article will review the current presentation, evaluation, management of epiglottitis.
2. Material and Methods
- This prospective done on the cases of epiglottitis admitted during the last 10 years (January 2007 to December 2016). There were 50 patients comprising of 41 male and only 9 female patients. The age of those affected, ranged from 20 to 63 years old. The diagnosis of acute epiglottitis was made according to clinical criteria and laryngoscopic examination. All were submitted to a complete otolaryngological examination, X-ray soft tissue neck lateral view and bacteriological study.All the patients presented with a sore throat initially and presented within 48 hours after the onset of their symptoms of dysphagia/odonophagia, 45 patients were febrile and 5 patients had dyspnoea. None of 50 patients developed stridor or respiratory distress after admission. Rapid onset of dysphagia was the other predominant symptom. On examination inflammatory oedema of the epiglottis was present in all cases (fig 1), and associated lingual tonsillitis in 10 patients (fig 2).
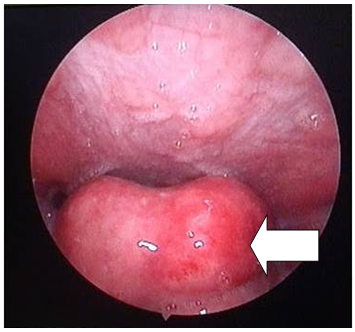 | Figure 1. Endoscopic picture showing swollen oedematous epiglottis |
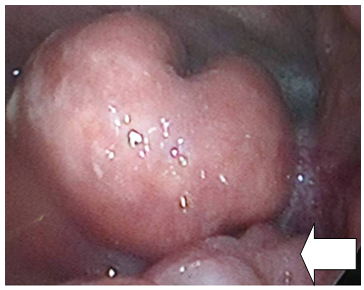 | Figure 2. Endoscopic picture showing swollen oedematous epiglottis & enlarged lingual tonsils |
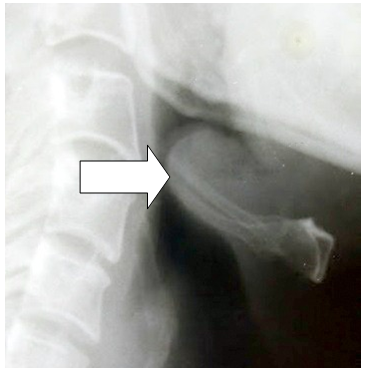 | Figure 3. Radiograph showing swollen oedematous epiglottis (Thumb sign) |
3. Discussion
- In the present study all the patients were in adult age group. There were no patients in the paediatric age group. Navarette et al observed a clear seasonal variation with the greatest frequency in autumn and summer. In November month there was highest number of cases [2]. However there was no seasonal variation in our study. All the patients presented with a sore throat initially and presented within 48 hours after the onset of their symptoms of dysphagia/odonophagia, 45 patients were febrile and 5 patients had dyspnoea. None of the 50 patients developed stridor or respiratory distress after admission. Rapid onset of dysphagia was the other predominant symptom. In earlier studies also dysphagia/odonophagia and fever were the common presenting symptoms [1-3]. In the present study, acute epiglottitis and lingual tonsillitis was also seen in 10 patients. Some earlier studies have also shown that in many cases of acute epiglottitis, lingual tonsillitis was present [2, 4, 5]. This may be due to the presence of rich lymphatic tissues in the periepiglottic tissues, hence inflammation can easily spread to the epiglottis [6]. The most frequent aetiological agent is type B Haemophilus influenza [2]. In the present study Haemophilus influenza was isolated in 10 cases.In some studies tracheostomy was carried out, where there was initial stridor and no response to the medical treatment [2, 7]. However in the present studies no such surgical interventions were required. Epiglottic abscess has been reported as a complication of epiglottitis [8]. In our study patients were treated with second generation cefotaxime or cefuroxime. There was no complication.In this study it was observed that:1. Acute epiglottitis was seen predominantly in adults.2. It responds well to medical line of management with higher antibiotics.3. Surgical airway intervention is usually not required, if treatment started early.4. If treated early, complications are rare.
4. Conclusions
- Acute epiglottitis is seen more commonly in adults. Acute epiglottitis in paediatric age group is rare, since the introduction of the conjugated Hib vaccine. Careful monitoring of the upper airway, empirical intravenous antibiotic and steroid therapy are important to reduce morbidity and mortality. The response to medical management is dramatic. Complications are rare.