-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(2): 27-29
doi:10.5923/j.otolaryn.20170602.03

Laryngeal Cysts in Children: A Prospective Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPrem Kumar P., Kumaraswamy K.
Department of Pediatric ENT, Indira Gandhi Institute of Child Health, Bangalore, India
Correspondence to: Prem Kumar P., Department of Pediatric ENT, Indira Gandhi Institute of Child Health, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

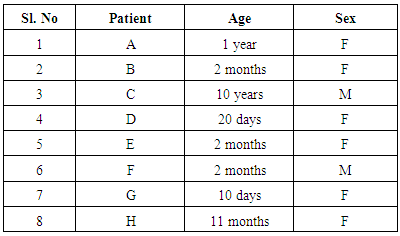
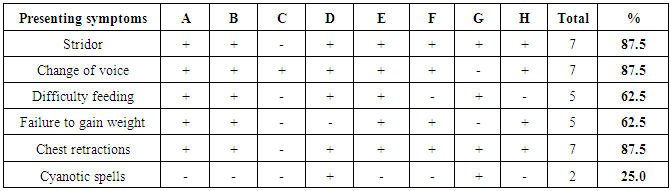
Objective: To understand the clinical features and surgical management of laryngeal cyst in children. Study design: A prospective, descriptive study. All cases of laryngeal cysts which were treated in the study period of 5 years (Jan 2012- Dec 2016) were included in this study. Materials and methods: All the cases of laryngeal cysts in children who presented to a tertiary care center were enrolled for the study. A total of 8 patients were enrolled for the study. Age of the children ranged from 10 days to 10 years. There were 2 male and 6 female children. A detailed history and examination revealed 87.5% of children presented with stridor, change of voice and chest retractions, 62.5% presented with difficulty swallowing and failure to gain weight, 25% presented with cyanotic spells. These children were subjected to detailed history and examination. All the children underwent direct laryngoscopy examination and diagnosis confirmed. Later all the patients underwent Endoscopic laryngeal excision of the cyst and they were followed up for 1 year for any complication and recurrence. Results: Post endoscopic surgery there were no complication and recurrence at the site of surgery. Conclusion: Laryngeal cysts in children are rare lesions which can present with stridor, change of voice, feeding difficulty and failure to thrive. These symptoms are non specific and may mimic other causes of laryngeal obstruction. Hence in all these cases a detailed work up and early intervention is pertinent to bring down mortality and morbidity.
Keywords: Laryngeal cyst, Stridor, Endoscopic cyst excision
Cite this paper: Prem Kumar P., Kumaraswamy K., Laryngeal Cysts in Children: A Prospective Study, Research in Otolaryngology, Vol. 6 No. 2, 2017, pp. 27-29. doi: 10.5923/j.otolaryn.20170602.03.
Article Outline
1. Introduction
- Laryngeal cysts in children are rare entities. They are located in the saccular appendage. They most commonly arise from between the arytenoid cartilage and the aryepiglottic fold with bulging into the rima glottis medially and pyriform sinus laterally. This location and extension commonly result in airway obstruction and severe stridor, a condition obligating prompt surgical intervention [3]. In 1970 De Santo classified laryngeal cysts into ductal and saccular. Ductal cysts results due to obstruction of the laryngeal epithelial mucous glands comprising 3/4th of all the laryngeal cysts. Saccular cysts are mucous retention in the laryngeal saccule resulting from obstruction or atresia of the laryngeal ventricle orifice. [1] These childrens present with stridor, change of voice, feeding difficulty, chest retractions and failure to thrive. They are diagnosed by direct laryngoscopy and mostly managed by endoscopic cyst excision with good success.In this prospective study, conducted at Pediatric ENT department in Indira Gandhi institute of child health from Jan 2012- Dec 2016, clinical evaluation and surgical management of laryngeal cysts in children are discussed.
2. Materials and Methods
- Study subjects were recruited from a tertiary care center over a 5 year period as part of the prospective study. All the children were in pediatric age group < 18yrs. These children were subjected to detailed history and examination. All the children underwent direct laryngoscopy examination under general anesthesia and diagnosis confirmed. All the 8 children diagnosed to have laryngeal cyst were electively posted for surgery under general anesthesia and a small size endotracheal tube was used to facilitate easy access.
|
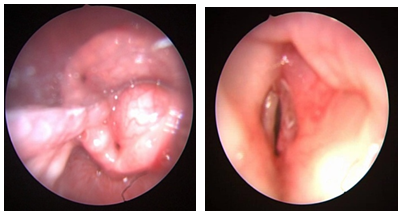 | Figure 1. (a) Laryngeal cyst – preoperative photograph (b) Laryngeal cyst – post-preoperative photograph |
3. Surgical Technique
- Under general anaesthesia a direct rigid laryngoscope was introduced to focus the laryngeal inlet. An assistant surgeon held the 0 degree hopkins rod. endoscope which was connected to a camera and displayed on a monitor. The endoscopic picture gave a good magnified view of the cyst. The cyst was held with a microlaryngeal cup forceps, retracted and a mucosal incision was made and the cyst was excised completely using micro laryngeal scissors including adjacent part of mucosa of the ventricle. Complete hemostasis was achieved. Post operatively all the children’s were put on antibiotics and injection Dexamethasone for 2 days.
4. Post Operative Results
- In all 8 children who underwent surgery postoperative period was uneventful without any complications. They were relieved of stridor and voice returned to normalcy. All patients were closely followed for 12 months and had no recurrence.One patient who was operated at 10 day of life for left laryngeal cyst had recurrence on right side for reasons unknown and was operated at 11 months of age and relieved of symptoms.
5. Discussion
- Laryngeal cysts in children are rare. They usually present with variable degree of airway obstruction, voice change and difficulty feeding which may prevent a baby from thriving. Congenital laryngeal cysts are rare with an annual incidence of 1.8 per 100,000 live births. [4] The severity of symptoms and timing of presentation of laryngeal cysts are related to the location and the size of the cysts. Smaller cysts presenting at birth produce less severe symptoms whereas larger cysts may present with life threatening airway obstruction requiring immediate intervention. [5]Children with laryngeal cysts typically present with inspiratory stridor. Stridor may be characteristic of a particular pathology, but it is never diagnostic. Stridor at birth is unusual and generally denotes a fixed congenital narrowing, such as a laryngeal web or subglottic stenosis. Dynamic conditions such as laryngomalacia and congenital vocal fold palsy become evident during the first few weeks of life. A gradual increase in the severity of stridor or airway compromise implies growth of an obstruction, such as in the case of a laryngeal cyst. The initial presentation of a laryngeal cyst may mimic laryngomalacia. In laryngomalacia there is no voice change whereas when the the cyst enlarges, the stridor may worsen and there may be voice changes associated with episodes of cyanosis, chest retractions and feeding difficulties.In our study 87.5% of children presented with Stridor, Change of voice and chest retractions, 62.5% presented with difficulty swallowing and failure to gain weight and 25% presented with cyanotic spells.These symptoms are nonspecific and mimic other laryngeal anomalies. Hence direct visualization of the cyst is important to establish diagnosis. This can be achieved by flexible bronchoscopy under local anesthesia but inadvertent head movement and abundant secretions in children may not allow good visualization for proper diagnosis [5, 6]. Direct laryngoscopy under general anesthesia gives good visualization of the cyst.
|
6. Conclusions
- Laryngeal cysts in children are rare lesions which can present with stridor, change of voice, feeding difficulty and failure to thrive. These symptoms are non specific and may mimic other causes of laryngeal obstruction. Hence in all these cases a detailed work up and early intervention is pertinent to bring down mortality and morbidity.