-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(2): 17-22
doi:10.5923/j.otolaryn.20170602.01

Comparison between Cold Dissection Snare Method and Bipolar Electrodissection Method in Tonsillectomy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAncy Anthony Vithayathil, Shreeharsha Maruvala, Ancy Anthony Vithayathil
Department of ENT, Al-Azhar Medical College and Superspeciality Hospital Thodupuzha, Ezhalloor Idukki Kerala
Correspondence to: Ancy Anthony Vithayathil, Department of ENT, Al-Azhar Medical College and Superspeciality Hospital Thodupuzha, Ezhalloor Idukki Kerala.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Tonsillectomy is one of the commonest surgical procedures performed in the field of Otorhinolaryngology. Over the last century many different procedures and techniques have been described, of which Cold Dissection-Snare method and Bipolar Electro dissection method are commonly used. The literature remains divided over which method is better. Objective: To compare Cold Dissection-Snare method and Bipolar Electro dissection method in tonsillectomy with respect to intraoperative blood loss and operative time taken. Materials and methods: Study is based on analysis of 40 patients aged between 5 to 40 yrs undergoing tonsillectomy in the Department of ENT at Meenakshi Medical College Hospital and Research Institute. Tonsillectomy is performed under general anaesthesia. Left sided tonsillectomies done by Bipolar Electro dissection and right side by Cold Dissection-Snare method, thus eliminating other potential influencing physiological factors. Amount of intraoperative blood loss is measured by calculating the difference in weight of swabs before and after use during surgery and then adding it to the total volume of blood collected in respective suction bottles. Operative time taken is also recorded. Result: Blood loss was significantly less with the Bipolar Electro dissection method (BED), averaging 47.13 ± 8.24ml compared to 52.23 ± 9.68 ml averaged in Cold Dissection Snare method in tonsillectomy. There was significant difference in operative time between both methods, 15.45 ± 3.93min on Bipolar Electro dissection side versus 18.03 ± 4.03 min on Cold Dissection-Snare side. Conclusion: In the present study, it was found that Bipolar Electro dissection was associated with a significant decrease in surgical time and intraoperative blood loss compared to the Cold Dissection-Snare method.
Keywords: Tonsillectomy, Electrocautery, Dissection snare, Electro dissection
Cite this paper: Ancy Anthony Vithayathil, Shreeharsha Maruvala, Ancy Anthony Vithayathil, Comparison between Cold Dissection Snare Method and Bipolar Electrodissection Method in Tonsillectomy, Research in Otolaryngology, Vol. 6 No. 2, 2017, pp. 17-22. doi: 10.5923/j.otolaryn.20170602.01.
Article Outline
1. Introduction
- Infectious and inflammatory diseases involving the tonsils account for a significant proportion of childhood illnesses and often result in tonsillectomy; one of the most common surgical procedures of childhood [1]. It’s probably the earliest described surgical intervention in Otorhinolaryngology. Tonsillectomy is performed by a variety of techniques [2]. These techniques have evolved over the years aiming to make the procedure safe and decrease the surgical time, intra operative blood loss, postoperative morbidity and complications [3]. It was not until the beginning of the twentieth century that Worthington [4] and Waugh [5, 6] described the modern technique of tonsillectomy by dissection. In 1968, Remington-Hobbs described the use of diathermy for removal of tonsils [7]. Despite the developments in techniques and technology, tonsillectomy still carries a relatively high risk of morbidity [8]. The two most commonly used techniques are Cold Dissection-Snare and Electro dissection. As a matter of fact, these are the mostly discussed techniques in the literature [2, 3, 9, 10, 11].This prospective study is to compare cold dissection-snare method of tonsillectomy with Bipolar Electro dissection method of tonsillectomy, in a group of 40 patients aged 5-40yrs at Meenakshi Medical College Hospital and Research Institute over a period of time from Sept 2011 – Sept 2013.
2. Materials and Methods
- This present study entitled “Comparison between Cold Dissection-Snare method and Bipolar Electro dissection method in tonsillectomy” is a prospective study conducted in Meenakshi Medical College & Research Institute in the year 2011-2013.Study is based on analysis of 40 patients aged between 5-40 years undergoing tonsillectomy in Department of ENT in Meenakshi Medical College Hospital and Research Institute. Each case after being screened from the outpatient department will undergo a general physical examination, local ENT, laboratory and radiological examination. Inclusion criteria:Ÿ Patients aged between 5 to 40 yrs with× Recurrent acute exacerbation of chronic tonsillitis (3-4 episodes for 2-3 yrs) and/or× Hypertrophied tonsils causing obstructive symptomsExclusion criteria:Ÿ Children suffering from tonsillitis of age less than 5 years. Ÿ Patients requiring adenoidectomy. Ÿ Underlying bleeding and clotting disorders. Ÿ Quinsy.Ÿ Pregnancy and lactation.Ÿ Submucous cleft palate.Ÿ Chronic systemic illnesses. Method of collection of dataŸ All the patients involved were explained in detail about the procedure and involvement in this study and a voluntary informed consent was obtained for the same.Ÿ After obtaining detailed history, a thorough local clinical examination of throat, ears, nose, and neck were done. A general examination was also done.Ÿ They were subjected to basic investigation for fitness of surgery under general anesthesia like Hb, TC, DC, ESR, BT, CT, Blood grouping and typing, Platelet count, aPTT, urine routine, HIV, HbSAg, ECG, Chest X-ray, X-ray Nasopharynx & X-ray P.N.S.Surgery was performed by the same surgeon. Under General Anaesthesia after oral/nasal endotracheal intubation, patient is positioned at the edge of the bed and a sand bag was applied between the shoulders to assume Rose’s Position. Boyle Davis mouth gag along with bipod stand was applied for adequate exposure of the oro-pharynx. A known quantity of saline (150 ml) was taken in the bowl and used for intermittent suction, to prevent blockage separately for each fossa.Right sided tonsillectomy was chosen for Cold Dissection-Snare method (CDS) (FIGURE 1) and left side for Bipolar Electro dissection (FIGURE 2). In this method per se patients became their own controls thus eliminating other potential influencing physiological factors.
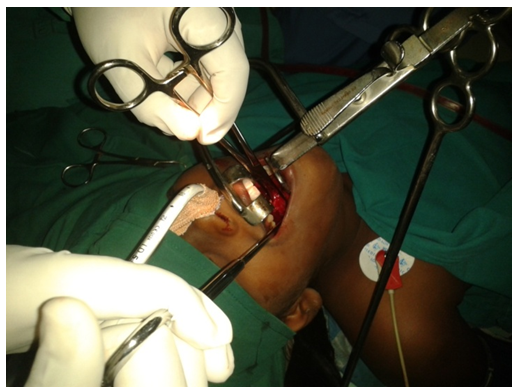 | Figure 1. Right Side Inferior Pedicle of Tonsil Being Snared |
 | Figure 2. Left Side Bipolar Electrodissection in Progress |
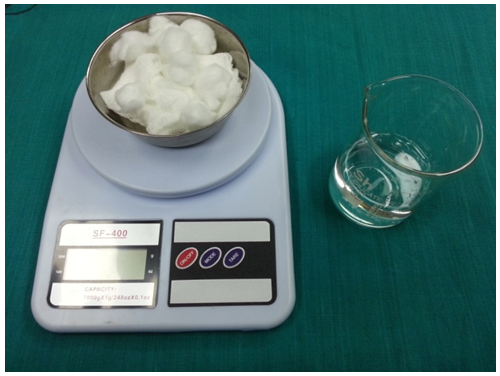 | Figure 3. Weighing Scale & Measuring Beaker |
3. Observations and Results
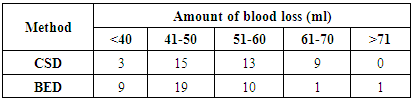
- The study showed maximum incidence of tonsillitis in the age group of 11-20 years (18 cases out of 40 cases studied) followed by the 5-10 years group. The study showed females had higher incidence of tonsillitis compared to males (57.5%).The incidence of presenting complaints in patients presenting with tonsillitis as well as the signs they presented with were analyzed.v Symptoms - Throat pain was the predominant presenting symptom in about 82.5 % of cases. The next common complaint was difficulty in swallowing in 72.5% of cases and 32.5% of cases had difficulty in breathing.v SIGNS- All cases had enlarged tonsils. 60% of cases on examination had enlargement of jugulo-digastric lymph nodes and 10% of cases had positive Erwin Moore sign.All cases presented with bilateral tonsillar enlargement. Majority (47.5%) presented with grade 2 tonsillar enlargement or tonsils occupying 25 to 50% of oropharynx .Median intra-operative blood loss was 47.13ml (SD 8.24) for Bipolar Electro-dissection tonsillectomy and 52.23ml (SD 9.68) for Cold Dissection-Snare tonsillectomy, P< 0.05.The median operative time was 15.45min (SD 3.93) for Bipolar Electro-Dissection tonsillectomy compared to 18.03min (SD 4.03) for the Cold Dissection-Snare method, P<0.05.All patients were asked about postoperative pain at 24 hours. There was no significant difference in postoperative pain on the first postoperative day between BED side and CDS side (i.e., 17.5% versus 10%) (p>0.05).There was no significant difference in postoperative bleeding between CDS side and BED side, only one case reported with secondary haemorrhage from left side (BED). (TABLE 1, GRAPH 1)
|
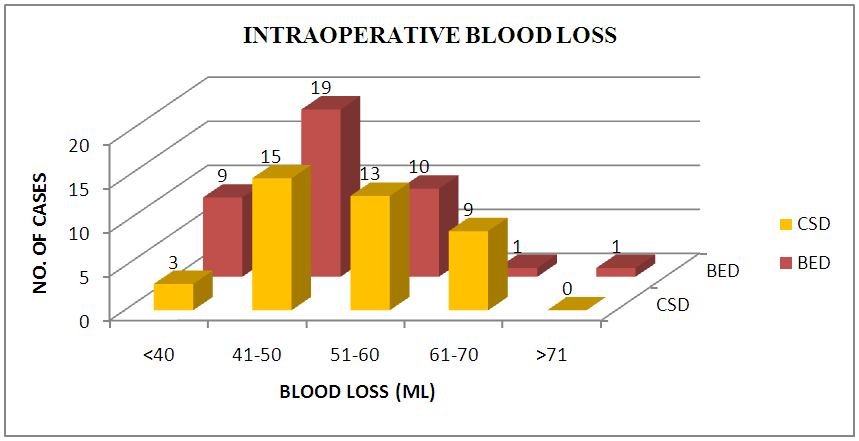 | Graph 1. Intraoperative Blood Loss – Comparison between CDS and BED Methods |
4. Discussion
- Tonsillectomy may be performed by different techniques [2] these techniques have evolved over the time with the objective of reducing the morbidity and complications associated with the procedure. All these techniques have advantages as well as drawbacks, as reported by the surgeons from time to time, but none of them has been accepted as the single best technique universally [15].Operating time, intra-operative blood loss, postoperative pain, return to normal diet and activity and secondary haemorrhage are the points of concern that have divided the surgeons between different techniques and are the objectives of clinical research going around globally.In the present study, the self-paired comparison between CDS and BED techniques reduced bias and increased precision of the study. Factors influencing the outcomes might not be equal in unpaired groups, such as age, tonsil size, and degree of infection, concomitant medication, hypertensive status, and surgical indication.A detailed study regarding the age and sex of the patients was done. The observations were tabulated. Maximum incidence of tonsillitis was in the age group of 11-20 years followed by the 5-10 years group, together accounting for 75% of cases. Females had higher incidence when compared to males (57.5%).The study showed that in the incidence of presenting complaints in patients presenting with tonsillitis throat pain was the predominant symptom in about 82.5 % of cases. The next common complaint was difficulty in swallowing in 72.5% of the cases which ranged from dysphagia to solids and liquids.All cases presented with bilateral tonsillar enlargement. Majority (47.5%) presented with grade ‘2’ tonsillar enlargement i.e., tonsils occupying 25 to 50% of oropharynx, 10% of the cases had positive Ervine Moore’s sign and 60% of cases on examination had enlargement of jugulo digastric lymph nodes bilateral. In this study, the operative time and intraoperative blood loss were found to be significantly less in the BED method. In a series of study by Blomgren et al. [16], on electrodissection tonsillectomy, they conclude that this technique was fast and resulted in little intraoperative bleed. Similar results were reported in many other studies by Pang [2], Silveira et al [11], Kirazli et al [17] & Raut et al [18, 19]. These findings may be attributed to the ability of diathermy to dissect the tonsils and coagulate the blood vessels simultaneously. In the present study intraoperative bleeding on both side showed a significant difference with the BED; averaging 47.13±8.24 ml compared to 52±9.68 ml for CDS tonsillectomy; (P<0.05). Mann et al [20], compared blood loss by electrocoagulation method versus dissection method in 95 patients, according to them average blood loss by hot method was markedly less, it was 11.8 ml and in cold it was 66.3 ml for each tonsil separately. In another study by Kousha et al the average amount of bleeding related to electrocautery tonsillectomy was 41.2 ± 2.46 ml and in cold dissection, tonsillectomy was 73.13 ± 3.37ml (P<0.05) [21]. Kujawski had a mean blood loss of 12 ml (SD 18 ml) in the diathermy group and 36 ml (SD 35 ml) in the dissection group [22] & Nunez found a mean blood loss of 15.1 ml (SD 11.7 ml) and 33.7 ml (SD 18.4 ml), respectively [23]. The literature on the subject by Trent [24], Atallah et al [9] & Leach et al [25] also supports the present study. In our study there was significant difference in operative time between both sides 15.45min (±3.93) in BED side versus 18.03min (±4.03) on CDS side, (P<0.05). Similar observation was seen in the study by Kousha et al [21] whose mean time of operation was 9.1 ± 0.39 minutes and 15.11 ± 0.65 respectively (P<0.05). There was no difference in the mean operating time between the two groups in a study by Kujawski (36.9 minutes for diathermy and 35.9 minutes for dissection) [22]. Similar findings were seen in studies by Lassaletta et al [26], Weimert TA et al [27], Roy A et al [28] and Pizzuto MP et al [29]. There are studies pointing to an opposite direction done by Szermetaw [30] and Watson M G [31].Pain is a very difficult response to study, as it is a highly subjective symptom with significant person to person variability. Our study design enabled an effective comparative assessment of pain by using the patient as his or her own control thus eliminating inter personal pain threshold. There was no significant difference in postoperative pain on the first postoperative day in the diathermy group compared to the cold dissection group (17.5% versus 10%) (p>0.05). Higher pain scores have been reported with electrodissection in studies done by Gendy S et al [3] and Atallah et al [9]. Increased pain reported with electrodissection could possibly be on account of various factors like experience with the technique, length of disease, amount of energy used during the procedure etc rather than the modality alone. Cardozo AA and colleagues have noted statistically significant positive relationship between the total amount of bipolar diathermy used and postoperative pain [32]. Still in another study by Atallah et al an increase in pain and a related prolongation of oral intake time in the postoperative period in bipolar cautery tonsillectomy group was found [9]. Increase in post operative pain in intensity and duration in bipolar diathermy cases; was also observed by Sood et al [33] and Me Gregor et al [34].One cases of secondary haemorrhage was seen in our study from the BED side, which settled with conservative medical treatment. Pang YT has reported incidence of postoperative haemorrhage as 1.7% with bipolar diathermy tonsillectomy compared to 3.4% with cold dissection, carrying no statistical significance [2]. Stephen O'Leary et al in his study reported that the difference in the risk of bleeding after dissection and diathermy tonsillectomy did not reach statistical significance [35]. Whereas Gendy S and colleagues have reported a higher incidence of secondary haemorrhage with bipolar dissection (2.3%) compared to cold dissection (1%) in a study including 545 children [3]. Similarly Lowe D et al after conducting a prospective national audit concluded that hot tonsillectomy techniques are associated with substantially high risk of secondary haemorrhage [36]. Increase in post operative haemorrhage has also been reported by Tay H L [37], Raut et al [19], Mann et al [20] and Weimert et al [38]. One explanation for higher post‐tonsillectomy bleeding rates after diathermy techniques may be related to greater thermal damage as the result of excessively high power settings or excessively frequent or prolonged application of diathermy [16].Limitations of the study1. Inflammable anaesthetic gases such as ether cannot be used along with bipolar diathermy.2. Weighing errors due to environmental factors like airflow in Operation Theater. 3. Methods for calculating weight contributed by secretions of upper airway during the surgery needs more research in future studies.
5. Conclusions
- Out of many available techniques for the tonsillectomy cold dissection and snare method and electrocautery methods are the most followed ones and there is significantly less blood loss in the electrocautery method of tonsillectomy. And with other parameters of comparison like operative time, post operative pains and bleeding electrocautery stands higher in position.