-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(1): 6-9
doi:10.5923/j.otolaryn.20170601.02

Sensorineural Hearing Loss in Mucosal and Squamous Type of Chronic Otitis Media - A Prospective Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDeepthi Padmanabhan, Borligegowda Viswanatha, Anil Kumar Ramabhadraiah, Maliyappanahalli Siddappa Vijayashree, Shambulinga Killera
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic otitis media is a chronic inflammation of the mucoperiosteal lining of the middle ear cleft. It is the commonest cause of hearing impairment which can be prevented, the prevalence being 72 per 1,000 population. Materials and Method: This study was conducted in 50 patients visiting the outpatient and inpatients department of Sri Venkateshwara ENT institute, Department of Otolaryngology, Bangalore Medical College and Research Institute. Detailed otologic history, clinical and audiometric findings were recorded and analysed. Results: 25 patients of each mucosal and squamous type of CSOM were included in the study. The prevalence of SNHL in mucosal group was found to be 12% and in squamous 36%. A statistically significant correlation was noted between the duration of disease and the bone conduction thresholds (p = 0.005) and also between the presence of cholesteatoma and SNHL (p= 0.029). No significant relation was noted among the gender, age of the patient, side of ear affected and BC thresholds in this study. Conclusion: SNHL, although a well documented complication of squamous CSOM, can occur following mucosal disease. Presence of cholesteatoma increased the likelihood of the patient having a higher BC threshold. The degree of SNHL was found to be dependent on the duration of disease, hence prompt and timely treatment can decrease the incidence of this sequel.
Keywords: Sensorineural hearing loss, Mucosal type otitis media, Squamous type otitis media
Cite this paper: Deepthi Padmanabhan, Borligegowda Viswanatha, Anil Kumar Ramabhadraiah, Maliyappanahalli Siddappa Vijayashree, Shambulinga Killera, Sensorineural Hearing Loss in Mucosal and Squamous Type of Chronic Otitis Media - A Prospective Study, Research in Otolaryngology, Vol. 6 No. 1, 2017, pp. 6-9. doi: 10.5923/j.otolaryn.20170601.02.
Article Outline
1. Introduction
- Chronic suppurative otitis media (CSOM) has assumed a world-wide importance. In the developing countries, it has continued to constitute a heavy disease burden, with the prevalence of chronic ear infections being up to 72 cases per 1,000 inhabitants [1, 2]. The diagnosis of chronic otitis media (COM) implies a permanent abnormality of the pars tensa or flaccida; most likely as a result of earlier acute otitis media, negative middle ear pressure or otitis media with effusion [3]. A considerable difference in the prevalence rate of COM is evident between developed and developing countries. Various studies shows prevalence of CSOM in India to range from 2 – 15 %. In a study by bluestone, India was considered to have a low prevalence of 2%, where as a study by Varma et al from Haryana showed it as high as 15.3% [4].One of the main consequences of COM is hearing loss. 80% of the people with COM, present with hearing loss. It is calculated that about 13.8 - 36.2% of the people have hearing impairment due to COM [5, 6]. It has been suggested that toxins in COM can damage the cochlea. The presence of SNHL has been ascribed to contribution of the middle ear in hearing mechanism by bone conduction which is also known as Carhart’s effect and/or cochlear damage resulting from extension of the inflammation in the middle ear cleft through round window membrane [7]. Paparella et al. in their research found that the toxin cross the round window membrane and cause irreversible cochlear hair cell loss mostly affecting the basal turn of the cochlea [8].The chronic inflammation on the round window membrane causes vasodilatation and vasoconstriction of the vessels and thereby causing circulatory disturbances leading to negative influential role on inner ear. Sensorineural hearing loss may also result from the treatment of active COM with potentially ototoxic eardrops, but most practicing otolaryngologists regard this as rare, probably at least as rare as sensorineural hearing loss due to the disease. In a retrospective study conducted by Alexandre et al. to study the incidence of SNHL in chronic suppurative otitis media and its association with cholesteatoma of the 115 patients analysed, SNHL was seen in 13% of the cases. But did not show a statistically significant association with the presence of cholesteatoma or duration of the ear disease [1].Another study by Rohit et al. conducted in 100 patients with unilateral CSOM, 28% had atticoantral type of disease and 72% had tubotympanic disease. The mean BC threshold in the CSOM group was found to be 15.03 dB and in control group 12 dB, this difference was found to be statistically significant. The degree of SNHL did not bear any correlation with the duration of discharge [9].The association between chronic otitis media and sensorineural hearing loss has been a broadly studied topic and yet there is controversy regarding its correlation with age of the patient and duration of otorrhea. The aim of this study is to analyse association between sensorineural hearing loss and chronic otitis media and its correlation with mucosal and squamous type of chronic otitis media.
2. Materials and Method
- This was a comparative study conducted at Sri Venkateshwara ENT Institute, Department Of Otolaryngology, Bangalore Medical College and Research Institute, during the period December 2015 to December 2016. A total of 50 patients who fulfilled the following criteria were included in the study,1. Patients willing to give informed written consent.2. Patients with age above 16 years.3. Patients with unilateral chronic suppurative otitis media.All patients with age above 60 years, family history of congenital / acquired Sensorineural hearing loss, history of use of ototoxic drugs (systemic or local), prior history of ear surgery, history of noise exposure and history of head injury were excluded from the study.A detailed history was obtained from the patients including ear discharge (onset, frequency, duration, etc.), vertigo, hearing loss, tinnitus, headache, etc. detailed clinical and otological examination was done. Presence of otorrhea, site and size of perforation, ossicular disruption and presence of cholesteatoma were noted. Tuning fork tests that included Weber’s, Rinne’s and Absolute Bone Conduction test were done. All patients were subjected to pure tone audiometry in a semi sound attenuated room. A narrow band noise was given to the other ear for masking.
3. Data Analysis
- For the purpose of analysis, all patients were grouped into two, namely Group A – CSOM safe type and Group B-CSOM unsafe type. The Average bone conduction thresholds for the frequencies 0.5, 1, 2 and 4 kHz were taken as the sensorineural component. BC threshold above 25 dB was considered as SNHL. Data analysis was done with IBM SPSS Statistics 21 software.
4. Results
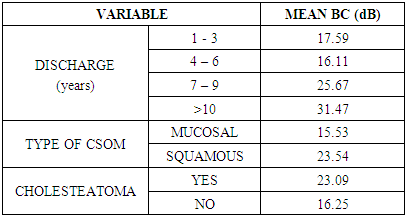
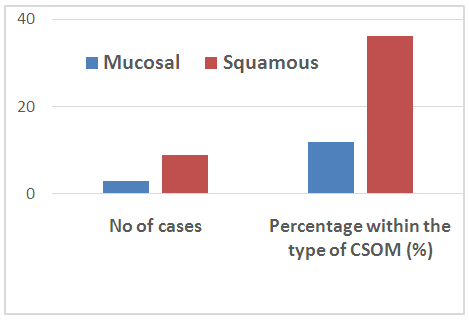
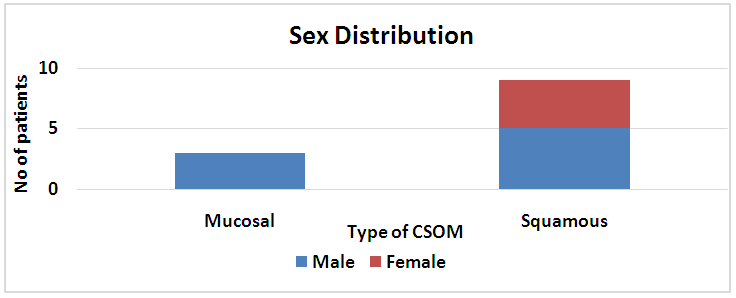
- The age of the subjects included in the study ranged from 16 to 60 years, with mean age 41.46. 34 (68%) males and 16 (32%) females were included in this study. 3 patients with mucosal type of CSOM had sensorineural hearing loss, the prevalence being 12%. The prevalence of sensorineural hearing loss in squamous type of CSOM was found to be 36% (Table 1).
|
 | Graph 1. Prevalence of SNHL |
 | Graph 2. Distribution of type of CSOM |
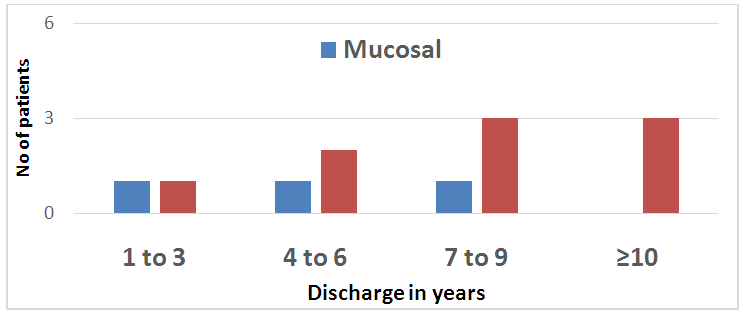 | Graph 3. Patient distribution for discharge in years for types of CSOM |
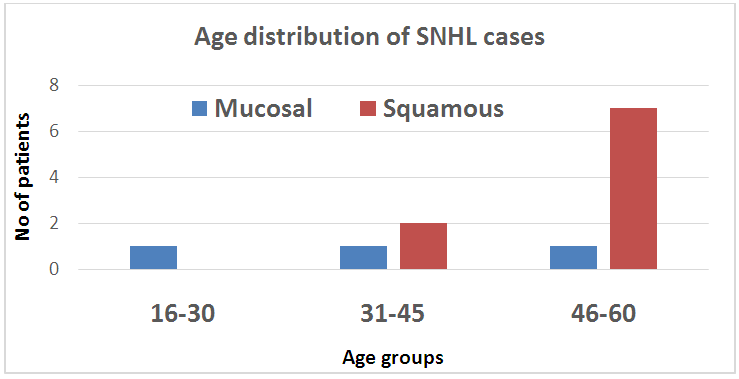 | Graph 4. Patient distribution for SNHL cases |
5. Discussion
- Conventionally, a conductive hearing loss is expected in a patient suffering from CSOM. Occasionally, elevated BC thresholds have been observed in various audiometric recordings in patients suffering from CSOM indicating a sensorineural (SN) element [9]. The mechanism for the occurrence of SNHL has been studied by many researchers. One study mentioned that cochlear damage in patients with COM might be due to bacterial toxins that diffuse through the round window membrane. These toxins might then cause damage to the hair cells especially those at the cochlear base; the reason why high frequency sounds are more affected [10-13]. In this study we tried to assess the relation of SNHL with various parameters like age, side of disease, duration of symptoms and presence of cholesteatoma. A comparative analysis between mucosal and squamous type of CSOM was also done.In our study it was observed that 46% of the population with squamous CSOM had cholesteatoma, a higher BC threshold was noted among patients with cholesteatoma. Study by Sharma et al [9] stated that chronic otitis media with cholesteatoma appears to be associated with greater sensorineural hearing loss but it was not statistically significant. In a similar study conducted by Handa et al [14] it was found that a significant relation was found between BC threshold and discharge.We also observed an elevated mean BC threshold in presence of cholesteatoma which are consistent with other studies [2, 15, 16, 17]. Cholesteatoma has an erosive nature. As the cholesteatoma contacts bone, normal mucosal lining degenerates and inflammatory mediators such as macrophages, monocytes and osteocytes begin to appear [16]. The round window membrane has a semipermeable nature, many toxins diffuse through this membrane leading to damage to inner hair cells. Cholesteatoma also causes erosion of the otic capsule which further facilitates this diffusion.In this study larger numbers of patients were noted to have higher BC thresholds as the duration of ear discharge increased, it was found to be a significant relationship. Similar results were noted by Azevado et al [1] and Chatterji P et al [2].
6. Conclusions
- The prevalence of SNHL was found to be higher (36%) in squamous than in the mucosal group (12%). Thus SNHL can occur as a sequel of both mucosal and squamous type of CSOM. Presence of cholesteatoma increased the likelihood of the patient having a higher BC threshold. The degree of SNHL was found to be dependent on the duration of disease, hence prompt and timely treatment the condition can decrease the incidence of this sequel.